Вам также может понравиться
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Method For Ultra High Purity Gold - Gold Refining ForumДокумент11 страницMethod For Ultra High Purity Gold - Gold Refining Forummladen lakic100% (1)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- OctaveДокумент2 страницыOctaveDavid CovatzinОценок пока нет
- V 1 Preparation of AZ31 Magnesium Alloy Strips Using Vertical Twin-Roll CasterДокумент7 страницV 1 Preparation of AZ31 Magnesium Alloy Strips Using Vertical Twin-Roll CasterVidya me20d015Оценок пока нет
- Hemodialysis Medical Supply and MedicationДокумент10 страницHemodialysis Medical Supply and Medicationsiuagan.jayveeОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Nanofabrication For Pattern Transfer Purpose.: Etching Is Done Either in "Dry" or "Wet" MethodsДокумент19 страницNanofabrication For Pattern Transfer Purpose.: Etching Is Done Either in "Dry" or "Wet" MethodsPRAVEEN MОценок пока нет
- 50 Easy and Free FertilizersДокумент12 страниц50 Easy and Free FertilizersScott Odam100% (1)
- Perkins 1104D (Mech) EngineДокумент140 страницPerkins 1104D (Mech) EngineAnonymous yjK3peI787% (15)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Panchakanya Structural SteelДокумент5 страницPanchakanya Structural Steelkabira12Оценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- A Clear & Present Danger 2 - The Use of QT or TMT Rebars in Seismic Zone 4Документ12 страницA Clear & Present Danger 2 - The Use of QT or TMT Rebars in Seismic Zone 4friends_y2k5Оценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Tugas 1 PPAДокумент29 страницTugas 1 PPAlulalalaОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- 2023 Microalgae Application To Bone Repairing Process - A ReviewДокумент19 страниц2023 Microalgae Application To Bone Repairing Process - A ReviewvirgiparedesОценок пока нет
- Astm G200 - 09Документ4 страницыAstm G200 - 09Sofia YuliОценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- 70 Penetration Grade BitumenДокумент1 страница70 Penetration Grade BitumenJohn SnowОценок пока нет
- Light ExperimentsДокумент12 страницLight ExperimentsmamosОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Newport E360 Ventilator - Service ManualДокумент76 страницNewport E360 Ventilator - Service ManualSHIRLEY GIRALDOОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- ASTM Method D5134-92Документ1 страницаASTM Method D5134-92Sylab InstrumentsОценок пока нет
- 3075-Article Text-9088-1-10-20201218Документ11 страниц3075-Article Text-9088-1-10-20201218Rasdawati RasulОценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Experimental Detemination of Crystal StructureДокумент40 страницExperimental Detemination of Crystal StructureAASHIR AHMAD JASKANIОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Embuild BrochureДокумент38 страницEmbuild BrochureKawish TamourОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Astm d1785Документ5 страницAstm d1785Kehinde AdebayoОценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Insulation System ClassДокумент2 страницыInsulation System ClassVictor Hutahaean100% (1)
- Ramabulana Et Al. 2021 MN and MetPA - Chemical Space of Four Momordica Plant SpeciesДокумент15 страницRamabulana Et Al. 2021 MN and MetPA - Chemical Space of Four Momordica Plant SpeciesFernanda SantosОценок пока нет
- Stopac Outer Wrap PE PDS-Stopaq-Outerwrap-PE-V8-ENДокумент2 страницыStopac Outer Wrap PE PDS-Stopaq-Outerwrap-PE-V8-ENvaradarajck893Оценок пока нет
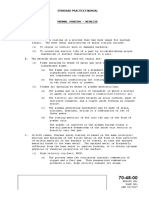
- CFM SPM 70-48-00Документ8 страницCFM SPM 70-48-00ZakiHaunaОценок пока нет
- Evaporation Rate of Solvents PDFДокумент2 страницыEvaporation Rate of Solvents PDFsyamlokОценок пока нет
- Bateria Data PDFДокумент2 страницыBateria Data PDFJulian GuascalОценок пока нет
- Msds FormaldehydeДокумент6 страницMsds Formaldehydemkhurram79Оценок пока нет
- Chemistry Investigatory Project On BrownДокумент14 страницChemistry Investigatory Project On BrownVidya GОценок пока нет
- Nitobond SBR PDFДокумент4 страницыNitobond SBR PDFhelloitskalaiОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- 006-MS For Purging of Stainless Steel PDFДокумент18 страниц006-MS For Purging of Stainless Steel PDFKöksal PatanОценок пока нет