Вам также может понравиться
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Robin Murphy - Coronavirus - Webinar - 01Документ78 страницRobin Murphy - Coronavirus - Webinar - 01lasti kurnia100% (5)
- Toxoplasma GondiiДокумент29 страницToxoplasma GondiiNagalingaОценок пока нет
- Extensive Research Proves Vaccines Are DeadlyДокумент70 страницExtensive Research Proves Vaccines Are DeadlyVigilantCitizen100% (5)
- Microbial Diseases of The Respiratory SystemДокумент30 страницMicrobial Diseases of The Respiratory SystemChristopher Eria Santiañez0% (1)
- Community Health Nursing QuizДокумент3 страницыCommunity Health Nursing QuizhemihemaОценок пока нет
- Laporan Evaluasi Tahunan 2022Документ40 страницLaporan Evaluasi Tahunan 2022Stevy MardLianyОценок пока нет
- CertificateДокумент1 страницаCertificateEkta WaykarОценок пока нет
- TB Case StudyДокумент2 страницыTB Case StudyReisabelle LabianoОценок пока нет
- Diseases and Mosquito Biology ProjectДокумент8 страницDiseases and Mosquito Biology ProjectCurnel MilletteОценок пока нет
- Department of Genetics: Covid-19 RT PCRДокумент1 страницаDepartment of Genetics: Covid-19 RT PCRDv RasminaОценок пока нет
- Enterobacteriaceae ManualДокумент1 страницаEnterobacteriaceae ManualMukhtiar AliОценок пока нет
- Deterministic Malaria Transmission Model With Acquired ImmunityДокумент6 страницDeterministic Malaria Transmission Model With Acquired ImmunityAchmad Nur AlphiantoОценок пока нет
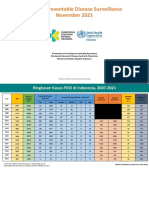
- 11 - VPD Surveillance Performance Analysis 2021 November 2021 (29122021)Документ57 страниц11 - VPD Surveillance Performance Analysis 2021 November 2021 (29122021)Kiky RizkyОценок пока нет
- S2-Epid - Main Disese (3) - Influenza - Student - 2023Документ48 страницS2-Epid - Main Disese (3) - Influenza - Student - 2023Syahrul SanmasОценок пока нет
- Spirochetes: Pantyo V., PHD Department of Microbiology, Virology, Epidemiology With Course of Infectious DiseasesДокумент29 страницSpirochetes: Pantyo V., PHD Department of Microbiology, Virology, Epidemiology With Course of Infectious DiseasesVivek Chaudhary100% (1)
- Laporan-Diagnosa DesemberДокумент421 страницаLaporan-Diagnosa DesemberPutri Annisa0% (1)
- Principles of Epidemiology in Public Health Practice-412-469Документ58 страницPrinciples of Epidemiology in Public Health Practice-412-469Dehnzel de LeonОценок пока нет
- dm2021 0327 Surge Response Plan For HFДокумент11 страницdm2021 0327 Surge Response Plan For HFMonica Lowinski100% (1)
- Schistosoma Haematobium: Chisto/copulating - Schistosomes - GifДокумент8 страницSchistosoma Haematobium: Chisto/copulating - Schistosomes - GifTinОценок пока нет
- Drugs For Parasitic Infections 2013 PDFДокумент31 страницаDrugs For Parasitic Infections 2013 PDFMichael FreudigerОценок пока нет
- WB DHFW Bulletin 4TH MAY FINAL PDFДокумент3 страницыWB DHFW Bulletin 4TH MAY FINAL PDFVishalBeheraОценок пока нет
- Immunologic Study of StreptolysinДокумент12 страницImmunologic Study of StreptolysinAishwarya BharathОценок пока нет
- Frankenmuth Disease Detective Test 2014 Answer KeyДокумент18 страницFrankenmuth Disease Detective Test 2014 Answer KeyOjasw UpadhyayОценок пока нет
- BHERT Pocket Guide Ver04Документ96 страницBHERT Pocket Guide Ver04easyasqweОценок пока нет
- Astudillo V Dr. Pierre-Claude Poulin, PédiatreДокумент4 страницыAstudillo V Dr. Pierre-Claude Poulin, PédiatreAl StatiliusОценок пока нет
- Catálogo Fast Track 2017Документ10 страницCatálogo Fast Track 2017rolan.olivaresОценок пока нет
- National Service Training Program: "Reaction Paper"Документ4 страницыNational Service Training Program: "Reaction Paper"Stefanny Anne GuminangОценок пока нет
- NP1 BulletsДокумент17 страницNP1 BulletsJea VesagasОценок пока нет
- CandidiasisДокумент6 страницCandidiasisNabrazz SthaОценок пока нет
- Pinta (Tropical Syphilis)Документ17 страницPinta (Tropical Syphilis)Aiman Tymer100% (1)