Вам также может понравиться
- Classroom Evaluation ChecklistДокумент3 страницыClassroom Evaluation ChecklistAngelaLomagdong94% (18)
- Example Reflection One NRS 411Документ9 страницExample Reflection One NRS 411collin carlosОценок пока нет
- Nur 4144 Quality Improvement PaperДокумент9 страницNur 4144 Quality Improvement Paperapi-370740810Оценок пока нет
- Nursing Philosophy Apa PaperДокумент5 страницNursing Philosophy Apa Paperapi-26840665675% (4)
- Final EvaluationДокумент10 страницFinal Evaluationapi-338285420Оценок пока нет
- 3020 Reflection 1Документ5 страниц3020 Reflection 1api-372418362Оценок пока нет
- Semester 4 Nurs 252 Schorlarly Written PaperДокумент6 страницSemester 4 Nurs 252 Schorlarly Written Paperapi-283956153Оценок пока нет
- Nursing Leadership Philosophy 2Документ8 страницNursing Leadership Philosophy 2api-499926602Оценок пока нет
- Intro Page - Philosophy of NursingДокумент2 страницыIntro Page - Philosophy of Nursingapi-467110214Оценок пока нет
- Nursing PhilosophyДокумент7 страницNursing Philosophyapi-448502475Оценок пока нет
- Acute Care Final Reflective Journal 2018Документ3 страницыAcute Care Final Reflective Journal 2018api-423090662Оценок пока нет
- Running Head: Senior Capstone Reflection 1Документ7 страницRunning Head: Senior Capstone Reflection 1Nathalee WalkerОценок пока нет
- The Ethic of Care: A Moral Compass for Canadian Nursing Practice - Revised EditionОт EverandThe Ethic of Care: A Moral Compass for Canadian Nursing Practice - Revised EditionОценок пока нет
- Advanced Writing Part 1: Formal Essay: Language For IntroductionsДокумент2 страницыAdvanced Writing Part 1: Formal Essay: Language For IntroductionsSara Albaladejo AlbaladejoОценок пока нет
- Personal Philosophy of Nursing - AdvancedДокумент8 страницPersonal Philosophy of Nursing - Advancedapi-328451896Оценок пока нет
- Nur401 Philosophy PaperДокумент7 страницNur401 Philosophy Paperapi-529373199Оценок пока нет
- Professional Meeting Reflective Journal-2Документ3 страницыProfessional Meeting Reflective Journal-2api-399086837Оценок пока нет
- Personal Philosophy of NursingДокумент5 страницPersonal Philosophy of Nursingapi-339774380Оценок пока нет
- Personal Philosophy PaperДокумент6 страницPersonal Philosophy Paperapi-404104900Оценок пока нет
- RN To BSN e PortfolioДокумент7 страницRN To BSN e PortfolioCherie BoyerОценок пока нет
- Midterm Evaluation - ClinicalДокумент7 страницMidterm Evaluation - Clinicalapi-240864098Оценок пока нет
- Acute Care Final Reflective Journal 2018 - Jamie BorelДокумент4 страницыAcute Care Final Reflective Journal 2018 - Jamie Borelapi-431213859Оценок пока нет
- Professional Meeting PaperДокумент6 страницProfessional Meeting Paperapi-403187872Оценок пока нет
- My Nursing Philosophy - Mai Nomura FinalДокумент9 страницMy Nursing Philosophy - Mai Nomura Finalmai_nomura_2Оценок пока нет
- Philosophy of NursingДокумент8 страницPhilosophy of Nursingapi-300623329Оценок пока нет
- Preceptor Evaluation of Student 1Документ2 страницыPreceptor Evaluation of Student 1api-335260566Оценок пока нет
- Clinical ReflectionДокумент6 страницClinical Reflectionapi-381845148Оценок пока нет
- NURS 627 Reflection 2Документ5 страницNURS 627 Reflection 2hlg34Оценок пока нет
- Reflection 2Документ5 страницReflection 2api-372418362Оценок пока нет
- Nur4122 - Nursing Research - Integrative Review PaperДокумент20 страницNur4122 - Nursing Research - Integrative Review Paperapi-380337414Оценок пока нет
- Professional Nursing PhilosophyДокумент7 страницProfessional Nursing Philosophyapi-458040024100% (1)
- Swanson - Tee, GammadДокумент9 страницSwanson - Tee, GammadCheiramina Serolc EetОценок пока нет
- Nursing JournalДокумент6 страницNursing Journalapi-401156566Оценок пока нет
- Nursing ImageДокумент10 страницNursing Imageapi-392400343Оценок пока нет
- 696 Clinical Learning Agreement - Plan EvaluationДокумент16 страниц696 Clinical Learning Agreement - Plan Evaluationapi-456551916Оценок пока нет
- Community Assessment PaperДокумент18 страницCommunity Assessment PaperAlyssa CardinalОценок пока нет
- LEADERSHIPДокумент6 страницLEADERSHIPisonОценок пока нет
- Pre-Grad Leadership Experience Reflection Part BДокумент5 страницPre-Grad Leadership Experience Reflection Part Bapi-285304739Оценок пока нет
- Older Adult Health Promotion ProjectДокумент6 страницOlder Adult Health Promotion Projectapi-404271262Оценок пока нет
- Reflective Journal Med Surg Clinical April 14thДокумент3 страницыReflective Journal Med Surg Clinical April 14thapi-238869728Оценок пока нет
- Personal Philosophy of Nursing PaperДокумент10 страницPersonal Philosophy of Nursing Paperapi-433883631Оценок пока нет
- Nursing Philosophy Apa PaperДокумент7 страницNursing Philosophy Apa Paperapi-449016836Оценок пока нет
- Nursing Philosophy FinalДокумент7 страницNursing Philosophy Finalapi-429837528100% (1)
- Nur 340 Research PaperДокумент8 страницNur 340 Research Paperapi-429837528Оценок пока нет
- Self-Reflection - EportfolioДокумент2 страницыSelf-Reflection - Eportfolioapi-254345179Оценок пока нет
- Ethics Essay Professional MisconductДокумент7 страницEthics Essay Professional Misconductapi-283071924Оценок пока нет
- Running Head: What Nursing Means To Me 1Документ6 страницRunning Head: What Nursing Means To Me 1Caitlyn CannoneОценок пока нет
- Name of StudentДокумент20 страницName of StudentHassan KhanОценок пока нет
- FesarahДокумент8 страницFesarahapi-271855323Оценок пока нет
- Personal Philosophy of Nursing 2015Документ8 страницPersonal Philosophy of Nursing 2015api-283120230100% (1)
- Jean WatsonДокумент2 страницыJean WatsonShanilyn Biong0% (1)
- Final Reflection DkropaczekДокумент3 страницыFinal Reflection Dkropaczekapi-294937204Оценок пока нет
- PGC Reflection FinalДокумент11 страницPGC Reflection Finalapi-581236671Оценок пока нет
- Running Head: CLINICAL REFLECTION 1Документ6 страницRunning Head: CLINICAL REFLECTION 1api-382642757Оценок пока нет
- A ADN or BSN What Is The Difference (A)Документ5 страницA ADN or BSN What Is The Difference (A)adrianazeleОценок пока нет
- Quality and Safety Education For Nurses CompetenciesДокумент5 страницQuality and Safety Education For Nurses CompetenciesSammy ChegeОценок пока нет
- Nursing DelegationДокумент2 страницыNursing DelegationAndre FortunaОценок пока нет
- Watson Theory PaperДокумент9 страницWatson Theory Paperapi-285171922Оценок пока нет
- Critical Reflection1Документ6 страницCritical Reflection1api-313097878Оценок пока нет
- Nursing Reflection - 1st Year PostingДокумент5 страницNursing Reflection - 1st Year PostingNurul NatrahОценок пока нет
- HealthДокумент6 страницHealthapi-422930884Оценок пока нет
- Final AnalysisДокумент2 страницыFinal Analysisapi-337559523Оценок пока нет
- Integrative ReviewДокумент16 страницIntegrative Reviewapi-337559523Оценок пока нет
- Service Learning Project Individual Reflection PaperДокумент3 страницыService Learning Project Individual Reflection Paperapi-33755952350% (2)
- Concept Map 11 4 15Документ4 страницыConcept Map 11 4 15api-337559523Оценок пока нет
- Advocacy Methods FinalДокумент3 страницыAdvocacy Methods Finalapi-337559523Оценок пока нет
- Eportfolio ResumeДокумент1 страницаEportfolio Resumeapi-337559523Оценок пока нет
- Eportfolio ResumeДокумент1 страницаEportfolio Resumeapi-337559523Оценок пока нет
- Comparative Education AustraliaДокумент2 страницыComparative Education AustraliaJoseph Eric Nardo100% (1)
- How School Funding WorksДокумент20 страницHow School Funding WorksCarolyn UptonОценок пока нет
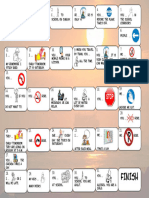
- Modal verbs board gameДокумент1 страницаModal verbs board gameEmmaBordetОценок пока нет
- English Teaching Methods ExamДокумент1 страницаEnglish Teaching Methods ExamNicoleta Maria MoisinОценок пока нет
- School Report CardsДокумент80 страницSchool Report CardswindsorstarОценок пока нет
- Creative TeachingДокумент254 страницыCreative TeachingYusuf Rizal100% (1)
- Hmec5313 - V2 Counseling and Guiding Children in Early Childhood EducationДокумент13 страницHmec5313 - V2 Counseling and Guiding Children in Early Childhood EducationTutor EvonОценок пока нет
- Assignment: English: Name Zuhaib AhmedДокумент5 страницAssignment: English: Name Zuhaib AhmedZuhaib AhmedОценок пока нет
- Child and Adolescent DevelopmentДокумент5 страницChild and Adolescent Developmentandrew gauranaОценок пока нет
- Manage Software ProjectsДокумент4 страницыManage Software ProjectsRas Abel BekeleОценок пока нет
- Preparing For NDA Exam With SchoolДокумент2 страницыPreparing For NDA Exam With SchoolAafia GauseОценок пока нет
- The Obstructive ObjectДокумент13 страницThe Obstructive ObjectCarla Santos100% (1)
- Math 120 Past Exam QuestionsДокумент199 страницMath 120 Past Exam Questions19cerena03Оценок пока нет
- JD-Virtual Customer Service-Amazon IndiaДокумент3 страницыJD-Virtual Customer Service-Amazon IndiaAnkitSharmaОценок пока нет
- BS en 1011-1-2005Документ15 страницBS en 1011-1-2005reezmanОценок пока нет
- The 2017 Terahertz Science and Technology Roadmap: Journal of Physics D: Applied PhysicsДокумент50 страницThe 2017 Terahertz Science and Technology Roadmap: Journal of Physics D: Applied PhysicsNUR AZIZATUL ULYAОценок пока нет
- DLL W11 MilДокумент4 страницыDLL W11 MilRICKELY BANTAОценок пока нет
- WhizCard CLF C01 06 09 2022Документ111 страницWhizCard CLF C01 06 09 2022sridhiyaОценок пока нет
- R22 - IT - Python Programming Lab ManualДокумент96 страницR22 - IT - Python Programming Lab ManualJasmitha BompellyОценок пока нет
- 50 Legitimage Ways 2 Make Money From HomeДокумент15 страниц50 Legitimage Ways 2 Make Money From HomeW Kay100% (1)
- Audio/Radio Production I Syllabus: Dallas College North Lake CampusДокумент13 страницAudio/Radio Production I Syllabus: Dallas College North Lake CampusUriel MenesesОценок пока нет
- Residential Comprehensive 2015 Leaflet PDFДокумент7 страницResidential Comprehensive 2015 Leaflet PDFmsatpathy2003Оценок пока нет
- Eapp Summative Test 2023 2024Документ5 страницEapp Summative Test 2023 2024Ed Vincent M. YbañezОценок пока нет
- Indian states with highest and lowest dropout ratesДокумент23 страницыIndian states with highest and lowest dropout ratesAJIT SINGHОценок пока нет
- Mathematics For Language - Language For MathematicsДокумент16 страницMathematics For Language - Language For MathematicsLenka TejkalovaОценок пока нет
- HG Las Q1 W3 Hawking RamosДокумент4 страницыHG Las Q1 W3 Hawking RamosSecond SubscriberОценок пока нет
- Mechanical CADD CourseДокумент8 страницMechanical CADD CourseCadd CentreОценок пока нет
- Individual Performance Commtment &review Form (Ipcr) : Approved: FacultyДокумент2 страницыIndividual Performance Commtment &review Form (Ipcr) : Approved: FacultyFrancis AlmiaОценок пока нет