Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Eighteenth Century in India - S AlviДокумент62 страницыThe Eighteenth Century in India - S Alvishubham sharma100% (2)
- 21 Indispensable Qualities of A Leader - John Maxwell (Presentation)Документ23 страницы21 Indispensable Qualities of A Leader - John Maxwell (Presentation)Le Po100% (1)
- The 21 Indispensable Qualities of A LeaderДокумент5 страницThe 21 Indispensable Qualities of A LeaderAmirhosein605334Оценок пока нет
- 467 PDFДокумент11 страниц467 PDFiqbalОценок пока нет
- Review ArticleДокумент12 страницReview ArticleBarbie Nurdilia RОценок пока нет
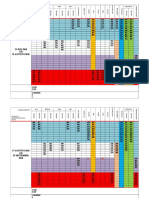
- Timeline ANOM FDMДокумент4 страницыTimeline ANOM FDMiqbalОценок пока нет
- Jadwal SweepingДокумент2 страницыJadwal SweepingiqbalОценок пока нет
- 467 PDFДокумент11 страниц467 PDFiqbalОценок пока нет
- Gejala Klinis:, Et Al. (Online) (CitedДокумент1 страницаGejala Klinis:, Et Al. (Online) (CitediqbalОценок пока нет
- Jcdsa20120300010 79060760Документ5 страницJcdsa20120300010 79060760iqbalОценок пока нет
- Cancer Skin Cancer IndonesianДокумент9 страницCancer Skin Cancer Indonesiandhedhe47Оценок пока нет
- Rollingan 22 Maret 2018 BaruДокумент19 страницRollingan 22 Maret 2018 BaruiqbalОценок пока нет
- Persiapan AnomДокумент3 страницыPersiapan AnomiqbalОценок пока нет
- Left Ventricular Aneurysm Is14Документ2 страницыLeft Ventricular Aneurysm Is14iqbalОценок пока нет
- Brochure TN 322Документ1 страницаBrochure TN 322iqbalОценок пока нет
- 2015 Stratigos EurGuidelineSCC EJCДокумент19 страниц2015 Stratigos EurGuidelineSCC EJCiqbalОценок пока нет
- Persiapan AnomДокумент3 страницыPersiapan AnomiqbalОценок пока нет
- Daftar Harga Suku Cadang Honda CBR 150 Honda Genuine Part (HGP)Документ25 страницDaftar Harga Suku Cadang Honda CBR 150 Honda Genuine Part (HGP)mbahlanhОценок пока нет
- 721 jmm067611Документ8 страниц721 jmm067611iqbalОценок пока нет
- SimcityДокумент1 страницаSimcityiqbalОценок пока нет
- Lee - Bactericidal Effect of PterostilbeneДокумент12 страницLee - Bactericidal Effect of PterostilbeneiqbalОценок пока нет
- Cbr150r - List Spare Parts HandbookДокумент150 страницCbr150r - List Spare Parts HandbookwidhiantoОценок пока нет
- Peran Tenaga Kesehatan Sebagai Pelaksana Pelayanan Pelayanan Kesehatan PuskesmasДокумент9 страницPeran Tenaga Kesehatan Sebagai Pelaksana Pelayanan Pelayanan Kesehatan PuskesmasIntar TeaОценок пока нет
- Daftar Harga Suku Cadang Honda CBR 150 Honda Genuine Part (HGP)Документ25 страницDaftar Harga Suku Cadang Honda CBR 150 Honda Genuine Part (HGP)mbahlanhОценок пока нет
- 721 jmm067611Документ8 страниц721 jmm067611iqbalОценок пока нет
- Ijcep0005 0231 PDFДокумент12 страницIjcep0005 0231 PDFiqbalОценок пока нет
- RockhillДокумент7 страницRockhillAnthie FitriОценок пока нет
- Ihk SodДокумент8 страницIhk SodrynaldiandriansyaОценок пока нет
- Full DPДокумент12 страницFull DPiqbalОценок пока нет
- Annona 001Документ8 страницAnnona 001iqbalОценок пока нет
- Cheruiyot - The Relationship Between Corporate Social Responsibility and Financial Performance of Companies Listed at The Nairobi Stock Exchange PDFДокумент63 страницыCheruiyot - The Relationship Between Corporate Social Responsibility and Financial Performance of Companies Listed at The Nairobi Stock Exchange PDFjohn MandagoОценок пока нет
- Lex Uri ServДокумент362 страницыLex Uri ServtatjanarubinОценок пока нет
- Academic WritingДокумент5 страницAcademic WritingShayne Herrera IIОценок пока нет
- Hazard Identification of ConstructionДокумент29 страницHazard Identification of ConstructionPintu Jaiswal100% (1)
- Teacher Professional Learning and DevelopmentДокумент32 страницыTeacher Professional Learning and DevelopmentEsteban67% (3)
- Hurlock PDFДокумент717 страницHurlock PDFatrasinadinaОценок пока нет
- Pup VmgoДокумент2 страницыPup VmgoAbbas MaghazehiОценок пока нет
- ZMNT Term Final!Документ22 страницыZMNT Term Final!Siddharth KalsiОценок пока нет
- Interpretation of DataДокумент11 страницInterpretation of Datamelody.magahisОценок пока нет
- Joel Aim IndiaДокумент43 страницыJoel Aim IndiaJoel BijoyОценок пока нет
- Bedan Research Journal2021Документ320 страницBedan Research Journal2021XUEWEI GANОценок пока нет
- A Study On Determinants of Unemployment in PakistanДокумент13 страницA Study On Determinants of Unemployment in PakistanBilal JavedОценок пока нет
- Alex Lyon Abbreviated Curriculum VitaДокумент4 страницыAlex Lyon Abbreviated Curriculum VitadingdionОценок пока нет
- Scientific Publishing in Biomedicine How To Choose A JournalДокумент9 страницScientific Publishing in Biomedicine How To Choose A JournalJuan Carlos Marcos EnriquezОценок пока нет
- 26884.nalr (Ge101)Документ5 страниц26884.nalr (Ge101)aarshiya3031Оценок пока нет
- Multicultural Experiential Learning in Music Therapy SupervisionДокумент17 страницMulticultural Experiential Learning in Music Therapy SupervisionDaniele PendezaОценок пока нет
- Brickell and Garrett, 2015 Storytelling Domestic Violence, ACMEДокумент26 страницBrickell and Garrett, 2015 Storytelling Domestic Violence, ACMEBradley GarrettОценок пока нет
- Baby Led Weaning Vs Parent LedДокумент12 страницBaby Led Weaning Vs Parent LedAdil SultaniОценок пока нет
- Oxford Research Encyclopedia of Communication: EnvironmentДокумент20 страницOxford Research Encyclopedia of Communication: EnvironmentMosor VladОценок пока нет
- Human Process Interventions: Selected CasesДокумент74 страницыHuman Process Interventions: Selected CasesAndika Abdi PamaОценок пока нет
- Dissertation Topics On Public International LawДокумент8 страницDissertation Topics On Public International LawPaperWritingServiceSuperiorpapersOmaha100% (1)
- Photos Courtesy: Footprints E.A.R.T.HДокумент4 страницыPhotos Courtesy: Footprints E.A.R.T.HTARUNОценок пока нет
- Ijebr 10 2019 0615Документ19 страницIjebr 10 2019 0615Bara PahlawanОценок пока нет
- Conclusion Chapter Dissertation ExampleДокумент5 страницConclusion Chapter Dissertation ExampleWriteMyPaperCheapBillings100% (1)
- Entry Level Activities Apprentice-1: Teacher NotesДокумент2 страницыEntry Level Activities Apprentice-1: Teacher NotesY. VaidyaОценок пока нет
- Conceptual Design of Chemical Processes - J. DouglasДокумент619 страницConceptual Design of Chemical Processes - J. DouglasJose Suarez67% (3)
- Approaches in Teaching Social StudiesДокумент6 страницApproaches in Teaching Social StudiesJesusa Mendoza100% (1)
- Board Attributes and Processes, Board Effectiveness, and Organizational Innovation: Evidence From Nonprofit OrganizationsДокумент14 страницBoard Attributes and Processes, Board Effectiveness, and Organizational Innovation: Evidence From Nonprofit OrganizationsSari NОценок пока нет
- Concept Note 9Документ12 страницConcept Note 9Nirup ChaudhuryОценок пока нет