Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Sample Immunization CertificateДокумент2 страницыSample Immunization Certificateanusdasari100% (10)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Hyoscine Assay Lecture-3aДокумент9 страницHyoscine Assay Lecture-3asultanОценок пока нет
- NSAIDs - Jack DeRuiter, Principles of Drug Action 2, Fall 2002Документ26 страницNSAIDs - Jack DeRuiter, Principles of Drug Action 2, Fall 2002Sai Kishore K100% (1)
- AnginaДокумент17 страницAnginasultanОценок пока нет
- First AidДокумент73 страницыFirst AidsultanОценок пока нет
- Chem2-Jan 19-Lab 1-Aspirin Quality ControlДокумент3 страницыChem2-Jan 19-Lab 1-Aspirin Quality Controlsultan0% (2)
- Diphtheria by DR SarmaДокумент14 страницDiphtheria by DR SarmasultanОценок пока нет
- Determination of The Ka Ofa Weak AcidДокумент7 страницDetermination of The Ka Ofa Weak AcidFikrie MuhdОценок пока нет
- Chem2-Jan 19-Lab 1-Aspirin Quality ControlДокумент3 страницыChem2-Jan 19-Lab 1-Aspirin Quality Controlsultan0% (2)
- Resume TemplateДокумент1 страницаResume TemplateYaseen MohamedОценок пока нет
- Resume TemplateДокумент1 страницаResume TemplateYaseen MohamedОценок пока нет
- Resume TemplateДокумент1 страницаResume TemplateYaseen MohamedОценок пока нет
- Resume TemplateДокумент1 страницаResume TemplateYaseen MohamedОценок пока нет
- DiphtheriaДокумент49 страницDiphtheriasultanОценок пока нет
- Limit Test of Chloride - Lecture-1Документ2 страницыLimit Test of Chloride - Lecture-1sultan100% (2)
- 04fc75de986c12 Pharmaceutics-I AROMATIC WATERSДокумент14 страниц04fc75de986c12 Pharmaceutics-I AROMATIC WATERSsultanОценок пока нет
- Chapter 27 (Perry & Potter)Документ41 страницаChapter 27 (Perry & Potter)sultanОценок пока нет
- Phar Calculations ReviewДокумент44 страницыPhar Calculations ReviewSarah JaneОценок пока нет
- Solutions PPT112Документ31 страницаSolutions PPT112sultanОценок пока нет
- 3 - Lectures of Capsules PracticalДокумент4 страницы3 - Lectures of Capsules PracticalsultanОценок пока нет
- Practical OintmentДокумент5 страницPractical OintmentmdsajidaaliОценок пока нет
- UNODC Methods For Idenfification and Analysis of Cocaine in Seized MaterialsДокумент48 страницUNODC Methods For Idenfification and Analysis of Cocaine in Seized MaterialsauredrelleОценок пока нет
- Chapter 27 (Perry & Potter)Документ41 страницаChapter 27 (Perry & Potter)sultanОценок пока нет
- Practical OintmentДокумент5 страницPractical OintmentmdsajidaaliОценок пока нет
- Laboratory Manual For: Physical Pharmacy IДокумент2 страницыLaboratory Manual For: Physical Pharmacy IsultanОценок пока нет
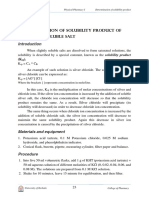
- Lab. 5 Determination of Solubility ProductДокумент4 страницыLab. 5 Determination of Solubility ProductsultanОценок пока нет
- Pharmaceutics Lab 156P, Spring 2016 Calculations and Compounding Syllabus/First Day HandoutДокумент4 страницыPharmaceutics Lab 156P, Spring 2016 Calculations and Compounding Syllabus/First Day HandoutsultanОценок пока нет
- Lab. 6 Buffer SolutionsДокумент4 страницыLab. 6 Buffer Solutionssultan100% (1)
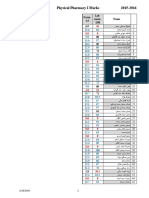
- Physical Pharmacy I Lab Exam MarksДокумент3 страницыPhysical Pharmacy I Lab Exam MarkssultanОценок пока нет
- Immunization ScheduleДокумент10 страницImmunization Schedulerandom.mail.scsm7112Оценок пока нет
- Astrazenica 2nd Dose 8-11-21 Alkie - Copy - Copy - Copy - Copy - Copy (Autorecovered)Документ109 страницAstrazenica 2nd Dose 8-11-21 Alkie - Copy - Copy - Copy - Copy - Copy (Autorecovered)Ganie Mar BiasonОценок пока нет
- Vaccination Schedule For Papua New Guinea 2022-027-010 1-38 UTCДокумент6 страницVaccination Schedule For Papua New Guinea 2022-027-010 1-38 UTCChuck AnsphilОценок пока нет
- Vaccination 860322235671Документ2 страницыVaccination 860322235671Nur Anis MazlinaОценок пока нет
- Certificate PDFДокумент1 страницаCertificate PDFbliss bОценок пока нет
- Vaccination EPI and Non EPIДокумент19 страницVaccination EPI and Non EPIRakhshanda khanОценок пока нет
- D - Vaccination Minor Consent FormДокумент2 страницыD - Vaccination Minor Consent FormNoemi CamberosОценок пока нет
- Certificate RajatДокумент1 страницаCertificate Rajatrajat meshramОценок пока нет
- Nithya CertificateДокумент1 страницаNithya CertificateVasanth RajuОценок пока нет
- Maklumat Vaksinasi: Vaccination DetailsДокумент1 страницаMaklumat Vaksinasi: Vaccination DetailsazlanОценок пока нет
- Injection Site and Needle Size Vaccine Dose RouteДокумент1 страницаInjection Site and Needle Size Vaccine Dose RouteDoc JT BylnОценок пока нет
- CertificateДокумент1 страницаCertificateKavinОценок пока нет
- The Covi d-19 Vacci Ne, The New Li Fe Saver: A Brief IntroductionДокумент3 страницыThe Covi d-19 Vacci Ne, The New Li Fe Saver: A Brief IntroductionyaraОценок пока нет
- SdsadsdadsДокумент143 страницыSdsadsdadsKayeОценок пока нет
- PosterДокумент1 страницаPosterIzzah IzatiОценок пока нет
- EPI Schedule of PakistanДокумент1 страницаEPI Schedule of Pakistanksbabar100% (1)
- Take 5 - Covid VaccineДокумент5 страницTake 5 - Covid VaccinetasialalalaОценок пока нет
- Mission Indradhanush To Put Vaccination Efforts On High SpeedДокумент3 страницыMission Indradhanush To Put Vaccination Efforts On High Speedchitransh90Оценок пока нет
- Certificate For COVID-19 Vaccination: Beneficiary DetailsДокумент1 страницаCertificate For COVID-19 Vaccination: Beneficiary DetailsamzadsmartОценок пока нет
- Revised Quotation Invitation For UPS For The Year 2017-18Документ67 страницRevised Quotation Invitation For UPS For The Year 2017-18rkg06011988Оценок пока нет
- CertificateДокумент1 страницаCertificateSubhajit MandalОценок пока нет
- EN Information Bulletin VVM AssignmentsДокумент4 страницыEN Information Bulletin VVM AssignmentsgnkarthikeyaОценок пока нет
- Akshat Singh 0353Документ4 страницыAkshat Singh 0353AKSHAT SINGHОценок пока нет
- MOH - UNICEF - Vaccine: PharmaceuticalsДокумент3 страницыMOH - UNICEF - Vaccine: Pharmaceuticalszinabu tesfayeОценок пока нет
- CertificateДокумент1 страницаCertificateShubham TiwariОценок пока нет
- Immunization ScheduleДокумент1 страницаImmunization ScheduleOksana PersaudОценок пока нет
- Certificate For COVID-19 Vaccination: Beneficiary DetailsДокумент1 страницаCertificate For COVID-19 Vaccination: Beneficiary DetailsHimanshu TanwarОценок пока нет
- Maklumat Vaksinasi: Vaccination DetailsДокумент2 страницыMaklumat Vaksinasi: Vaccination DetailsEkyienОценок пока нет
- The Different Types of COVID-19 VaccinesДокумент4 страницыThe Different Types of COVID-19 VaccinesSusanty NazmiОценок пока нет