Вам также может понравиться
- Tooth-Implant ConnectionДокумент63 страницыTooth-Implant Connectionmanasvi100% (1)
- Nursing Management of Oral HygieneДокумент40 страницNursing Management of Oral HygieneMheanne RomanoОценок пока нет
- Tongue in Complete DentureДокумент8 страницTongue in Complete DentureAman SachdevaОценок пока нет
- Prosthodontics QPДокумент8 страницProsthodontics QPsamhitaОценок пока нет
- Components FPDДокумент91 страницаComponents FPDKashish08Оценок пока нет
- Lab Procedures in Complete Denture Prosthodontics / Orthodontic Courses by Indian Dental AcademyДокумент90 страницLab Procedures in Complete Denture Prosthodontics / Orthodontic Courses by Indian Dental Academyindian dental academy100% (1)
- Working Length DeterminationДокумент97 страницWorking Length Determinationrolly_jatinОценок пока нет
- Congenitally Missing Maxillary Lateral IncisorsДокумент56 страницCongenitally Missing Maxillary Lateral Incisorsdrsankhya100% (1)
- Intracoronal Attachments For Removable Partial DenturesДокумент18 страницIntracoronal Attachments For Removable Partial Denturesapi-3710948100% (6)
- Hand Out 2021 Restoration of Endodontically Treated TeethДокумент40 страницHand Out 2021 Restoration of Endodontically Treated TeethpriyaОценок пока нет
- MRD Past Years - Faezah3Документ11 страницMRD Past Years - Faezah3neelmakhan5748100% (2)
- Silverman 1971Документ19 страницSilverman 1971Krupali JainОценок пока нет
- RPD Clasp DesignДокумент10 страницRPD Clasp DesignAmar BhochhibhoyaОценок пока нет
- Alginate Impression MaterialДокумент92 страницыAlginate Impression MaterialrusschallengerОценок пока нет
- Cavitypreparation 130320103634 Phpapp01Документ60 страницCavitypreparation 130320103634 Phpapp01Sumit BediОценок пока нет
- Direct RetainersДокумент10 страницDirect RetainersSakinah SyahirahОценок пока нет
- Teeth Selection and ArrangementДокумент118 страницTeeth Selection and Arrangementaakankshakanwar100% (2)
- Supra-Gingival Minimally Invasive Dentistry: A Healthier Approach to Esthetic RestorationsОт EverandSupra-Gingival Minimally Invasive Dentistry: A Healthier Approach to Esthetic RestorationsРейтинг: 5 из 5 звезд5/5 (1)
- Basic Principles of Obturator Design IIДокумент7 страницBasic Principles of Obturator Design IIGilberto Arturo Huapaya MarcosОценок пока нет
- Biological Considerations in Mandibular ImpressionДокумент105 страницBiological Considerations in Mandibular Impressionshraddha100% (1)
- Non Surgical Endodontic Retreatment: Presented byДокумент58 страницNon Surgical Endodontic Retreatment: Presented bySayak GuptaОценок пока нет
- Occlusion in Implant Prosthodontics: Radhika B Parekh, Omkar Shetty, Rubina TabassumДокумент4 страницыOcclusion in Implant Prosthodontics: Radhika B Parekh, Omkar Shetty, Rubina TabassumTung Thanh NguyenОценок пока нет
- Complete Denture JourneyДокумент30 страницComplete Denture JourneysapnaОценок пока нет
- Balanced Occlu HandoutДокумент9 страницBalanced Occlu HandoutMostafa FayadОценок пока нет
- Selecion of Major ConnectorsДокумент2 страницыSelecion of Major ConnectorsTanmay SrivastavaОценок пока нет
- Fixed Orthodontic Appliances: A Practical GuideОт EverandFixed Orthodontic Appliances: A Practical GuideРейтинг: 1 из 5 звезд1/5 (1)
- Orthodontically Driven Corticotomy: Tissue Engineering to Enhance Orthodontic and Multidisciplinary TreatmentОт EverandOrthodontically Driven Corticotomy: Tissue Engineering to Enhance Orthodontic and Multidisciplinary TreatmentFederico BrugnamiОценок пока нет
- Lecture 6 Acrylic RPDДокумент23 страницыLecture 6 Acrylic RPDAmmar AldawoodyehОценок пока нет
- Relining and Rebasing of Complete DenturesДокумент28 страницRelining and Rebasing of Complete DenturesPurnama SyahbaniОценок пока нет
- Bds Tutorial Overdentures 1Документ7 страницBds Tutorial Overdentures 1ikeuchi_ogawaОценок пока нет
- Biomechanics and Clinical Implications of Complete Edentulous StateДокумент4 страницыBiomechanics and Clinical Implications of Complete Edentulous StateDorobantuMihaiGabiОценок пока нет
- Dahl's ApplianceДокумент7 страницDahl's AppliancerekabiОценок пока нет
- Jurnal DentistДокумент8 страницJurnal DentistAnugrah AztriОценок пока нет
- Oral Diagnosis and Treatment Planning: Part 7. Treatment Planning For Missing TeethДокумент11 страницOral Diagnosis and Treatment Planning: Part 7. Treatment Planning For Missing TeethalfredoibcОценок пока нет
- Prostho Lec - OverdenturesДокумент14 страницProstho Lec - Overdenturesdrgayen6042Оценок пока нет
- Overdenture 4th Year 15-3-2020Документ52 страницыOverdenture 4th Year 15-3-2020Ahmed AliОценок пока нет
- Overdenture 140503222227 Phpapp01Документ107 страницOverdenture 140503222227 Phpapp01TatsamYadavОценок пока нет
- Removable Partial DentureДокумент16 страницRemovable Partial DentureRonald NarsicoОценок пока нет
- ISSN: 0975-833X: Research ArticleДокумент9 страницISSN: 0975-833X: Research ArticleSuryo HannaОценок пока нет
- 12 Pin Retained RestorationДокумент59 страниц12 Pin Retained RestorationMohsin HabibОценок пока нет
- My 3rd Seminar - DentinДокумент25 страницMy 3rd Seminar - DentinJon YorkОценок пока нет
- Removable Partial DentureДокумент38 страницRemovable Partial DentureNissaОценок пока нет
- Management of Acquired Maxillary Defects Partially Edentlous PDFДокумент129 страницManagement of Acquired Maxillary Defects Partially Edentlous PDFRamy Khalifa AshmawyОценок пока нет
- Occlusal MoldsДокумент7 страницOcclusal MoldsFrederico Diego Medeiros LimaОценок пока нет
- Complete Rehabilitation of A Patient With Occlusal Wear PDFДокумент7 страницComplete Rehabilitation of A Patient With Occlusal Wear PDFsarfarazahmad19Оценок пока нет
- Debate Acrylic Vs Cobalt ChromeДокумент29 страницDebate Acrylic Vs Cobalt ChromeNafij JamayetОценок пока нет
- Single Complete DentureДокумент23 страницыSingle Complete DentureNelly SuriamahОценок пока нет
- Recent Advances in Provisional RestorationsДокумент6 страницRecent Advances in Provisional RestorationsAngelia PratiwiОценок пока нет
- Direct Retainers (Infra Bulge)Документ31 страницаDirect Retainers (Infra Bulge)Bara Abdul0% (1)
- Partial Retainer in FPD DR VikasДокумент99 страницPartial Retainer in FPD DR VikasVikas AggarwalОценок пока нет
- 0 - A Clinical Guide To OcclusionДокумент1 страница0 - A Clinical Guide To Occlusionyhajo100% (1)
- Bicon Seating ChecklistДокумент2 страницыBicon Seating ChecklistRoger VergarayОценок пока нет
- Occlusion / Orthodontic Courses by Indian Dental AcademyДокумент90 страницOcclusion / Orthodontic Courses by Indian Dental Academyindian dental academyОценок пока нет
- Principles of Tooth PreparationДокумент10 страницPrinciples of Tooth Preparationruchika100% (2)
- Practice: Restoration of The Root-Filled Tooth: Pre-Operative AssessmentДокумент10 страницPractice: Restoration of The Root-Filled Tooth: Pre-Operative AssessmenteletiОценок пока нет
- Accurate ALginate ImpressionДокумент2 страницыAccurate ALginate Impressionlah_saneОценок пока нет
- Try in AppointmentДокумент91 страницаTry in Appointmentspu123Оценок пока нет
- Surgical Extrusion: A Dental TechniqueДокумент6 страницSurgical Extrusion: A Dental TechniqueDragos CiongaruОценок пока нет
- Preoperative Diagnosis of A Third Root Canal in First and Second Maxillary Premolars A Challenge For The ClinicianДокумент7 страницPreoperative Diagnosis of A Third Root Canal in First and Second Maxillary Premolars A Challenge For The ClinicianS S Saad SaadОценок пока нет
- New Microsoft Office Word DocumentДокумент3 страницыNew Microsoft Office Word DocumentAtulsanapОценок пока нет
- Relining and Rebasing of Complete DentureДокумент7 страницRelining and Rebasing of Complete DentureAdinda YokoОценок пока нет
- Restoration of THE Endodonticall Y Treated Tooth: Amith Babu Amrita Dora Ganesh O.R Praveen J Ourvind SinghДокумент100 страницRestoration of THE Endodonticall Y Treated Tooth: Amith Babu Amrita Dora Ganesh O.R Praveen J Ourvind SinghCahyani CahyaniОценок пока нет
- Infection Control in Fixed Prosthodontics: Prepared & Presented byДокумент57 страницInfection Control in Fixed Prosthodontics: Prepared & Presented byaloooooooshОценок пока нет
- Failures in FPDДокумент30 страницFailures in FPDMayank Aggarwal100% (1)
- Single Complete DenturesДокумент20 страницSingle Complete DenturesDeepthi RajeshОценок пока нет
- ProsthoДокумент59 страницProsthoramОценок пока нет
- Curriculum Vitae: Personal DetailsДокумент3 страницыCurriculum Vitae: Personal DetailsBibek RajОценок пока нет
- When Is Oral Biopsy Not Needed?Документ6 страницWhen Is Oral Biopsy Not Needed?Bibek RajОценок пока нет
- For Mucocele Lesions - Careful Excisional BiopsyДокумент11 страницFor Mucocele Lesions - Careful Excisional BiopsyBibek RajОценок пока нет
- QDWPlicДокумент2 страницыQDWPlicBibek RajОценок пока нет
- 3 UhnjkcДокумент8 страниц3 UhnjkcBibek RajОценок пока нет
- JdsmcxnksДокумент32 страницыJdsmcxnksBibek RajОценок пока нет
- Inflammation: Presenter: Priyanka Shah Junior Resident Department of Pedodontics and Preventive DentistryДокумент73 страницыInflammation: Presenter: Priyanka Shah Junior Resident Department of Pedodontics and Preventive DentistryBibek RajОценок пока нет
- Background Methods: Review' (OHAR) Guidance in BriefДокумент1 страницаBackground Methods: Review' (OHAR) Guidance in BriefBibek RajОценок пока нет
- Biopsy Is Derived From A Greek Word (By-Op-See) Bio - Meaning LIFE and Opsy - TO LOOK (Vision)Документ5 страницBiopsy Is Derived From A Greek Word (By-Op-See) Bio - Meaning LIFE and Opsy - TO LOOK (Vision)Bibek RajОценок пока нет
- Practical Skill Station Basic Life Support Key Teaching ObjectivesДокумент3 страницыPractical Skill Station Basic Life Support Key Teaching ObjectivesBibek RajОценок пока нет
- Trapezoidal Flap. A Diagrammatic IllustrationДокумент6 страницTrapezoidal Flap. A Diagrammatic IllustrationBibek RajОценок пока нет
- DhdifogkДокумент4 страницыDhdifogkBibek RajОценок пока нет
- JDJDJDJДокумент23 страницыJDJDJDJBibek RajОценок пока нет
- DrtfygbyuijДокумент29 страницDrtfygbyuijBibek RajОценок пока нет
- Vitamin B-Functions, Food Sources and RDA Value Deficiency and Their Oral ManifestationsДокумент6 страницVitamin B-Functions, Food Sources and RDA Value Deficiency and Their Oral ManifestationsBibek RajОценок пока нет
- Background Triads Framework: Jan Clarkson, Craig Ramsay, Linda Young, Paula Elouafkaoui and Heather CassieДокумент1 страницаBackground Triads Framework: Jan Clarkson, Craig Ramsay, Linda Young, Paula Elouafkaoui and Heather CassieBibek RajОценок пока нет
- YuybnunhhuhbДокумент2 страницыYuybnunhhuhbBibek RajОценок пока нет
- FfghhthjgvyujhДокумент1 страницаFfghhthjgvyujhBibek RajОценок пока нет
- Ultrasonic Cleaner Test Record: Ultrasonic Serial Number - LocationДокумент2 страницыUltrasonic Cleaner Test Record: Ultrasonic Serial Number - LocationBibek RajОценок пока нет
- YudsbhcjДокумент1 страницаYudsbhcjBibek RajОценок пока нет
- Rapid: Reducing Antibiotic Prescribing in DentistryДокумент5 страницRapid: Reducing Antibiotic Prescribing in DentistryBibek RajОценок пока нет
- TG 6 YhunjДокумент48 страницTG 6 YhunjBibek RajОценок пока нет
- Warfarin and Your Dental Treatment: Information For PatientsДокумент5 страницWarfarin and Your Dental Treatment: Information For PatientsBibek RajОценок пока нет
- Toothbrushing Chart PDFДокумент1 страницаToothbrushing Chart PDFBibek RajОценок пока нет
- Dental Anxiety Form 4 PDFДокумент2 страницыDental Anxiety Form 4 PDFBibek RajОценок пока нет
- VfyggdbДокумент33 страницыVfyggdbBibek RajОценок пока нет
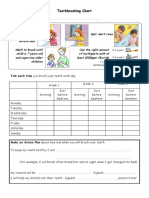
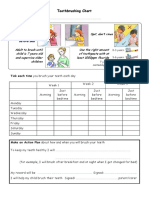
- Toothbrushing Chart: Tick Each Time You Brush Your Teeth Each DayДокумент1 страницаToothbrushing Chart: Tick Each Time You Brush Your Teeth Each DayBibek RajОценок пока нет
- Acrylic Allergies InformationДокумент7 страницAcrylic Allergies Informationdrgayen6042Оценок пока нет
- Management of Alveolar Ridge ResorptionДокумент29 страницManagement of Alveolar Ridge Resorptionفواز نميرОценок пока нет
- Single Complete DentureДокумент20 страницSingle Complete DentureNelly SuriamahОценок пока нет
- File 925Документ26 страницFile 925SadishОценок пока нет
- Complete Dentures - Extraoral ExamДокумент8 страницComplete Dentures - Extraoral ExamlindaОценок пока нет
- Analysis of Resistance and Retention of Complete Veneer Crown RetainersДокумент8 страницAnalysis of Resistance and Retention of Complete Veneer Crown Retainerssara luciaОценок пока нет
- Specific Examination (Prostho 3 - Complete Denture (Lec)Документ3 страницыSpecific Examination (Prostho 3 - Complete Denture (Lec)Leigh BelmonteОценок пока нет
- Different Pontic DesignДокумент5 страницDifferent Pontic DesignHassanein Al-HamdaniОценок пока нет
- Healthy Smiles Implant Patient Surgery Information and Consent FormДокумент3 страницыHealthy Smiles Implant Patient Surgery Information and Consent FormAnup Lal RajbahakОценок пока нет
- web-VALPLAST PDFДокумент2 страницыweb-VALPLAST PDFHendra AzhariОценок пока нет
- 5 Direct RetainersДокумент56 страниц5 Direct RetainersKandiwapa ShivuteОценок пока нет
- Practical, Esthetic Options For Retention of Removable Partial Dentnres: A Case ReportДокумент8 страницPractical, Esthetic Options For Retention of Removable Partial Dentnres: A Case ReportHusnul KhatimahОценок пока нет
- Articulators ProsthoДокумент91 страницаArticulators ProsthoFourthMolar.com0% (1)
- The Initial Interview With Complete-Denture Patients. ITs Structure and StrategyДокумент8 страницThe Initial Interview With Complete-Denture Patients. ITs Structure and Strategyjorefe12Оценок пока нет
- 2015Документ45 страниц2015jimmyОценок пока нет
- Neutral Zone Dentures Versus Conventional Dentures in Diverse Edentulous PeriodsДокумент10 страницNeutral Zone Dentures Versus Conventional Dentures in Diverse Edentulous Periodsizeldien5870Оценок пока нет
- CBL EnglishДокумент15 страницCBL EnglishRohma DwiОценок пока нет
- Talkabout Great Sutton & Little Sutton April 2020Документ36 страницTalkabout Great Sutton & Little Sutton April 2020Talkabout PublishingОценок пока нет
- Partially Dentate PatientДокумент55 страницPartially Dentate PatientAhmed SamirОценок пока нет
- 6 Regestration Ii PDFДокумент6 страниц6 Regestration Ii PDFmahmoudОценок пока нет
- Diagnosis and Treatment Planning in FPDДокумент109 страницDiagnosis and Treatment Planning in FPDvergel john ErciaОценок пока нет