Вам также может понравиться
- Timebomb:The Global Epidemic of Multi-Drug Resistant TuberculosisОт EverandTimebomb:The Global Epidemic of Multi-Drug Resistant TuberculosisРейтинг: 3.5 из 5 звезд3.5/5 (2)
- ThoracostomyДокумент10 страницThoracostomywabalyОценок пока нет
- Radiopatologi Traktus RespiratoriusДокумент57 страницRadiopatologi Traktus RespiratoriusAris MahfuzhiОценок пока нет
- RozerplastyДокумент4 страницыRozerplastyLutfi Aulia RahmanОценок пока нет
- Hirschsprung DiseaseДокумент20 страницHirschsprung DiseaseIyan AsianaОценок пока нет
- Elbow - Fractures in Children: Fracture MechanismДокумент31 страницаElbow - Fractures in Children: Fracture MechanismhendoramuОценок пока нет
- Tindakan TorakosentesisДокумент15 страницTindakan TorakosentesisAyu Ayu AyuОценок пока нет
- DyspepsiaДокумент7 страницDyspepsiaFa'iz HeryotoОценок пока нет
- Abdomen GIT Radiology 1Документ57 страницAbdomen GIT Radiology 1malekОценок пока нет
- Referat - Spondilitis TB (RSAL)Документ35 страницReferat - Spondilitis TB (RSAL)Angga Yogi LaksmanaОценок пока нет
- Interpretasi Thorax FotoДокумент38 страницInterpretasi Thorax FotoSinta SintaaОценок пока нет
- Blunt Adominal TraumaДокумент13 страницBlunt Adominal TraumaIlham RamadhanОценок пока нет
- DR - Dr. Tahan P.H.,: FK UWK Surabaya Januari 2014Документ30 страницDR - Dr. Tahan P.H.,: FK UWK Surabaya Januari 2014Chen SiongОценок пока нет
- Diabetes Melitus: Makbul M AmanДокумент69 страницDiabetes Melitus: Makbul M AmanDwi YantiОценок пока нет
- Gambaran CT Scan NormalДокумент16 страницGambaran CT Scan NormalYudi SfОценок пока нет
- TPE in Intensive Care - Dr. Teuku Yasir, SpAn-KIC, FIPMДокумент17 страницTPE in Intensive Care - Dr. Teuku Yasir, SpAn-KIC, FIPMTeuku FauzanoeОценок пока нет
- Comparison of General and Regional Anesthesia in Morbidly Obese Patient Case Report Ijdmd 18Документ4 страницыComparison of General and Regional Anesthesia in Morbidly Obese Patient Case Report Ijdmd 18Djustiela KarrangОценок пока нет
- Volvulus MedscapeДокумент7 страницVolvulus MedscapeHanny Novia RiniОценок пока нет
- Bimbingan ThoraksДокумент71 страницаBimbingan ThoraksHedya Nadhrati SururaОценок пока нет
- Radlink PET and Cardiac Imaging Centre - PhilipsДокумент1 страницаRadlink PET and Cardiac Imaging Centre - PhilipsRadlinkSingaporeОценок пока нет
- Oeis SyndromeДокумент9 страницOeis SyndromeADEEОценок пока нет
- Midgut Volvulus 2018Документ2 страницыMidgut Volvulus 2018zzzОценок пока нет
- WSDДокумент12 страницWSDIvana SupitОценок пока нет
- Death Case Dr. MeikoДокумент49 страницDeath Case Dr. MeikoMohamad ZulfikarОценок пока нет
- RIZ - Enterocutaneous FistulaДокумент35 страницRIZ - Enterocutaneous FistulaAdiwirya AristiaraОценок пока нет
- Worksheet PrognosisДокумент3 страницыWorksheet PrognosisAmieyAtlantaMayОценок пока нет
- CA MammaeДокумент30 страницCA MammaeAlfiany SahrОценок пока нет
- Jurnal MRCPДокумент18 страницJurnal MRCPMaharani Eka SaputriОценок пока нет
- Shock Management, by Ayman RawehДокумент15 страницShock Management, by Ayman RawehaymxОценок пока нет
- Pengantar RadiologiДокумент40 страницPengantar Radiologishrt gtОценок пока нет
- Radiographic Positioning and Related Anatomy by Isadore MeschanДокумент3 страницыRadiographic Positioning and Related Anatomy by Isadore MeschanChe Castro0% (1)
- DAFTAR PUSTAKA RadiologiДокумент1 страницаDAFTAR PUSTAKA RadiologiSantrii AdztiiОценок пока нет
- InsulinomaДокумент16 страницInsulinomaDerly Barino HasdiОценок пока нет
- Systemic Therapies of CRC: Johan KurniandaДокумент56 страницSystemic Therapies of CRC: Johan KurniandaANISA RACHMITA ARIANTI 2020Оценок пока нет
- GossipybomaДокумент8 страницGossipybomaDADDYTOОценок пока нет
- EGDT SepsisДокумент8 страницEGDT Sepsissiti fatmalaОценок пока нет
- CCDuodenum Periampullary Neoplasms ChuДокумент68 страницCCDuodenum Periampullary Neoplasms ChuSahirОценок пока нет
- Teknik Foto X Ray EkstremitasДокумент14 страницTeknik Foto X Ray EkstremitasEdiPtkОценок пока нет
- Differential Diagnosis of Microcytic Anemia PDFДокумент5 страницDifferential Diagnosis of Microcytic Anemia PDFayms99Оценок пока нет
- White Island in The Red SeaДокумент1 страницаWhite Island in The Red SeaIndach RatnaОценок пока нет
- PPTДокумент27 страницPPTmonicanasutionОценок пока нет
- Kuliah Radiologi Emergensi - Maret 2020 - PlainДокумент67 страницKuliah Radiologi Emergensi - Maret 2020 - PlainArief VerditoОценок пока нет
- Fraktur Humerus Sepertiga DistalДокумент26 страницFraktur Humerus Sepertiga DistalNurul Rezki Fitriani AzisОценок пока нет
- Pelvic Organ Prolapse: PathophysiologyДокумент4 страницыPelvic Organ Prolapse: PathophysiologyGrimaldi IhsanОценок пока нет
- Chord So Far AwayДокумент2 страницыChord So Far AwaymarasutansirОценок пока нет
- Batu Saluran Kemih: Dr. Suhaemi, SPPD, FinasimДокумент57 страницBatu Saluran Kemih: Dr. Suhaemi, SPPD, FinasimAfri AdiОценок пока нет
- Diabetic FootДокумент73 страницыDiabetic Footmohammad.irfanОценок пока нет
- CASP Checklist: Case Control Study How To Use This Appraisal ToolДокумент6 страницCASP Checklist: Case Control Study How To Use This Appraisal Toolanon_770867052Оценок пока нет
- TN73-2 Electromagnetic Disturbance Troubleshooting HelpДокумент6 страницTN73-2 Electromagnetic Disturbance Troubleshooting HelpCharls GuevaraОценок пока нет
- Difficult AirwayДокумент38 страницDifficult AirwaybrojeemОценок пока нет
- Empiema Kandung EmpeduДокумент7 страницEmpiema Kandung EmpeduHasya KinasihОценок пока нет
- ICU Management of Acute PancreatitisДокумент77 страницICU Management of Acute PancreatitisAndriy SubieОценок пока нет
- Bipolar TurpДокумент22 страницыBipolar Turpjmohideenkadhar100% (1)
- Acute AbdomenДокумент117 страницAcute Abdomenayundaafdal100% (1)
- LONG CASE Luka BakarДокумент16 страницLONG CASE Luka BakarAfiazka LuthfitaОценок пока нет
- Lampiran Pengumuman Nominas Tahap 1 Sipenmaru Jalur PMDP 2020 PDFДокумент66 страницLampiran Pengumuman Nominas Tahap 1 Sipenmaru Jalur PMDP 2020 PDFRizki Abdul MalikОценок пока нет
- Antibiotic Therapy For Peritonitis: Treatment Overview, Spontaneous Bacterial Peritonitis, Secondary and Tertiary PeritonitisДокумент7 страницAntibiotic Therapy For Peritonitis: Treatment Overview, Spontaneous Bacterial Peritonitis, Secondary and Tertiary PeritonitisTias SubagioОценок пока нет
- n378.008 Iris Website Staging of CKD PDFДокумент8 страницn378.008 Iris Website Staging of CKD PDFrutebeufОценок пока нет
- Total Mesorectal Excision (Tme)Документ19 страницTotal Mesorectal Excision (Tme)Mehtab JameelОценок пока нет
- Supplementary Table 1a. All Study Data For Bladder Cancer IncidenceДокумент19 страницSupplementary Table 1a. All Study Data For Bladder Cancer IncidenceSteven SetioОценок пока нет
- ESC Guidelines For DX and TX of Acute and Chronic HF (2016)Документ85 страницESC Guidelines For DX and TX of Acute and Chronic HF (2016)Imja94Оценок пока нет
- The Association Between Smoking Quantity and Lung Cancer in Men and WomenДокумент7 страницThe Association Between Smoking Quantity and Lung Cancer in Men and WomenSteven SetioОценок пока нет
- Perforated Jejunal Diverticular Disease: A Diagnostic Pitfall at Frozen Section of A Mesenteric Mass For Adenocarcinoma of The StomachДокумент3 страницыPerforated Jejunal Diverticular Disease: A Diagnostic Pitfall at Frozen Section of A Mesenteric Mass For Adenocarcinoma of The StomachSteven SetioОценок пока нет
- Guidlines Pregnancy and Heart DiseaseДокумент52 страницыGuidlines Pregnancy and Heart DiseasePanggih Sekar Palupi IIОценок пока нет
- RCOG Cardiac Disease and Pregnancy PDFДокумент18 страницRCOG Cardiac Disease and Pregnancy PDFSteven SetioОценок пока нет
- RCOG Cardiac Disease and Pregnancy PDFДокумент18 страницRCOG Cardiac Disease and Pregnancy PDFSteven SetioОценок пока нет
- 2012 FallwinterДокумент8 страниц2012 FallwinterSteven SetioОценок пока нет
- Sle 07 PDFДокумент6 страницSle 07 PDFSteven SetioОценок пока нет
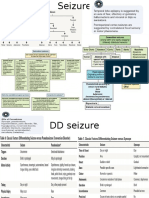
- SeizureДокумент6 страницSeizureSteven SetioОценок пока нет
- GINA 2016 Main Pocket GuideДокумент29 страницGINA 2016 Main Pocket GuideKaren Ceballos LopezОценок пока нет
- Status Asmatikus 1Документ8 страницStatus Asmatikus 1Steven SetioОценок пока нет
- DR - Jane Gillett-Whats The Difference Between A Subdural and Epidural HematomaДокумент2 страницыDR - Jane Gillett-Whats The Difference Between A Subdural and Epidural HematomaproluvieslacusОценок пока нет
- Nefrolitiasis 02Документ8 страницNefrolitiasis 02Steven SetioОценок пока нет
- Frequency Table UnivariatДокумент2 страницыFrequency Table UnivariatSteven SetioОценок пока нет
- 3 s2.0 B9781437722062001391Документ23 страницы3 s2.0 B9781437722062001391Steven SetioОценок пока нет
- Adrenal CrisisДокумент6 страницAdrenal CrisisSteven SetioОценок пока нет
- Sle 05 PDFДокумент6 страницSle 05 PDFSteven SetioОценок пока нет
- International Journal of Gynecology and ObstetricsДокумент4 страницыInternational Journal of Gynecology and ObstetricsSteven SetioОценок пока нет
- Fleis PDFДокумент1 страницаFleis PDFSteven SetioОценок пока нет
- Tugas KKDДокумент4 страницыTugas KKDSteven SetioОценок пока нет
- 1 s2.0 S0735675713004890Документ3 страницы1 s2.0 S0735675713004890Steven SetioОценок пока нет
- 2021 A Guide To The African Human Rights System Celebrating 40 YearsДокумент115 страниц2021 A Guide To The African Human Rights System Celebrating 40 YearsChala Yuye KemerОценок пока нет
- S.N o Name of Drug Recommended Paediatrics Dose Strength 1.: CPM - 2 mg/5mlДокумент3 страницыS.N o Name of Drug Recommended Paediatrics Dose Strength 1.: CPM - 2 mg/5mlmrs raamОценок пока нет
- Coca Cola The Water Stewardship and Replanish Report1 2012Документ80 страницCoca Cola The Water Stewardship and Replanish Report1 2012CSRmedia.ro NetworkОценок пока нет
- Reflective Journal 1 2 and 3Документ11 страницReflective Journal 1 2 and 3api-321980896Оценок пока нет
- Job Contract Agreement Letter PDFДокумент4 страницыJob Contract Agreement Letter PDFQazi Yusuf100% (1)
- Reflection PaperДокумент27 страницReflection PaperBon Ryan LeonardoОценок пока нет
- Tinnitus Today September 1986 Vol 11, No 3Документ8 страницTinnitus Today September 1986 Vol 11, No 3American Tinnitus AssociationОценок пока нет
- HSE Assignment 3 FinalДокумент21 страницаHSE Assignment 3 FinalLuqman HakimОценок пока нет
- Clinical Gaze Through The Prism of LiteratureДокумент10 страницClinical Gaze Through The Prism of LiteratureZedarОценок пока нет
- Health Tourism Presentation IBMДокумент65 страницHealth Tourism Presentation IBMMd. Ashraf Hossain SarkerОценок пока нет
- ResearchДокумент3 страницыResearchMervin AlbercaОценок пока нет
- Minimum and Peak Flows of WastewaterДокумент26 страницMinimum and Peak Flows of WastewaterSteven Joseph IncioОценок пока нет
- Travel Nurse Pdf1Документ2 страницыTravel Nurse Pdf1Med NetОценок пока нет
- TDR Business Plan 2008-2013: Robert RidleyДокумент43 страницыTDR Business Plan 2008-2013: Robert RidleySripal JainОценок пока нет
- Gold Medalist ClubДокумент18 страницGold Medalist ClubSmit patelОценок пока нет
- One-Compartment Open Model: Intravenous Bolus AdministrationДокумент8 страницOne-Compartment Open Model: Intravenous Bolus AdministrationnursalОценок пока нет
- Inventory Management NestleДокумент40 страницInventory Management Nestlesrinivas2help883675% (4)
- CPRДокумент45 страницCPRJames Elwood DoyolaОценок пока нет
- Common Childhood Rashes: Has The Rash Got Fluid-Filled (Vesiculobullous) Lesions?Документ4 страницыCommon Childhood Rashes: Has The Rash Got Fluid-Filled (Vesiculobullous) Lesions?abu ubaidahОценок пока нет
- Manual PTCДокумент64 страницыManual PTCSeba SapiainОценок пока нет
- Interstitial Cystitis (Painful Bladder Syndrome) - Causes & TreatmentДокумент12 страницInterstitial Cystitis (Painful Bladder Syndrome) - Causes & TreatmentJimmy GillОценок пока нет
- One Compartment Open ModelДокумент81 страницаOne Compartment Open Modelanon_937994778Оценок пока нет
- Progressive Addition Lens Design and The Short of Stature (Shan-Yu, S.)Документ3 страницыProgressive Addition Lens Design and The Short of Stature (Shan-Yu, S.)Valentina PereaОценок пока нет
- P CLS14 Powertec Compact Leg Sled ManualДокумент15 страницP CLS14 Powertec Compact Leg Sled ManualElizabeth GuzmanОценок пока нет
- Combine PDFДокумент164 страницыCombine PDFmichael.quintanaОценок пока нет
- Schoolgirl: María de Los Ángeles Lizeth Solís Jiménez Teacher: Kenneth Matter: English VДокумент16 страницSchoolgirl: María de Los Ángeles Lizeth Solís Jiménez Teacher: Kenneth Matter: English VAngeles Solis JimenezОценок пока нет
- 2017 ESC Guidelines For The Management of Acute Myocardial Infarction in Patients Presenting With ST Segment ElevationДокумент66 страниц2017 ESC Guidelines For The Management of Acute Myocardial Infarction in Patients Presenting With ST Segment ElevationMoises Torres AlvarezОценок пока нет
- Hun Yuan Qigong - All NotesДокумент19 страницHun Yuan Qigong - All Notespilillo50% (2)
- MSDS-Muriate of Potash 2017Документ11 страницMSDS-Muriate of Potash 2017Inoe69Оценок пока нет
- Pandakaking-Puti: KampupotДокумент10 страницPandakaking-Puti: KampupotgosmileyОценок пока нет