Вам также может понравиться
- 4-How To EvaluateДокумент18 страниц4-How To EvaluateDuilio GuerreroОценок пока нет
- 4-How To PDFДокумент18 страниц4-How To PDFninin latwolatwoОценок пока нет
- Program Evaluation Methods PDFДокумент152 страницыProgram Evaluation Methods PDFRiaTorano100% (1)
- Prescriptive Model Report DummyДокумент5 страницPrescriptive Model Report DummyMaestro GallaОценок пока нет
- DP Me Standards For Evaluation in Government V 2140306Документ16 страницDP Me Standards For Evaluation in Government V 2140306Kaua PitondoОценок пока нет
- Evaluation Methods - An Overview v1Документ6 страницEvaluation Methods - An Overview v1Rashad IshaqОценок пока нет
- M&E KatendeДокумент39 страницM&E KatendeBopzilla ReddyОценок пока нет
- Overview of The Framework For Program Evaluation: CDC E W GДокумент3 страницыOverview of The Framework For Program Evaluation: CDC E W GwaitОценок пока нет
- 505 Evaluation Chapter QuestionsДокумент9 страниц505 Evaluation Chapter QuestionsBrian MitchellОценок пока нет
- Topic 7. Strategy Monitoring and Evaluation Tools and Methods-2Документ13 страницTopic 7. Strategy Monitoring and Evaluation Tools and Methods-2carolineОценок пока нет
- Program Evaluation DefinedДокумент7 страницProgram Evaluation DefinedthisisghostactualОценок пока нет
- Categorization of Evaluation Techniques-1Документ16 страницCategorization of Evaluation Techniques-1Krushna KhedkarОценок пока нет
- Monitoring & Evaluation of Health Programs: Yodit Zewdie (MPH, Ass. Professor)Документ30 страницMonitoring & Evaluation of Health Programs: Yodit Zewdie (MPH, Ass. Professor)AmsaluОценок пока нет
- Dev & Planning Assignment: Umair AlamДокумент5 страницDev & Planning Assignment: Umair AlamUmair RehmanОценок пока нет
- 5068 Preskill Chapter 5Документ80 страниц5068 Preskill Chapter 5pj501Оценок пока нет
- Module 8 - INTRODUCTION TO MONITORING AND EVALUATIONДокумент33 страницыModule 8 - INTRODUCTION TO MONITORING AND EVALUATIONAnthony100% (1)
- CDC Evaluation Framework SummaryДокумент23 страницыCDC Evaluation Framework Summaryzaky ariandyОценок пока нет
- A Guide To Evaluating Road Safety Education Programs For Young AdultsДокумент50 страницA Guide To Evaluating Road Safety Education Programs For Young AdultsShuaib IsmailОценок пока нет
- 7 - Evaluating A Health Education PlanДокумент11 страниц7 - Evaluating A Health Education Plancristine albanoОценок пока нет
- Week 1 UNFPA PurposesofEvalДокумент6 страницWeek 1 UNFPA PurposesofEvallaeli sukmahayaniОценок пока нет
- Focusing Your Evaluation...................................... 4Документ49 страницFocusing Your Evaluation...................................... 4mohamad-abdul-sater-1406Оценок пока нет
- Designing An Effective Evaluation Strategy:: Sharon Schnelle, PH.DДокумент32 страницыDesigning An Effective Evaluation Strategy:: Sharon Schnelle, PH.DClyde SalaritanОценок пока нет
- Project Monitoring and Evaluation PlanДокумент21 страницаProject Monitoring and Evaluation Planeliza ChaleОценок пока нет
- 2020 Guide On Monitoring and Evaluation For BeginnersДокумент30 страниц2020 Guide On Monitoring and Evaluation For Beginnersmarija100% (3)
- Question Assignment 1Документ8 страницQuestion Assignment 1Moiz AntariaОценок пока нет
- M E GuidelinesДокумент25 страницM E GuidelinesJoel RotichОценок пока нет
- 490 14Документ15 страниц490 14Riski Fitri DamayОценок пока нет
- Program Development-PolicyДокумент6 страницProgram Development-Policyapi-528796845Оценок пока нет
- NCM 113 Midterm Lec Mod 6Документ10 страницNCM 113 Midterm Lec Mod 6Angel Khrisna BacasmotОценок пока нет
- 4-9 Core Concepts in Developing M&E - 2013Документ15 страниц4-9 Core Concepts in Developing M&E - 2013Tunal TayualistiОценок пока нет
- (Pertemuan 6) Evaluasi Di KomunitasДокумент26 страниц(Pertemuan 6) Evaluasi Di Komunitaswindi pujiaОценок пока нет
- Evaluation Approaches, Framework, and DesignsДокумент15 страницEvaluation Approaches, Framework, and DesignsDanson Githinji EОценок пока нет
- Bench MarkingДокумент25 страницBench Markingavnishchauhan8_46499Оценок пока нет
- Monitoring & Evaluation EssentialsДокумент27 страницMonitoring & Evaluation EssentialsWaltas Kariuki0% (2)
- Mentoring 418Документ27 страницMentoring 418Romaine Russell100% (1)
- GROUP 4 - Project DesignДокумент19 страницGROUP 4 - Project Designodeke aronОценок пока нет
- Defination of Training and EvaluationДокумент13 страницDefination of Training and EvaluationUmika SawhneyОценок пока нет
- Managing Continuous Improvement SystemДокумент18 страницManaging Continuous Improvement SystemDark KnightОценок пока нет
- Impact Evaluations in UN Agency Evaluation Systems - Guidance On Selection, Planning and ManagementДокумент43 страницыImpact Evaluations in UN Agency Evaluation Systems - Guidance On Selection, Planning and ManagementSergio GaudencioОценок пока нет
- CPD M&E Framework GuideДокумент15 страницCPD M&E Framework GuideVitalise AdongoОценок пока нет
- Assessing Project Processes and ImpactsДокумент17 страницAssessing Project Processes and ImpactsJunior ValОценок пока нет
- M & E TestДокумент10 страницM & E TesttkurasaОценок пока нет
- Evaluating Communication For DevelopmentДокумент21 страницаEvaluating Communication For DevelopmentAikoGonzalesCastroОценок пока нет
- Draft Monitoring and Evaluation ManualДокумент38 страницDraft Monitoring and Evaluation ManualJoshua Abao100% (1)
- Evaluating Programmes with StandardsДокумент7 страницEvaluating Programmes with Standardscamry_ngОценок пока нет
- RBM Toolkit - Doc WordДокумент43 страницыRBM Toolkit - Doc WordMuhammad Azam TahirОценок пока нет
- Economic Appraisal - v5.6 A4 Final WebДокумент13 страницEconomic Appraisal - v5.6 A4 Final WebHEENA GARGОценок пока нет
- Models and Methods For Evaluation: Ron OwstonДокумент14 страницModels and Methods For Evaluation: Ron OwstonAMAAL ALORINIОценок пока нет
- Standard Comprehensive Training PlanДокумент26 страницStandard Comprehensive Training PlanAlicia PearlОценок пока нет
- Monitoring & EvaluationДокумент21 страницаMonitoring & EvaluationAbas AhmedОценок пока нет
- Expectations and Deliverables HSE Excellence AwardДокумент4 страницыExpectations and Deliverables HSE Excellence AwardOki EriandiОценок пока нет
- Advocacy Toolkit CompanionДокумент50 страницAdvocacy Toolkit CompanionGail HoadОценок пока нет
- Unit Introduction To Monitoring and EvaluationДокумент3 страницыUnit Introduction To Monitoring and EvaluationKouame AdjepoleОценок пока нет
- Topic 3 - Models of Monitoring and Evaluation - Types of Evaluation Process, Outcome and ImpactДокумент54 страницыTopic 3 - Models of Monitoring and Evaluation - Types of Evaluation Process, Outcome and Impactmohammadnazar saqi100% (1)
- What Is Program EvaluationДокумент42 страницыWhat Is Program EvaluationDoru ConstantinОценок пока нет
- Question Assignment 2Документ9 страницQuestion Assignment 2Moiz AntariaОценок пока нет
- Siemens Nixdorf CaseДокумент7 страницSiemens Nixdorf CaseMarwa Mourad IbОценок пока нет
- 6 Steps 4 Standards Program EvaluationДокумент26 страниц6 Steps 4 Standards Program EvaluationAdeq NorzuaniОценок пока нет
- Audit Engagement Strategy (Driving Audit Value, Vol. III): The Best Practice Strategy Guide for Maximising the Added Value of the Internal Audit EngagementsОт EverandAudit Engagement Strategy (Driving Audit Value, Vol. III): The Best Practice Strategy Guide for Maximising the Added Value of the Internal Audit EngagementsОценок пока нет
- Case 3 CA Nasofaring Dr. Oscar, SPTHTДокумент16 страницCase 3 CA Nasofaring Dr. Oscar, SPTHTAndy XiaoОценок пока нет
- Nasi Lemak Restaurants in Bangsar VillageДокумент1 страницаNasi Lemak Restaurants in Bangsar VillageAndy XiaoОценок пока нет
- Water Imaging FetusДокумент9 страницWater Imaging FetusAndy XiaoОценок пока нет
- Aha SVTДокумент69 страницAha SVTdeardiarymysteryОценок пока нет
- Who FCH Cah 06.1Документ123 страницыWho FCH Cah 06.1Ðr SalmaОценок пока нет
- CJC 31 04 185Документ12 страницCJC 31 04 185Azan Al RasyidОценок пока нет
- NASOPHARYNGEAL CARCINOMA CASE PRESENTATIONДокумент37 страницNASOPHARYNGEAL CARCINOMA CASE PRESENTATIONAndy XiaoОценок пока нет
- Referat Farmakologi Obat AnestesiДокумент11 страницReferat Farmakologi Obat AnestesiAndy XiaoОценок пока нет
- Who FCH Cah 06.1Документ123 страницыWho FCH Cah 06.1Ðr SalmaОценок пока нет
- Poster 10 NLS 01 01 ENG V20100927 PDFДокумент1 страницаPoster 10 NLS 01 01 ENG V20100927 PDFAndy XiaoОценок пока нет
- Anatomy of The Ear FixДокумент40 страницAnatomy of The Ear FixAndy XiaoОценок пока нет
- Aorta: Normal Radiological Reference ValuesДокумент3 страницыAorta: Normal Radiological Reference ValuesJha K SujitОценок пока нет
- Positioningandradiographicanatomyoftheskull 131218154334 Phpapp01Документ121 страницаPositioningandradiographicanatomyoftheskull 131218154334 Phpapp01Andy XiaoОценок пока нет
- Case OMA DR - Oscar, SPTHTДокумент29 страницCase OMA DR - Oscar, SPTHTAndy XiaoОценок пока нет
- Angina Ludovici EmergenciesДокумент5 страницAngina Ludovici EmergenciesAndy XiaoОценок пока нет
- Laboratory: Anne Z - Saunders, Andrea Vallen Stein, and Nancy Lite ShusterДокумент3 страницыLaboratory: Anne Z - Saunders, Andrea Vallen Stein, and Nancy Lite ShusterAndy XiaoОценок пока нет
- Poster 10 PALS 01 01 ENG V20100927 PDFДокумент1 страницаPoster 10 PALS 01 01 ENG V20100927 PDFAndy XiaoОценок пока нет
- 10.1 Life-Threatening Electrolyte AbnormalitiesДокумент6 страниц10.1 Life-Threatening Electrolyte AbnormalitiesWidya WidyariniОценок пока нет
- Poster 10 NLS 01 01 ENG V20100927 PDFДокумент1 страницаPoster 10 NLS 01 01 ENG V20100927 PDFAndy XiaoОценок пока нет
- Poster 10 ALS-TACH 01 01 ENG V20100927Документ1 страницаPoster 10 ALS-TACH 01 01 ENG V20100927Andy XiaoОценок пока нет
- Basic Life Support & Automated External Defibrillation: Check ResponseДокумент1 страницаBasic Life Support & Automated External Defibrillation: Check ResponseAndy XiaoОценок пока нет
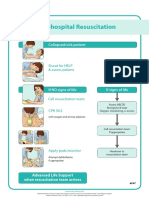
- Poster 10 IHBLS 01 01 ENG V20100927Документ1 страницаPoster 10 IHBLS 01 01 ENG V20100927Andy XiaoОценок пока нет
- Iv 136Документ4 страницыIv 136Andy XiaoОценок пока нет
- Poster 10 ALS-BRAD 01 01 ENG V20100927Документ1 страницаPoster 10 ALS-BRAD 01 01 ENG V20100927Andy XiaoОценок пока нет
- Iv 133Документ4 страницыIv 133Andy XiaoОценок пока нет
- Iv 111Документ11 страницIv 111Andy XiaoОценок пока нет
- Universal Algorithm: Advanced Life SupportДокумент1 страницаUniversal Algorithm: Advanced Life SupportAndy XiaoОценок пока нет
- Iv 89Документ23 страницыIv 89Andy XiaoОценок пока нет
- Cardioversion, and Pacing Part 5: Electrical Therapies: Automated External Defibrillators, DefibrillationДокумент13 страницCardioversion, and Pacing Part 5: Electrical Therapies: Automated External Defibrillators, DefibrillationAndy XiaoОценок пока нет
- Iv 84 PDFДокумент6 страницIv 84 PDFAndy XiaoОценок пока нет
- Fire Retardant Research PaperДокумент2 страницыFire Retardant Research Paperapi-318759920Оценок пока нет
- Personal Trainer TextДокумент97 страницPersonal Trainer Textwuddafren100% (1)
- 296402-Official ESTA Application Website U.S. Customs and Border Protection PDFДокумент5 страниц296402-Official ESTA Application Website U.S. Customs and Border Protection PDFLouise Ann TunstallОценок пока нет
- International Journal of Radiology and Imaging Technology Ijrit 7 082Документ3 страницыInternational Journal of Radiology and Imaging Technology Ijrit 7 082Zafitri AsrulОценок пока нет
- Burnett: The First Non-Conformist HomeopathДокумент4 страницыBurnett: The First Non-Conformist Homeopathsimiliadoc100% (1)
- MRNA Vaccines - Day - 04.14.20 PDFДокумент259 страницMRNA Vaccines - Day - 04.14.20 PDFTammy G100% (1)
- HO#1.1 Caring For The BodyДокумент7 страницHO#1.1 Caring For The BodyGemma CanlapanОценок пока нет
- ImplantsДокумент11 страницImplantsraheelОценок пока нет
- MKWD Lwua Adb Package 2 AnnexesДокумент199 страницMKWD Lwua Adb Package 2 AnnexesRoland AnaumОценок пока нет
- Analytical Exposition Text Corona Should Be Against Surround UsДокумент2 страницыAnalytical Exposition Text Corona Should Be Against Surround UsRifkyОценок пока нет
- PamphletДокумент1 страницаPamphletAldenn MinotaurОценок пока нет
- Grade 7 (TLE) Week 1Документ12 страницGrade 7 (TLE) Week 1RoswlleОценок пока нет
- NO Kodebarang Satuan Pakai Stock Awal Masuk Keluar Stock Akhir Harga KeteranganДокумент4 страницыNO Kodebarang Satuan Pakai Stock Awal Masuk Keluar Stock Akhir Harga Keteranganruang belajar farmasiОценок пока нет
- Manuale Advantage 350Документ50 страницManuale Advantage 350PaulmankeОценок пока нет
- Inflammation - The Silent Killer - Terra Health EssentialsДокумент6 страницInflammation - The Silent Killer - Terra Health EssentialshighlanderoneОценок пока нет
- Catheterization ChecklistДокумент3 страницыCatheterization ChecklistAlthea Aubrey AgbayaniОценок пока нет
- USMLE High YieldДокумент8 страницUSMLE High YieldNajia ChoudhuryОценок пока нет
- Memory Manipulation PDFДокумент381 страницаMemory Manipulation PDFAlapan Bandyopadhyay100% (2)
- Antonella Arrieta LaurentДокумент24 страницыAntonella Arrieta LaurentEmanueleОценок пока нет
- Acetabular and Hip FractureДокумент133 страницыAcetabular and Hip FractureJuanita HenryОценок пока нет
- 2016 3 23 9 12 47tapchi-Dhdn-So12 (97) .2015-Color-WebДокумент128 страниц2016 3 23 9 12 47tapchi-Dhdn-So12 (97) .2015-Color-WebThọ Nguyễn Văn100% (1)
- Exercise Chart: Warm UpДокумент1 страницаExercise Chart: Warm UpJeremy van der MerweОценок пока нет
- ACIDITY REMEDIESДокумент3 страницыACIDITY REMEDIESYasmeen JafferОценок пока нет
- Mdbsis09 CA A III 2017Документ4 страницыMdbsis09 CA A III 2017Guneyden GuneydenОценок пока нет
- Nogales v. Capitol Medical Center DigestДокумент4 страницыNogales v. Capitol Medical Center DigestWilliam AzucenaОценок пока нет
- Serial number verification formДокумент1 страницаSerial number verification formArjelyОценок пока нет
- Aiapget 2020 QPДокумент29 страницAiapget 2020 QPGanesh RadhakrishnanОценок пока нет
- Details of Positive Cases in Kurnool DistrictДокумент60 страницDetails of Positive Cases in Kurnool DistrictSohail MullaОценок пока нет
- Verification of Conformity Safety Consideration For Radio Equipment DirectiveДокумент1 страницаVerification of Conformity Safety Consideration For Radio Equipment DirectiveThắng CòiОценок пока нет
- Functional Test and Weight Verification of BalancesДокумент5 страницFunctional Test and Weight Verification of BalancesMartellRОценок пока нет