Вам также может понравиться
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Theragran (Multiple Vitamins)Документ3 страницыTheragran (Multiple Vitamins)Adrianne BazoОценок пока нет
- Tugas 1 Writing 4-Bing4309Документ1 страницаTugas 1 Writing 4-Bing4309DitaSariKusumaОценок пока нет
- What Is A PsychiatristДокумент2 страницыWhat Is A Psychiatristmercy robinsonОценок пока нет
- DSM 5 - DSM 5Документ7 страницDSM 5 - DSM 5Roxana ClsОценок пока нет
- Benefits of HijamaДокумент3 страницыBenefits of HijamaBateria MeaОценок пока нет
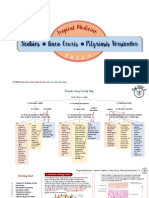
- Scabies Tinea Cruris Pityriasis Versicolor: Semangat!Документ11 страницScabies Tinea Cruris Pityriasis Versicolor: Semangat!Fitriah Nur SyamiatiОценок пока нет
- Reference: Maglumi TSH (Clia)Документ5 страницReference: Maglumi TSH (Clia)Lidia NarbОценок пока нет
- Licensing Officer ResumeДокумент4 страницыLicensing Officer ResumeShairaCerenoОценок пока нет
- Clinical Psychology Notes No. 1Документ2 страницыClinical Psychology Notes No. 1Jerine Bonus ApostolОценок пока нет
- Cerebrovit X-CelДокумент36 страницCerebrovit X-CelzuzuzazaziziОценок пока нет
- Faculty List2019Документ6 страницFaculty List2019suyashsahu2505Оценок пока нет
- Journal Reading: Stase Ilmu THT RS Umum Daerah Sayang Cianjur Universitas Muhammadiyah Jakarta 2019Документ15 страницJournal Reading: Stase Ilmu THT RS Umum Daerah Sayang Cianjur Universitas Muhammadiyah Jakarta 2019dwi purwantiОценок пока нет
- Filarial Worm: Richard David Silvestre, RMT, MSMT 9 C 0Документ13 страницFilarial Worm: Richard David Silvestre, RMT, MSMT 9 C 0Hearts heavy Moms spaghettiОценок пока нет
- Anesthesia For Cardiac Surgery - General Principles - UpToDateДокумент58 страницAnesthesia For Cardiac Surgery - General Principles - UpToDateEvoluciones MedicinaОценок пока нет
- Double Stimulations During The Follicular and Luteal Phases of Poor Responders in IVF/ICSI Programmes (Shanghai Protocol)Документ8 страницDouble Stimulations During The Follicular and Luteal Phases of Poor Responders in IVF/ICSI Programmes (Shanghai Protocol)Nirmal KumawatОценок пока нет
- Core Surgical Training CT1 Person SpecificationsДокумент10 страницCore Surgical Training CT1 Person SpecificationsRajin MaahiОценок пока нет
- Braden Q Scale PDFДокумент1 страницаBraden Q Scale PDFSri NiningОценок пока нет
- Art Therapy What Is Art Therapy?Документ2 страницыArt Therapy What Is Art Therapy?rohit singhОценок пока нет
- Antimicrobial Peptides Under Clinical InvestigationДокумент15 страницAntimicrobial Peptides Under Clinical InvestigationEsteban MalamboОценок пока нет
- Analisis Kesesuaian Penggunaan Antiinfeksi Pada Infeksi Oportunistik Pasien Hiv/Aids Rawat Inap Di Rsup Dr. Sardjito YogyakartaДокумент7 страницAnalisis Kesesuaian Penggunaan Antiinfeksi Pada Infeksi Oportunistik Pasien Hiv/Aids Rawat Inap Di Rsup Dr. Sardjito YogyakartaindahОценок пока нет
- Summative 2 Renal 2011Документ8 страницSummative 2 Renal 2011Ike Annisa YuwelzaОценок пока нет
- PHSW CME Sedation Answer KeyДокумент10 страницPHSW CME Sedation Answer Keyعلي صادق جعفرОценок пока нет
- Headache: Differential Diagnosis of HeadacheДокумент139 страницHeadache: Differential Diagnosis of Headachemero1983Оценок пока нет
- 20 OncoДокумент115 страниц20 OncomichelleОценок пока нет
- Research Project ProposalДокумент8 страницResearch Project ProposalAthena Irish LastimosaОценок пока нет
- Bayabas: Instructions For GuavaДокумент2 страницыBayabas: Instructions For GuavadorothypearlОценок пока нет
- Department of Clinical Medicine and SurgeryДокумент2 страницыDepartment of Clinical Medicine and SurgeryBonface KenaniОценок пока нет
- 3-Ammar Notes (Ob - Gyn)Документ6 страниц3-Ammar Notes (Ob - Gyn)Dr-Hashem Al-ShareefОценок пока нет
- Hepatitis EДокумент7 страницHepatitis EmdОценок пока нет
- Hypertention and HypotentionДокумент46 страницHypertention and HypotentionAmanuel MaruОценок пока нет