Вам также может понравиться
- RSW in LBP RCTДокумент10 страницRSW in LBP RCTNakarit SangsirinawinОценок пока нет
- Peripheral and Central Adaptations After A Median Nerve Neuromobilization Program Completed by Individuals With Carpal Tunnel SyndromeДокумент13 страницPeripheral and Central Adaptations After A Median Nerve Neuromobilization Program Completed by Individuals With Carpal Tunnel SyndromeRafael MoreiraОценок пока нет
- Bougea 2013Документ9 страницBougea 2013Lia YulianiОценок пока нет
- Gray 2014Документ10 страницGray 2014Nada MachichОценок пока нет
- Controlled Study of Neuroprosthetic Functional Electrical Stimulation in Sub-Acute Post-Stroke RehabilitationДокумент5 страницControlled Study of Neuroprosthetic Functional Electrical Stimulation in Sub-Acute Post-Stroke RehabilitationAiry MercadoОценок пока нет
- Science IntegrationДокумент11 страницScience IntegrationDiego ElíasОценок пока нет
- Kelompok 2Документ23 страницыKelompok 2lutfiah nabilahОценок пока нет
- Agopuntura Per StrokeДокумент14 страницAgopuntura Per StrokeAngela PagliusoОценок пока нет
- Current Trends Stroke Rehabilitation JohanssonДокумент13 страницCurrent Trends Stroke Rehabilitation Johanssonsidney drecotteОценок пока нет
- Acupuncture Therapy in Ischemic Stroke RehabilitationДокумент12 страницAcupuncture Therapy in Ischemic Stroke RehabilitationcocosinghОценок пока нет
- YNSAДокумент8 страницYNSAGracielle VasconcelosОценок пока нет
- Research Article: Yu Zheng, Jiping Zhang, Yanjie Wang, Yuying Wang, Yujun Lan, Shanshan Qu, Chunzhi Tang, and Yong HuangДокумент10 страницResearch Article: Yu Zheng, Jiping Zhang, Yanjie Wang, Yuying Wang, Yujun Lan, Shanshan Qu, Chunzhi Tang, and Yong Huangmazh21Оценок пока нет
- Effects of Repeated Anodal TDCS Coupled With Cognitive Training For Patients With Severe Traumatic Brain Injury: A Pilot Randomized Controlled TrialДокумент10 страницEffects of Repeated Anodal TDCS Coupled With Cognitive Training For Patients With Severe Traumatic Brain Injury: A Pilot Randomized Controlled TrialAmandaОценок пока нет
- Exercise and Neuropathic Pain: A General Overview of Preclinical and Clinical ResearchДокумент16 страницExercise and Neuropathic Pain: A General Overview of Preclinical and Clinical ResearchderisonmarsinovabakaraОценок пока нет
- 27 InhibitoryДокумент18 страниц27 InhibitoryrogerОценок пока нет
- How Fast Pain, Numbness, and Paresthesia Resolves After Lumbar Nerve Root DecompressionДокумент8 страницHow Fast Pain, Numbness, and Paresthesia Resolves After Lumbar Nerve Root DecompressioniswaraОценок пока нет
- Quality of Life and Traumatic Spinal Cord Injury: Ninni Westgren, CNM, Richard Levi, MD, PHDДокумент7 страницQuality of Life and Traumatic Spinal Cord Injury: Ninni Westgren, CNM, Richard Levi, MD, PHDDrDevanshi DesaiОценок пока нет
- Hyperbaric Oxygen Therapy Improves Symptoms, Brain's Microstructure and Functionality in Veterans With Treatment Resistant Post-Traumatic Stress Disorder - A Prospective, Randomized, Controlled TrialДокумент21 страницаHyperbaric Oxygen Therapy Improves Symptoms, Brain's Microstructure and Functionality in Veterans With Treatment Resistant Post-Traumatic Stress Disorder - A Prospective, Randomized, Controlled Trialitziar luceñoОценок пока нет
- Efectividad de La Fisio en EspasticidadДокумент58 страницEfectividad de La Fisio en EspasticidadAbner SánchezОценок пока нет
- Multiple Sessions of Transcranial Direct Current Stimulation and Upperextremity Rehab in StrokeДокумент10 страницMultiple Sessions of Transcranial Direct Current Stimulation and Upperextremity Rehab in StrokelabsoneducationОценок пока нет
- Su Jok Stress PDFДокумент10 страницSu Jok Stress PDFghhy100% (4)
- Gait Disorders: Editorial CommentaryДокумент2 страницыGait Disorders: Editorial CommentaryAffan AdibОценок пока нет
- J JBMT 2014 01 001Документ10 страницJ JBMT 2014 01 001yoverОценок пока нет
- Velasco 2008Документ9 страницVelasco 2008moiОценок пока нет
- Influence of The Generation of Motor Mental Images On Physiotherapy Treatment in Patients With Chronic Low Back PainДокумент13 страницInfluence of The Generation of Motor Mental Images On Physiotherapy Treatment in Patients With Chronic Low Back PainPaulomds1991Оценок пока нет
- Aplicaciones Clínicas de La DbsДокумент10 страницAplicaciones Clínicas de La DbsTARОценок пока нет
- Acupuncture Protocols For Shen DisordersДокумент168 страницAcupuncture Protocols For Shen Disorderstito zambranoОценок пока нет
- Acupuncture and StrokeДокумент13 страницAcupuncture and StrokeSeriusОценок пока нет
- Electrical Stimulation in The Management of Spasticity: A ReviewДокумент5 страницElectrical Stimulation in The Management of Spasticity: A ReviewArkar SoeОценок пока нет
- Cognitive Outcomes in Patients With Major Depression Treated With Electroconvulsive TherapyДокумент8 страницCognitive Outcomes in Patients With Major Depression Treated With Electroconvulsive TherapyPsiholog Monica StănescuОценок пока нет
- A Randomized Controlled Study of Segment PDFДокумент7 страницA Randomized Controlled Study of Segment PDFFauzan IndraОценок пока нет
- ArchRheumatol 33 418Документ6 страницArchRheumatol 33 418qwerty hrОценок пока нет
- Functional Strength Training Versus Movement Performance Therapy For Upper Limb Motor Recovery Early After Stroke: A RCTДокумент8 страницFunctional Strength Training Versus Movement Performance Therapy For Upper Limb Motor Recovery Early After Stroke: A RCTانجمن بدنسازی ایرانОценок пока нет
- HTTPS:WWW Ncbi NLM Nih gov:pmc:articles:PMC9144471:pdf:jpm-12-00808Документ12 страницHTTPS:WWW Ncbi NLM Nih gov:pmc:articles:PMC9144471:pdf:jpm-12-00808Ihsanul Ma'arifОценок пока нет
- Neurom Tec at The Neur Inter - 2017 - Linderoth - Conventional and Novel Spinal Stimulation Algorithms HypotheticalДокумент9 страницNeurom Tec at The Neur Inter - 2017 - Linderoth - Conventional and Novel Spinal Stimulation Algorithms Hypotheticalsannorberto8Оценок пока нет
- Acupuntrure MasachusetsДокумент7 страницAcupuntrure Masachusetsjavimirf_966919057Оценок пока нет
- Peripheralneuromodulation Fortreatmentofchronic MigraineheadacheДокумент4 страницыPeripheralneuromodulation Fortreatmentofchronic MigraineheadacheCorin Boice TelloОценок пока нет
- The Effectiveness of Non-Invasive Treatments For Active Myofascial Trigger Point Pain A Systematic Review of The Literature - Rickards2006Документ17 страницThe Effectiveness of Non-Invasive Treatments For Active Myofascial Trigger Point Pain A Systematic Review of The Literature - Rickards2006hjakamjОценок пока нет
- Efficassy and Safety of TDCSДокумент2 страницыEfficassy and Safety of TDCSlabsoneducationОценок пока нет
- Influence of The Generation of Motor Mental Images On Physiotherapy Treatment in Patients With Chronic Low Back PainДокумент25 страницInfluence of The Generation of Motor Mental Images On Physiotherapy Treatment in Patients With Chronic Low Back PainMÓNICA GRANDE ALONSOОценок пока нет
- Clinical Neurophysiology of Fatigue: M.J. Zwarts, G. Bleijenberg, B.G.M. Van EngelenДокумент9 страницClinical Neurophysiology of Fatigue: M.J. Zwarts, G. Bleijenberg, B.G.M. Van EngelenShyamali Kaushalya FernandoОценок пока нет
- Estimulação Cerebral Não Invasiva para o Tratamento Da Disartria Neurogênica - RevisãoДокумент10 страницEstimulação Cerebral Não Invasiva para o Tratamento Da Disartria Neurogênica - Revisãonathalia suellenОценок пока нет
- TENS Literature - Review - and - Meta - Analysis - Of.99266Документ9 страницTENS Literature - Review - and - Meta - Analysis - Of.99266Adam ForshawОценок пока нет
- Acupuncture For CTSДокумент7 страницAcupuncture For CTSspiderОценок пока нет
- Ef Ficacy of Transcutaneous Electrical Nerve Stimulation in People With Pain After Spinal Cord Injury: A Meta-AnalysisДокумент7 страницEf Ficacy of Transcutaneous Electrical Nerve Stimulation in People With Pain After Spinal Cord Injury: A Meta-Analysisxian karachiОценок пока нет
- Assembling Acupuncture Points To Impart A Meaningful Neuromodulatory InputДокумент2 страницыAssembling Acupuncture Points To Impart A Meaningful Neuromodulatory InputTrung Hiệp ĐàoОценок пока нет
- Toxina BotulinicaДокумент6 страницToxina BotulinicaBerbece SorinОценок пока нет
- Programme 1615Документ29 страницProgramme 1615Matias RizzoneОценок пока нет
- NIH Public Access: Author ManuscriptДокумент12 страницNIH Public Access: Author ManuscriptcasОценок пока нет
- Research Article: Neuroprotective Effects of Cistanches Herba Therapy On Patients With Moderate Alzheimer's DiseaseДокумент13 страницResearch Article: Neuroprotective Effects of Cistanches Herba Therapy On Patients With Moderate Alzheimer's DiseaseVeronica Yosita AnandaОценок пока нет
- Heterogeneous Cortical Effects of Spinal Cord StimДокумент11 страницHeterogeneous Cortical Effects of Spinal Cord StimOscarGallardoОценок пока нет
- A Double Blind Placebo RCT To Investigate The Effects of Serotonergic Modulation On Brain Excitability and Motor Recovery in Stroke PatientsДокумент7 страницA Double Blind Placebo RCT To Investigate The Effects of Serotonergic Modulation On Brain Excitability and Motor Recovery in Stroke PatientsJuan Jose Anaya UribeОценок пока нет
- Hypothalamus and Amygdala Response To Acupuncture StimuliДокумент13 страницHypothalamus and Amygdala Response To Acupuncture StimuliAnibal CisternasОценок пока нет
- Asj 2020 0146Документ6 страницAsj 2020 0146Mandeep JangraОценок пока нет
- Seizures and Cognitive Outcome After Traumatic Brain Injury: A Post Hoc AnalysisДокумент9 страницSeizures and Cognitive Outcome After Traumatic Brain Injury: A Post Hoc AnalysisAlexisBallénОценок пока нет
- PDF 68919 81419Документ12 страницPDF 68919 81419daisyscdomingosОценок пока нет
- Cerebal PalsyДокумент10 страницCerebal PalsySoffie FitriyahОценок пока нет
- 2014 24 H Mov SacadicosДокумент11 страниц2014 24 H Mov SacadicosIda Ho Rosell RodríguezОценок пока нет
- Upper Airway Stimulation For Obstructive Sleep Apnea: Durability of The Treatment Effect at 18 MonthsДокумент9 страницUpper Airway Stimulation For Obstructive Sleep Apnea: Durability of The Treatment Effect at 18 MonthsHamzeh AlsalhiОценок пока нет
- Scmittt MC Cord Indicator TestingДокумент4 страницыScmittt MC Cord Indicator TestingmitroisergiuОценок пока нет
- Innervation: The of The Joints of TheДокумент8 страницInnervation: The of The Joints of ThemitroisergiuОценок пока нет
- Zweifach 1959Документ8 страницZweifach 1959mitroisergiuОценок пока нет
- Leong 2011Документ6 страницLeong 2011mitroisergiuОценок пока нет
- Gardner 1948Документ14 страницGardner 1948mitroisergiuОценок пока нет
- Innervation of The Acromioclavicular Joint by The Suprascapular NerveДокумент6 страницInnervation of The Acromioclavicular Joint by The Suprascapular NervemitroisergiuОценок пока нет
- Dennis R. Carter, Gary S. Beaupré - Skeletal Function and Form - Mechanobiology of Skeletal Development, Aging, and Regeneration (2007)Документ331 страницаDennis R. Carter, Gary S. Beaupré - Skeletal Function and Form - Mechanobiology of Skeletal Development, Aging, and Regeneration (2007)mitroisergiuОценок пока нет
- Of Of: The Innervation The Joints The Wrist and HandДокумент6 страницOf Of: The Innervation The Joints The Wrist and HandmitroisergiuОценок пока нет
- Innervation The Human Shoulder Joint and Its Implications For SurgeryДокумент6 страницInnervation The Human Shoulder Joint and Its Implications For SurgerymitroisergiuОценок пока нет
- Gardner 1948Документ19 страницGardner 1948mitroisergiuОценок пока нет
- Gardner 1948Документ22 страницыGardner 1948mitroisergiuОценок пока нет
- Innervation O F Joint) : For The Hip, Knee and Elbow, and There Have BeenДокумент18 страницInnervation O F Joint) : For The Hip, Knee and Elbow, and There Have BeenmitroisergiuОценок пока нет
- Gardner 1948Документ14 страницGardner 1948mitroisergiuОценок пока нет
- Innervation: The of The Joints of TheДокумент8 страницInnervation: The of The Joints of ThemitroisergiuОценок пока нет
- Gardner 1948Документ22 страницыGardner 1948mitroisergiuОценок пока нет
- Innervation The Human Shoulder Joint and Its Implications For SurgeryДокумент6 страницInnervation The Human Shoulder Joint and Its Implications For SurgerymitroisergiuОценок пока нет
- Of Of: The Innervation The Joints The Wrist and HandДокумент6 страницOf Of: The Innervation The Joints The Wrist and HandmitroisergiuОценок пока нет
- Innervation of The Acromioclavicular Joint by The Suprascapular NerveДокумент6 страницInnervation of The Acromioclavicular Joint by The Suprascapular NervemitroisergiuОценок пока нет
- Innervation O F Joint) : For The Hip, Knee and Elbow, and There Have BeenДокумент18 страницInnervation O F Joint) : For The Hip, Knee and Elbow, and There Have BeenmitroisergiuОценок пока нет
- Laumonerie 2020Документ27 страницLaumonerie 2020mitroisergiuОценок пока нет
- Gardner 1948Документ14 страницGardner 1948mitroisergiuОценок пока нет
- Gardner 1948Документ19 страницGardner 1948mitroisergiuОценок пока нет
- Innervation: The of The Joints of TheДокумент8 страницInnervation: The of The Joints of ThemitroisergiuОценок пока нет
- Innervation O F Joint) : For The Hip, Knee and Elbow, and There Have BeenДокумент18 страницInnervation O F Joint) : For The Hip, Knee and Elbow, and There Have BeenmitroisergiuОценок пока нет
- Laumonerie 2020Документ27 страницLaumonerie 2020mitroisergiuОценок пока нет
- Innervation of The Acromioclavicular Joint by The Suprascapular NerveДокумент6 страницInnervation of The Acromioclavicular Joint by The Suprascapular NervemitroisergiuОценок пока нет
- Gardner 1948Документ22 страницыGardner 1948mitroisergiuОценок пока нет
- Of Of: The Innervation The Joints The Wrist and HandДокумент6 страницOf Of: The Innervation The Joints The Wrist and HandmitroisergiuОценок пока нет
- Innervation The Human Shoulder Joint and Its Implications For SurgeryДокумент6 страницInnervation The Human Shoulder Joint and Its Implications For SurgerymitroisergiuОценок пока нет
- Gardner 1948Документ19 страницGardner 1948mitroisergiuОценок пока нет
- Chronic Complications of Spinal Cord Injury and Disease - UpToDateДокумент25 страницChronic Complications of Spinal Cord Injury and Disease - UpToDateElinaldo Soares Costa SilvaОценок пока нет
- Sample Test Questions V 3Документ43 страницыSample Test Questions V 3Jignasha VadiОценок пока нет
- Impaired Physical Mobility NCPДокумент3 страницыImpaired Physical Mobility NCPYan ReyesОценок пока нет
- 2001 Yorkston KM - Evidence-Based Practice Guidelines For Dysarthria Management of Velopharyngeal FunctionДокумент18 страниц2001 Yorkston KM - Evidence-Based Practice Guidelines For Dysarthria Management of Velopharyngeal FunctionPaulo César Ferrada VenegasОценок пока нет
- The Detailed Neurological Examination in Adults PDFДокумент30 страницThe Detailed Neurological Examination in Adults PDFOkenabirhieОценок пока нет
- Chronic Neuromusculoskeletal DisordersДокумент28 страницChronic Neuromusculoskeletal DisordersMegan KelleyОценок пока нет
- Physical Therapy Clinical Management.9 PDFДокумент24 страницыPhysical Therapy Clinical Management.9 PDFClaudia MicuОценок пока нет
- Skeletal Muscle Relaxants and AssociatedДокумент10 страницSkeletal Muscle Relaxants and AssociatedMiguelОценок пока нет
- AssessmentДокумент2 страницыAssessmentKit Julls GutierrezОценок пока нет
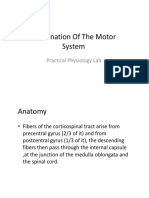
- Examination of The Motor System: Practical Physiology LabДокумент20 страницExamination of The Motor System: Practical Physiology Labحسين سعد حاتم خضيرОценок пока нет
- Cerebral Palsy Presentation 1Документ12 страницCerebral Palsy Presentation 1api-438626249Оценок пока нет
- Cerebral Palsy An Overview 2018Документ11 страницCerebral Palsy An Overview 2018Yhuliana AcostaОценок пока нет
- Spasticity: Pathophysiology, Evaluation and ManagementДокумент10 страницSpasticity: Pathophysiology, Evaluation and ManagementNacho MicheloniОценок пока нет
- Journal TetanusДокумент10 страницJournal TetanusWinariieeyy NayyОценок пока нет
- Orthotic Management of Children With Cerebral PalsyДокумент9 страницOrthotic Management of Children With Cerebral PalsyEslam ElsayedОценок пока нет
- People Vs VillacortaДокумент11 страницPeople Vs VillacortaFelix Gabriel BalaniОценок пока нет
- Reflex TestingДокумент44 страницыReflex Testingsarguss14100% (7)
- Cerebral Palsy - Definition, Causes and ClassificationДокумент40 страницCerebral Palsy - Definition, Causes and Classificationrenuka aurangabadkerОценок пока нет
- Sullivan Et Al 2007 STEPS-CR 5Документ23 страницыSullivan Et Al 2007 STEPS-CR 5Karen PohlОценок пока нет
- Pediatric Nursing-Course AuditДокумент305 страницPediatric Nursing-Course AuditMarites Santos Aquino100% (1)
- PathoPHYSIOLOGY OF Spasticity PDFДокумент9 страницPathoPHYSIOLOGY OF Spasticity PDFmandeep axonОценок пока нет
- The Sinew (Tendino-Muscular) Meridians - Jade Institute ClassesДокумент10 страницThe Sinew (Tendino-Muscular) Meridians - Jade Institute ClassespanisajОценок пока нет
- 2005 Self-Assessment Examination For Residents (Sae-R) : Abridged VersionДокумент22 страницы2005 Self-Assessment Examination For Residents (Sae-R) : Abridged VersionSoumabho DasОценок пока нет
- Management of Gross Motor (PT)Документ63 страницыManagement of Gross Motor (PT)Xulkanain ZEОценок пока нет
- Speech Characteristics of Different Types of Dysarthria: by Dr. Somesh Maheshwari, IndoreДокумент21 страницаSpeech Characteristics of Different Types of Dysarthria: by Dr. Somesh Maheshwari, IndoreDr. Somesh MaheshwariОценок пока нет
- Cerebral PalsyДокумент6 страницCerebral PalsyDarayaniDinaОценок пока нет
- Cerebral Palsy: I. Definition/ DescriptionДокумент5 страницCerebral Palsy: I. Definition/ Descriptionfaye kimОценок пока нет
- MNDДокумент28 страницMNDGayle VillarizaОценок пока нет
- Cerebral Palsy Physiotherapy TreatmentДокумент17 страницCerebral Palsy Physiotherapy Treatmentj_______________jОценок пока нет
- Sample Initial Evaluation PhysiotherapyДокумент10 страницSample Initial Evaluation PhysiotherapyWenzy CruzОценок пока нет