Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- We AreДокумент2 страницыWe ArePradila Desty SariОценок пока нет
- WordddДокумент1 страницаWordddPradila Desty SariОценок пока нет
- 701029Документ6 страниц701029Pradila Desty SariОценок пока нет
- DapusДокумент1 страницаDapusPradila Desty SariОценок пока нет
- DapusДокумент1 страницаDapusPradila Desty SariОценок пока нет
- KJKJKJДокумент1 страницаKJKJKJPradila Desty SariОценок пока нет
- DapusДокумент1 страницаDapusPradila Desty SariОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- MEDICINEДокумент20 страницMEDICINEMwanza Kabachele HenryОценок пока нет
- ALLHAT Journal ClubДокумент3 страницыALLHAT Journal ClubcvariableОценок пока нет
- Blood Pressure Control InType 2 DiabetesДокумент119 страницBlood Pressure Control InType 2 Diabetesjourey08Оценок пока нет
- sglt2 Inhibition PDFДокумент11 страницsglt2 Inhibition PDFNarinder SharmaОценок пока нет
- Hypertension Management GuidelineДокумент11 страницHypertension Management GuidelineAdeNeaОценок пока нет
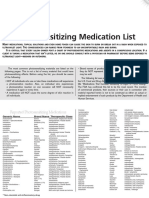
- Photosensitizing Medication ListДокумент3 страницыPhotosensitizing Medication ListDimas RfОценок пока нет
- Towards Better Patient Care Drugs To Avoid in 2020Документ10 страницTowards Better Patient Care Drugs To Avoid in 2020AlvaroОценок пока нет
- Baharudin Et Al 2023 Factors Associated With Achievement of Blood Pressure Low Density Lipoprotein Cholesterol LDL CДокумент13 страницBaharudin Et Al 2023 Factors Associated With Achievement of Blood Pressure Low Density Lipoprotein Cholesterol LDL CFifi RetiatyОценок пока нет
- ADR PharmacologyДокумент30 страницADR PharmacologySumanth Kumar ReddyОценок пока нет
- Beyond Traditional Methods: Facile Multicomponent Reactions As Cornerstones of Drug DevelopmentДокумент39 страницBeyond Traditional Methods: Facile Multicomponent Reactions As Cornerstones of Drug DevelopmentInternational Journal of Innovative Science and Research TechnologyОценок пока нет
- Hypertension Topic DiscussionДокумент13 страницHypertension Topic Discussionapi-665372449Оценок пока нет
- Postdialysis Hypertension: Associated Factors, Patient Profiles, and Cardiovascular MortalityДокумент6 страницPostdialysis Hypertension: Associated Factors, Patient Profiles, and Cardiovascular MortalityLaura PutriОценок пока нет
- Aldomet: (Methyldopa)Документ6 страницAldomet: (Methyldopa)Riska AuliahОценок пока нет
- Canadian Guidelines 2018Документ6 страницCanadian Guidelines 2018Eduardo JiménezОценок пока нет
- Ilmu Penyakit Dalam: BagianДокумент48 страницIlmu Penyakit Dalam: BagianRoberto SoehartonoОценок пока нет
- Methyldopa Drug StudyДокумент2 страницыMethyldopa Drug StudyBea Dela Cena100% (1)
- Case StudiesДокумент5 страницCase Studiespragna novaОценок пока нет
- HTN and Arrh AfzalДокумент8 страницHTN and Arrh AfzalAFA.BLSОценок пока нет
- Turkey BK 2013 - Full VersionДокумент147 страницTurkey BK 2013 - Full VersionmmmmzОценок пока нет
- Pharma 10 Years-1Документ15 страницPharma 10 Years-1Dheeraj Garg100% (1)
- Anti Hypertensive DrugsДокумент113 страницAnti Hypertensive DrugsRobert DowneyОценок пока нет
- Pharmaceutical CareДокумент114 страницPharmaceutical CareRisdaFitriaОценок пока нет
- Advanced Pharmacology Module 4 DiscussionДокумент3 страницыAdvanced Pharmacology Module 4 Discussionapi-634345342Оценок пока нет
- Pcol Cover To CoverДокумент214 страницPcol Cover To CoverJec OcampoОценок пока нет
- Eddy Wirawan, SPJP - Fiha: Rsud. Ulin BanjarmasinДокумент49 страницEddy Wirawan, SPJP - Fiha: Rsud. Ulin Banjarmasineka febriantyОценок пока нет
- Strategies For Dementia Prevention: Latest Evidence and ImplicationsДокумент16 страницStrategies For Dementia Prevention: Latest Evidence and ImplicationsRitmaОценок пока нет
- Oleh: Bagian Ilmu Penyakit Dalam FK Universitas Sultan Agung Semarang 2012Документ40 страницOleh: Bagian Ilmu Penyakit Dalam FK Universitas Sultan Agung Semarang 2012Mbenk NjoeОценок пока нет
- Hypertensive Emergencies in The Emergency DepartmentДокумент13 страницHypertensive Emergencies in The Emergency DepartmentLuis Lopez RevelesОценок пока нет
- Saudi Health ExamДокумент90 страницSaudi Health ExamJafar AP100% (2)
- Prescribing For The ElderlyДокумент8 страницPrescribing For The ElderlykarladeyОценок пока нет