Вам также может понравиться
- Complementary and Alternative Medical Lab Testing Part 12: NeurologyОт EverandComplementary and Alternative Medical Lab Testing Part 12: NeurologyОценок пока нет
- Alteración Del Sueño en El Trastorno Adaptativo y El Episodio DepresivoДокумент11 страницAlteración Del Sueño en El Trastorno Adaptativo y El Episodio DepresivoPABLOОценок пока нет
- Definition of InsomniaДокумент10 страницDefinition of Insomniaeka yusrianaОценок пока нет
- Correlates of General Quality of Life Are Different in Patients With Primary Insomnia As Compared To Patients With Insomnia and Psychiatric ComorbidityДокумент13 страницCorrelates of General Quality of Life Are Different in Patients With Primary Insomnia As Compared To Patients With Insomnia and Psychiatric ComorbidityVictor CarrenoОценок пока нет
- Cannabis Paper 2Документ6 страницCannabis Paper 2Carlos Eduardo Jorquera GonzálezОценок пока нет
- Swinkels PscychopathologieДокумент16 страницSwinkels PscychopathologiesezalwickОценок пока нет
- The Association Between Insomnia and Cardiovascular DiseasesДокумент8 страницThe Association Between Insomnia and Cardiovascular Diseasesnouval_iqbalОценок пока нет
- Original Paper Comorbidity of Epilepsy and Depression in Al Husseini Teaching Hospital in Holy Kerbala /iraq in 2018Документ9 страницOriginal Paper Comorbidity of Epilepsy and Depression in Al Husseini Teaching Hospital in Holy Kerbala /iraq in 2018sarhang talebaniОценок пока нет
- Epilepsia y AnsiedadДокумент10 страницEpilepsia y AnsiedadNCОценок пока нет
- JCSM 11 9 1029 PDFДокумент10 страницJCSM 11 9 1029 PDFNonoОценок пока нет
- Bruno 2013Документ7 страницBruno 2013Ferdy LainsamputtyОценок пока нет
- Sleep Medicine: Amparo Díaz-Román, Lilisbeth Perestelo-Pérez, Gualberto Buela-CasalДокумент7 страницSleep Medicine: Amparo Díaz-Román, Lilisbeth Perestelo-Pérez, Gualberto Buela-CasalRavennaОценок пока нет
- Fatigue in A Cohort of Geriatric Patients With and Without Parkinson's DiseaseДокумент5 страницFatigue in A Cohort of Geriatric Patients With and Without Parkinson's DiseaseOcisa ZakiahОценок пока нет
- Salud Mental y Calidad de Sueño Ene Studiantes de Ocho Facultades de Medicina Humana Del PerúДокумент10 страницSalud Mental y Calidad de Sueño Ene Studiantes de Ocho Facultades de Medicina Humana Del PerúPsico29Оценок пока нет
- Insomnia HipertensiДокумент11 страницInsomnia HipertensiKondang WarasОценок пока нет
- The Diagnosis and Treatment of Chronic Insomnia in Adults: EditorialДокумент2 страницыThe Diagnosis and Treatment of Chronic Insomnia in Adults: EditorialFiddien InderaОценок пока нет
- Sleep DisorderДокумент6 страницSleep DisorderNurul FajriОценок пока нет
- Sleep Quality and Associated Factors in Hemodialysis PatientsДокумент8 страницSleep Quality and Associated Factors in Hemodialysis PatientsChristina NovarinОценок пока нет
- Accepted Manuscript: Epilepsy ResearchДокумент24 страницыAccepted Manuscript: Epilepsy Researchmohamad safiiОценок пока нет
- NIH Public Access: Author ManuscriptДокумент16 страницNIH Public Access: Author ManuscriptFika Tri NandaОценок пока нет
- BMC Psychiatry: Thyroid Function in Clinical Subtypes of Major Depression: An Exploratory StudyДокумент9 страницBMC Psychiatry: Thyroid Function in Clinical Subtypes of Major Depression: An Exploratory StudyTRTETDX TETDОценок пока нет
- Emergency Delirium in PediatricДокумент15 страницEmergency Delirium in PediatricUzZySusFabregasОценок пока нет
- Comorbid Insomnia and Obstructive Sleep Apnea: Challenges For Clinical Practice and ResearchДокумент9 страницComorbid Insomnia and Obstructive Sleep Apnea: Challenges For Clinical Practice and ResearchIriawan Indra PutraОценок пока нет
- Anxiety and Mood Disorders in Narcolepsy: A Case - Control StudyДокумент8 страницAnxiety and Mood Disorders in Narcolepsy: A Case - Control StudyDesyifa Annisa MursalinОценок пока нет
- Introduction CorrectionsДокумент2 страницыIntroduction Correctionsfarkad falihОценок пока нет
- Prospective 10-Year Follow-Up in Adolescent Anorexia Nervosa-Course, Outcome, Psychiatric Comorbidity, and Psychosocial AdaptationДокумент10 страницProspective 10-Year Follow-Up in Adolescent Anorexia Nervosa-Course, Outcome, Psychiatric Comorbidity, and Psychosocial AdaptationCătălina LunguОценок пока нет
- Sleep Problems and Disorders Among Adolescents With Persistent and Subthreshold Attention-deficit/Hyperactivity DisordersДокумент9 страницSleep Problems and Disorders Among Adolescents With Persistent and Subthreshold Attention-deficit/Hyperactivity DisordersdentistwaseemОценок пока нет
- 2006 Association of Usual Sleep Duration With Hypertension The Sleep Heart Health StudyДокумент6 страниц2006 Association of Usual Sleep Duration With Hypertension The Sleep Heart Health Study丁崝Оценок пока нет
- Paper - Night - Eating - Syndrome - in - Young - Adults - de 17-7-2021Документ8 страницPaper - Night - Eating - Syndrome - in - Young - Adults - de 17-7-2021Cristóbal Cortázar MorizonОценок пока нет
- Associations of Heart Failure With Sleep Quality: The Rotterdam StudyДокумент6 страницAssociations of Heart Failure With Sleep Quality: The Rotterdam StudySheryl ElitaОценок пока нет
- Insomnia and Excessive Daytime Sleepiness in ObstrДокумент3 страницыInsomnia and Excessive Daytime Sleepiness in ObstrChatterjee SomanОценок пока нет
- Jurnal 1 PDFДокумент6 страницJurnal 1 PDFNicoYansenОценок пока нет
- Zandian (2007) Cause and Treatment of Anorexia NervosaДокумент8 страницZandian (2007) Cause and Treatment of Anorexia NervosaRenzo LanfrancoОценок пока нет
- Comorbidity Between Sleep Apnea and InsomniaДокумент7 страницComorbidity Between Sleep Apnea and InsomniaMaria Jose YevenesОценок пока нет
- Sleep: Depression and Insomnia: Questions of Cause and EffectДокумент10 страницSleep: Depression and Insomnia: Questions of Cause and EffectAnonymous l3X3jf0NPОценок пока нет
- 2010 - Juliana-Methods For Increasing Upper Airway Muscle TonusДокумент7 страниц2010 - Juliana-Methods For Increasing Upper Airway Muscle TonusGoongGiing MatinaОценок пока нет
- Chronic Fatigue Syndrome: Diagnosis and TreatmentДокумент6 страницChronic Fatigue Syndrome: Diagnosis and TreatmentHitesh VermaОценок пока нет
- The Diagnosis and Management of Insomnia in Clinical Practice: A Practical Evidence-Based ApproachДокумент5 страницThe Diagnosis and Management of Insomnia in Clinical Practice: A Practical Evidence-Based ApproachanzzunОценок пока нет
- Restless Legs Syndrome in Adult Patients With Obstructive Sleep ApneaДокумент10 страницRestless Legs Syndrome in Adult Patients With Obstructive Sleep ApneaBruna PinheirosОценок пока нет
- Effect of Depression On SleepДокумент19 страницEffect of Depression On SleepLia Noor AnggrainiОценок пока нет
- Stigma, Seizure Frequency and Quality of Life: The Impact of Epilepsy in Late AdulthoodДокумент7 страницStigma, Seizure Frequency and Quality of Life: The Impact of Epilepsy in Late AdulthoodTony DurãoОценок пока нет
- Exercise and Sleep-Disordered Breathing: An Association Independent of Body HabitusДокумент5 страницExercise and Sleep-Disordered Breathing: An Association Independent of Body HabitusponnuswamyvОценок пока нет
- Roth2007 PDFДокумент9 страницRoth2007 PDFmeiutaОценок пока нет
- Privação Do SonoДокумент3 страницыPrivação Do SonoHugo BarbosaОценок пока нет
- Bansil Et Al-2011-The Journal of Clinical HypertensionДокумент5 страницBansil Et Al-2011-The Journal of Clinical HypertensionFika Tri NandaОценок пока нет
- Epidemiology of Insomnia, Depression, and AnxietyДокумент8 страницEpidemiology of Insomnia, Depression, and AnxietyMarina OpreaОценок пока нет
- Psychosocial Adjustment To Illness ScaleДокумент12 страницPsychosocial Adjustment To Illness ScaleABD.NASIRОценок пока нет
- Association of Gastroesophageal Reflux Disease With Anxiety, Depression, and Sleep Disorders Original ArticleДокумент8 страницAssociation of Gastroesophageal Reflux Disease With Anxiety, Depression, and Sleep Disorders Original Articlebarokahgroup groupОценок пока нет
- The Role of Psychotropic Medications in The ManagementДокумент24 страницыThe Role of Psychotropic Medications in The ManagementloloasbОценок пока нет
- TDAH Sono PDFДокумент9 страницTDAH Sono PDFAlberto José Correia RamosОценок пока нет
- Original Papers: The Lifetime Prevalence of Anxiety Disorders Among Patients With Irritable Bowel SyndromeДокумент6 страницOriginal Papers: The Lifetime Prevalence of Anxiety Disorders Among Patients With Irritable Bowel Syndromeapi-193771047Оценок пока нет
- Residual Sleep DisturbancesДокумент9 страницResidual Sleep DisturbancesEstefanía ChávezОценок пока нет
- The Health Anxiety Inventory - Development and Validation of Scales For The Measurement of Health Anxiety and Hypochondriasis 2002Документ11 страницThe Health Anxiety Inventory - Development and Validation of Scales For The Measurement of Health Anxiety and Hypochondriasis 2002Catalina NedelciuОценок пока нет
- Chest 147 4 1179Документ14 страницChest 147 4 1179Albert TandyОценок пока нет
- Insomnia and Depression: Original ArticleДокумент7 страницInsomnia and Depression: Original ArticleFlorina AnichitoaeОценок пока нет
- ESCALA de Somnolencia de Epworth en Un Centro de Salud FamiliarДокумент10 страницESCALA de Somnolencia de Epworth en Un Centro de Salud FamiliarEnith VilelaОценок пока нет
- Psychosomatic Aspects in Idiopathic Infertility: Effects of Treatment With Autogenic TrainingДокумент7 страницPsychosomatic Aspects in Idiopathic Infertility: Effects of Treatment With Autogenic TrainingMayrá LobatoОценок пока нет
- Aspek Psikiatrik Pada Penderita SLEДокумент119 страницAspek Psikiatrik Pada Penderita SLETami JebaОценок пока нет
- Tiara-Dr - Ingrid English 3 (I)Документ14 страницTiara-Dr - Ingrid English 3 (I)Krisna HerdiyantoОценок пока нет
- SCH Man Detal 2011Документ6 страницSCH Man Detal 2011sonoiochecomandoОценок пока нет
- A Mechanism For Impaired Fear Recognition After Amygdala DamageДокумент6 страницA Mechanism For Impaired Fear Recognition After Amygdala DamagesonoiochecomandoОценок пока нет
- Article DCL 2008 - 13p PDFДокумент17 страницArticle DCL 2008 - 13p PDFsonoiochecomandoОценок пока нет
- Article DCL 2008 - 13p PDFДокумент17 страницArticle DCL 2008 - 13p PDFsonoiochecomandoОценок пока нет
- Left Temporoparietal Junction Is Necessary For Representing Somone Else's BeliefДокумент3 страницыLeft Temporoparietal Junction Is Necessary For Representing Somone Else's BeliefsonoiochecomandoОценок пока нет
- Harciareketal 2011Документ17 страницHarciareketal 2011sonoiochecomandoОценок пока нет
- Applying Skinner's Analysis of Verbal Behavior To Persons With DementiaДокумент21 страницаApplying Skinner's Analysis of Verbal Behavior To Persons With DementiasonoiochecomandoОценок пока нет
- Brain 2001 Rowe 600 16Документ17 страницBrain 2001 Rowe 600 16sonoiochecomandoОценок пока нет
- The Frequency, Clinical Correlates, and Mechanism of Anosognosia After Stroke.Документ8 страницThe Frequency, Clinical Correlates, and Mechanism of Anosognosia After Stroke.sonoiochecomandoОценок пока нет
- Differences in Cognitive Performance, Level of Dependency and Quality of Life (QoL), Related To Age and Cognitive StatusДокумент6 страницDifferences in Cognitive Performance, Level of Dependency and Quality of Life (QoL), Related To Age and Cognitive StatussonoiochecomandoОценок пока нет
- Angry Responses To Emotional Events. The Role of Impaired Control and Drive in People With Severe Traumatic Brain Injury.Документ11 страницAngry Responses To Emotional Events. The Role of Impaired Control and Drive in People With Severe Traumatic Brain Injury.sonoiochecomandoОценок пока нет
- Anosognosia For Memory Deficit in Amnestic Mild Cognitive Impairment and Alzheimer's DiseaseДокумент8 страницAnosognosia For Memory Deficit in Amnestic Mild Cognitive Impairment and Alzheimer's DiseasesonoiochecomandoОценок пока нет
- Alzheimer in Down SyndromeДокумент12 страницAlzheimer in Down SyndromesonoiochecomandoОценок пока нет
- Assessment and Approach of Patients With Severe Dementia: by Bernard Groulx, MD, FRCPCДокумент4 страницыAssessment and Approach of Patients With Severe Dementia: by Bernard Groulx, MD, FRCPCsonoiochecomandoОценок пока нет
- Retrieval Monitoring and Anosohgnosia in Alzheimer's Disease.Документ10 страницRetrieval Monitoring and Anosohgnosia in Alzheimer's Disease.sonoiochecomandoОценок пока нет
- Disentangling Alzheimer's Disease Duyckaerts Lancet 07.11Документ2 страницыDisentangling Alzheimer's Disease Duyckaerts Lancet 07.11sonoiochecomandoОценок пока нет
- Why Are Drug Trials in AD Failing Dsmith LancetДокумент1 страницаWhy Are Drug Trials in AD Failing Dsmith LancetsonoiochecomandoОценок пока нет
- Two Dimensions of Anosognosia in Patients With Alzheimer's Disease. Reliability and Validity of The Japanese Version of The Anosognosia Questionnaire For Dementia (AQ-D)Документ7 страницTwo Dimensions of Anosognosia in Patients With Alzheimer's Disease. Reliability and Validity of The Japanese Version of The Anosognosia Questionnaire For Dementia (AQ-D)sonoiochecomandoОценок пока нет
- Cognitive Advantages of Chewing GumДокумент34 страницыCognitive Advantages of Chewing GumsonoiochecomandoОценок пока нет
- Compounding Artefacjkjkts With Uncertainty, and An Amyloid Cascade Hypothesis Too Big To FailДокумент6 страницCompounding Artefacjkjkts With Uncertainty, and An Amyloid Cascade Hypothesis Too Big To FailsonoiochecomandoОценок пока нет
- Decreased Awareness of Cognitive Deficits in Patients With Mild Dementia of The Alzheimer Type.Документ13 страницDecreased Awareness of Cognitive Deficits in Patients With Mild Dementia of The Alzheimer Type.sonoiochecomandoОценок пока нет
- Cognitive and Functional Neuroimaging Correlates For Anosognosia in Mild Cognitive Impairment and Alzheimer's DiseaseДокумент10 страницCognitive and Functional Neuroimaging Correlates For Anosognosia in Mild Cognitive Impairment and Alzheimer's DiseasesonoiochecomandoОценок пока нет
- Relationship Between Cognition and Awareness of Deficit in Mild Cognitive Impairment.Документ9 страницRelationship Between Cognition and Awareness of Deficit in Mild Cognitive Impairment.sonoiochecomandoОценок пока нет
- The Frequency, Clinical Correlates, and Mechanism of Anosognosia After Stroke.Документ8 страницThe Frequency, Clinical Correlates, and Mechanism of Anosognosia After Stroke.sonoiochecomandoОценок пока нет
- Yes PenizeДокумент7 страницYes PenizesonoiochecomandoОценок пока нет
- Sumerians Elamites Egyptians: AmoritesДокумент5 страницSumerians Elamites Egyptians: AmoritessonoiochecomandoОценок пока нет
- ITECH1000 Assignment1 Specification Sem22014Документ6 страницITECH1000 Assignment1 Specification Sem22014Nitin KumarОценок пока нет
- EP 1110-1-8 Vo2 PDFДокумент501 страницаEP 1110-1-8 Vo2 PDFyodiumhchltОценок пока нет
- Slip Rings: SRI085 V100 - XX - XX - Xxx1XxДокумент3 страницыSlip Rings: SRI085 V100 - XX - XX - Xxx1XxMatheus Henrique MattiaОценок пока нет
- Ethoxy 1Документ77 страницEthoxy 1HoshiОценок пока нет
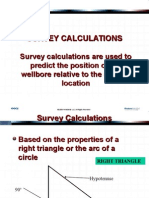
- 02 Survey Calculations - PpsДокумент96 страниц02 Survey Calculations - PpsLeo Ivan Aviles RicaldiОценок пока нет
- AlgebraДокумент66 страницAlgebraOliseyenum Precious ChukuemekeОценок пока нет
- Tutorial 1 SolutionsДокумент4 страницыTutorial 1 Solutionsteju1996coolОценок пока нет
- Creating Attachments To Work Items or To User Decisions in WorkflowsДокумент20 страницCreating Attachments To Work Items or To User Decisions in Workflowselampe100% (1)
- Business Analytics Data Analysis and Decision Making 6th Edition Albright Solutions ManualДокумент24 страницыBusiness Analytics Data Analysis and Decision Making 6th Edition Albright Solutions ManualAngelaLewisyqza100% (26)
- General Pathology Lecture Group 1 HandoutДокумент6 страницGeneral Pathology Lecture Group 1 HandoutCecille AnnОценок пока нет
- Solution Manual For Introductory Statistics 9th Edition by Mann Chapters 1 13 PDFДокумент10 страницSolution Manual For Introductory Statistics 9th Edition by Mann Chapters 1 13 PDFa40095824643% (14)
- Air Movements 06-26-2019 - Full ScoreДокумент5 страницAir Movements 06-26-2019 - Full ScoreMichael CrawfordОценок пока нет
- Cep MPДокумент1 страницаCep MPAzmat HabeebОценок пока нет
- API2000 Tank Venting CalcsДокумент5 страницAPI2000 Tank Venting Calcsruhul01Оценок пока нет
- SC Perthub Single Cell OmicsДокумент34 страницыSC Perthub Single Cell OmicsGANYA U 2022 Batch,PES UniversityОценок пока нет
- Data Mining ConceptsДокумент175 страницData Mining ConceptsNikolya SmirnoffОценок пока нет
- Cleats CatalogueДокумент73 страницыCleats Cataloguefire123123Оценок пока нет
- Urban Road Types 25.01.2022Документ5 страницUrban Road Types 25.01.2022Balogun IbrahimОценок пока нет
- A Simulation-Based Process Model For Managing Complex Design ProcessДокумент13 страницA Simulation-Based Process Model For Managing Complex Design ProcessMetehan AgacaОценок пока нет
- Pneumatic Conveying of Bulk Solids PDFДокумент231 страницаPneumatic Conveying of Bulk Solids PDFCarloLopez100% (2)
- Che 410 ................... Transition Metal ChemistryДокумент13 страницChe 410 ................... Transition Metal ChemistryElizabeth AnyangoОценок пока нет
- Watchgas AirWatch MK1.0 Vs MK1.2Документ9 страницWatchgas AirWatch MK1.0 Vs MK1.2elliotmoralesОценок пока нет
- L4 Subdivision of PlotsДокумент20 страницL4 Subdivision of PlotsKenny BoatОценок пока нет
- Microprocessor I - Lecture 01Документ27 страницMicroprocessor I - Lecture 01Omar Mohamed Farag Abd El FattahОценок пока нет
- 9Y011-02704 KubotaДокумент143 страницы9Y011-02704 KubotaZaqi SatchОценок пока нет
- GTG - TFA Belt DrivenДокумент2 страницыGTG - TFA Belt Drivensuan170Оценок пока нет
- Bootloader3 PDFДокумент18 страницBootloader3 PDFsaravananОценок пока нет
- Three - Dimensional Viscous Confinement and Cooling of Atoms by Resonance Radiation PressureДокумент6 страницThree - Dimensional Viscous Confinement and Cooling of Atoms by Resonance Radiation PressureWenjun ZhangОценок пока нет
- Stellar Evolution SimulationДокумент2 страницыStellar Evolution Simulationncl12142Оценок пока нет
- P 130881757895329843Документ44 страницыP 130881757895329843Vijay MohanОценок пока нет