Вам также может понравиться
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Bellini - Oboe Concerto Big Orchestra - Oboe SoloДокумент3 страницыBellini - Oboe Concerto Big Orchestra - Oboe SoloAlberto SignorileОценок пока нет
- Bellini - Oboe Concerto Big Orchestra - Oboe SoloДокумент3 страницыBellini - Oboe Concerto Big Orchestra - Oboe SoloAlberto SignorileОценок пока нет
- Cardiovascular Notes ATFДокумент256 страницCardiovascular Notes ATFenriОценок пока нет
- Cardio Pulmo NotesДокумент12 страницCardio Pulmo NotesCherrie MaeОценок пока нет
- U World Cardiac FinalДокумент15 страницU World Cardiac FinalAcohCChaoОценок пока нет
- Hematology SBAДокумент17 страницHematology SBAJared Khoo Er Hau100% (1)
- Cardiac Surgeries: and ManagementДокумент64 страницыCardiac Surgeries: and ManagementSimon Josan0% (1)
- Robert A. Freitas Nano Medicine, Vol. IIA Biocompatibility-Landes Bioscience (2003)Документ357 страницRobert A. Freitas Nano Medicine, Vol. IIA Biocompatibility-Landes Bioscience (2003)maimai_bnОценок пока нет
- (Family Medicine) Mimi Zeiger - Essentials of Writing Biomedical Research Papers-McGraw-Hill (1999) PDFДокумент473 страницы(Family Medicine) Mimi Zeiger - Essentials of Writing Biomedical Research Papers-McGraw-Hill (1999) PDFAaron MokОценок пока нет
- F Theta 017700 003 26 FT 03 90FT 125Документ1 страницаF Theta 017700 003 26 FT 03 90FT 125Aaron MokОценок пока нет
- 1550nm CCDДокумент20 страниц1550nm CCDAaron MokОценок пока нет
- 2014 Student MapДокумент1 страница2014 Student MapDan latherОценок пока нет
- 6215 H Data SheetДокумент1 страница6215 H Data SheetAaron MokОценок пока нет
- Syllabus AEP4400 Sp18Документ2 страницыSyllabus AEP4400 Sp18Aaron MokОценок пока нет
- Watson Et Al 1987 CytometryДокумент8 страницWatson Et Al 1987 CytometryAaron MokОценок пока нет
- MAGOOSH Guide To The TOEFL-iBT PDFДокумент157 страницMAGOOSH Guide To The TOEFL-iBT PDFPolivio J. RosarioОценок пока нет
- Presentation On MaybellineДокумент10 страницPresentation On MaybellineAaron Mok0% (1)
- 2013 AnnualReportДокумент92 страницы2013 AnnualReportHarish RamasubramanianОценок пока нет
- SM1000 Datasheet PDFДокумент3 страницыSM1000 Datasheet PDFAaron MokОценок пока нет
- Hongkong Notes A AsdfasdfsdafsadfДокумент6 страницHongkong Notes A AsdfasdfsdafsadfAaron MokОценок пока нет
- Flowchart For PeДокумент1 страницаFlowchart For PeJuan Dela CruzОценок пока нет
- Optogenetics FutureДокумент2 страницыOptogenetics FutureAaron MokОценок пока нет
- New Trend Maths ChapterДокумент32 страницыNew Trend Maths ChapterAaron MokОценок пока нет
- Pulse Oximeter Implementation Freescale..Документ39 страницPulse Oximeter Implementation Freescale..yrikkiОценок пока нет
- Flowchart For PeДокумент1 страницаFlowchart For PeJuan Dela CruzОценок пока нет
- Anoobisvol 4pmpmybuildpaladinguideДокумент12 страницAnoobisvol 4pmpmybuildpaladinguideAaron MokОценок пока нет
- ReadmeДокумент1 страницаReadmejacksonrandyjjОценок пока нет
- IKEA Marketing Plan - Part I: John DalyДокумент29 страницIKEA Marketing Plan - Part I: John DalyAaron MokОценок пока нет
- 4 Ae 5 C 07 Be 030 DДокумент16 страниц4 Ae 5 C 07 Be 030 DAaron MokОценок пока нет
- Valvular Heart Disease: Mitral RegurgitationДокумент33 страницыValvular Heart Disease: Mitral RegurgitationjihyooniОценок пока нет
- Advocacy ProjectДокумент18 страницAdvocacy Projectapi-236375124Оценок пока нет
- All Four Heart Valves Lie Along The Same PlaneДокумент2 страницыAll Four Heart Valves Lie Along The Same PlaneSulochana ChanОценок пока нет
- Supraventricular TachycardiaДокумент20 страницSupraventricular TachycardiaBenyWirananggalaОценок пока нет
- The Newborn Care: Fcnlxa - St. Luke's College of NursingДокумент11 страницThe Newborn Care: Fcnlxa - St. Luke's College of NursingFrancine LaxaОценок пока нет
- Echo Protocol GuideДокумент29 страницEcho Protocol Guideapi-722001988Оценок пока нет
- Complication of MI (Myocardial Infarction)Документ2 страницыComplication of MI (Myocardial Infarction)Zahid QamarОценок пока нет
- Olahraga Sebagai Pencegahan Penyakit Jantung KoronerДокумент6 страницOlahraga Sebagai Pencegahan Penyakit Jantung KoronerGrace YutoОценок пока нет
- The Language of Medicine: Cardiovascular SystemДокумент33 страницыThe Language of Medicine: Cardiovascular SystemCPD MASОценок пока нет
- Syllabus of Paramedical Courses PDFДокумент355 страницSyllabus of Paramedical Courses PDFbonat07Оценок пока нет
- WSDДокумент13 страницWSDhinatakunhinata75Оценок пока нет
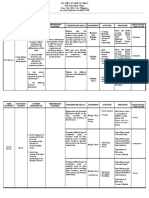
- CURRICULUM MAP (Grade 9)Документ2 страницыCURRICULUM MAP (Grade 9)Vijanes BeltransОценок пока нет
- IGCSE - CIE - Combined 2017 2018 SyllabusДокумент57 страницIGCSE - CIE - Combined 2017 2018 SyllabusYu SunОценок пока нет
- DC-N2 Datasheet - 160428Документ16 страницDC-N2 Datasheet - 160428Sayuri SuárezОценок пока нет
- Drill #1 With RationaleДокумент12 страницDrill #1 With RationaleRellie CastroОценок пока нет
- Euac 125Документ23 страницыEuac 125Nicoletta OrphanouОценок пока нет
- Ms Plastic SurgeryДокумент48 страницMs Plastic SurgeryAlfirmansyah AmruОценок пока нет
- How To Measure Ankle Brachial IndexДокумент4 страницыHow To Measure Ankle Brachial Indexzaky0% (1)
- Blood VesselsДокумент4 страницыBlood VesselsCrazy StrangerОценок пока нет
- BioK QQ 6.2 QPДокумент2 страницыBioK QQ 6.2 QPesteban1013264503Оценок пока нет
- Acyanotic Congenital Heart DiseaseДокумент23 страницыAcyanotic Congenital Heart DiseasePernel Jose Alam MicuboОценок пока нет
- SherpaSpecialityCurvesBrochure OriginalДокумент2 страницыSherpaSpecialityCurvesBrochure OriginalDigipact DigiОценок пока нет
- Right + Increased Vascularity + Fixed S2 / Widely Split Austin-Flint (Chronic) Graham Steele MurmurДокумент14 страницRight + Increased Vascularity + Fixed S2 / Widely Split Austin-Flint (Chronic) Graham Steele MurmurRojales FrancisОценок пока нет
- B.sc. NSG - Sylabus KUHASДокумент63 страницыB.sc. NSG - Sylabus KUHASrijumathewmscОценок пока нет