Вам также может понравиться
- Acidosis: Clinical Aspects and Treatment with Isotonic Sodium Bicarbonate SolutionОт EverandAcidosis: Clinical Aspects and Treatment with Isotonic Sodium Bicarbonate SolutionРейтинг: 5 из 5 звезд5/5 (1)
- Oxygen: High Enzymatic Reactivity of Reactive Oxygen SpeciesОт EverandOxygen: High Enzymatic Reactivity of Reactive Oxygen SpeciesОценок пока нет
- Thorn Eh and OutДокумент24 страницыThorn Eh and OutNick MaxОценок пока нет
- Pharmacotherapy of Bronchial AsthmaДокумент7 страницPharmacotherapy of Bronchial AsthmaAhmedshaker21100% (2)
- 14 NSAIDS LastДокумент46 страниц14 NSAIDS LastMewael TesfamichaelОценок пока нет
- StrokeДокумент102 страницыStrokea20-0353-958Оценок пока нет
- On The Origin of Free and Bound Staling Aldehydes in BeerДокумент24 страницыOn The Origin of Free and Bound Staling Aldehydes in BeerVal SelОценок пока нет
- Turpentine Oil Poisoning MedlinePlus Medical EncyclopediaДокумент4 страницыTurpentine Oil Poisoning MedlinePlus Medical Encyclopediapiemar10Оценок пока нет
- Alzheimer's Disease Causes, Effects, and TreatmentsДокумент21 страницаAlzheimer's Disease Causes, Effects, and TreatmentsJesshica Navarro AlejandrinoОценок пока нет
- A Proposal On Study On The Histamine Content of Dried Fish in Some Districts of NepalДокумент8 страницA Proposal On Study On The Histamine Content of Dried Fish in Some Districts of NepalPrashanta PokhrelОценок пока нет
- Fitness & Mental HealthДокумент568 страницFitness & Mental HealthAndrew Richard ThompsonОценок пока нет
- ARBs (Angiotensin II Receptor Blockers) NCLEXДокумент15 страницARBs (Angiotensin II Receptor Blockers) NCLEXSameerQadumi100% (1)
- HypertensionДокумент85 страницHypertensionmelkamu AssefaОценок пока нет
- Methotrexate: DR B Himasri Sravya Pgy1 ResidentДокумент24 страницыMethotrexate: DR B Himasri Sravya Pgy1 ResidentSravyavas BhamidipatiОценок пока нет
- 9149StatlerMentalStatus PDFДокумент5 страниц9149StatlerMentalStatus PDFArumDesiPratiwiОценок пока нет
- Reference Ranges For Blood TestsДокумент38 страницReference Ranges For Blood TestscatalinОценок пока нет
- Chemistry ProjectДокумент11 страницChemistry ProjectThomas NinanОценок пока нет
- Recipes (Pharmacology Prescriptions)Документ6 страницRecipes (Pharmacology Prescriptions)tianallyОценок пока нет
- Vitamin B GroupДокумент31 страницаVitamin B GroupDereen NajatОценок пока нет
- 2014antiepileptics 131129145211 Phpapp01 PDFДокумент50 страниц2014antiepileptics 131129145211 Phpapp01 PDFshravaniОценок пока нет
- Ethanol Poisoning: Ethanol Poisoning Is Caused by Drinking Too Much AlcoholДокумент11 страницEthanol Poisoning: Ethanol Poisoning Is Caused by Drinking Too Much Alcohol0921pyОценок пока нет
- Water Soluble Vitamins: Vitamin C, B1, B2 & B3 FunctionsДокумент56 страницWater Soluble Vitamins: Vitamin C, B1, B2 & B3 FunctionsAvicena RasyidОценок пока нет
- For Best Viewing:: Open in Slide Show Mode Click On IconДокумент32 страницыFor Best Viewing:: Open in Slide Show Mode Click On IconSutapa PawarОценок пока нет
- Inhaled InsulinДокумент17 страницInhaled InsulinH.k. VamshidharОценок пока нет
- Ethiopian National Drug FormularyДокумент572 страницыEthiopian National Drug FormularyportosinОценок пока нет
- Diabetes Mellitus in The US:: PrevalenceДокумент48 страницDiabetes Mellitus in The US:: PrevalenceokibreazyОценок пока нет
- AkiДокумент13 страницAkiharshe v100% (1)
- Fluids & Electrolytes Disorders: Ariano Marcos State UniversityДокумент13 страницFluids & Electrolytes Disorders: Ariano Marcos State UniversityClements galiza100% (1)
- Anti Depressant Drug LatestДокумент65 страницAnti Depressant Drug LatestAnonymous zOMkw9100% (1)
- Standardization of Alcohol Calculations in ResearchДокумент12 страницStandardization of Alcohol Calculations in ResearchSava Vijak100% (1)
- Adult Nasogastric Insertion and Removal ProcedureДокумент8 страницAdult Nasogastric Insertion and Removal ProcedureAna MarieОценок пока нет
- Degenerative Joint DiseaseДокумент35 страницDegenerative Joint DiseaseWendy EscalanteОценок пока нет
- Basics of EpilepsyДокумент15 страницBasics of EpilepsyDiana CОценок пока нет
- Approach To Comatose Child: DR G.VenkateshДокумент83 страницыApproach To Comatose Child: DR G.VenkateshG VenkateshОценок пока нет
- Pathology of Stroke: Dr. Isnaniah, Sp. SДокумент51 страницаPathology of Stroke: Dr. Isnaniah, Sp. SFiladelfia sariОценок пока нет
- Pratley New Treatments For Type 2 DiabetesДокумент85 страницPratley New Treatments For Type 2 DiabetesMia DangaОценок пока нет
- Antiepileptic Drugs and Parkinson's Disease PharmacologyДокумент50 страницAntiepileptic Drugs and Parkinson's Disease PharmacologymayraОценок пока нет
- LocalanestheticsДокумент51 страницаLocalanestheticskingkb4uОценок пока нет
- General Anesthetics AbeerДокумент45 страницGeneral Anesthetics AbeerYousef JafarОценок пока нет
- Anti Anemia DrugsДокумент36 страницAnti Anemia DrugsArabelle GOОценок пока нет
- Whats Wrong With Prescribing Hipnotics?Документ6 страницWhats Wrong With Prescribing Hipnotics?Alberto JaramilloОценок пока нет
- Practice Guidelines for Candidiasis TreatmentДокумент17 страницPractice Guidelines for Candidiasis TreatmentCristian HaesbaertОценок пока нет
- What Is The Oxygen CascadeДокумент27 страницWhat Is The Oxygen CascadeRandhir Singh90% (10)
- Types of Tablets and Their CharecteristicsДокумент49 страницTypes of Tablets and Their CharecteristicsRohit IrkalОценок пока нет
- Candida and Other Fungi: Dr. John BergmanДокумент60 страницCandida and Other Fungi: Dr. John Bergmanzeina32Оценок пока нет
- Hypertension Treatment Steps For HypertensionДокумент15 страницHypertension Treatment Steps For Hypertensionfreelancer08100% (1)
- Understanding Metabolism of CarbohydratesДокумент48 страницUnderstanding Metabolism of CarbohydratesAbdullah TheОценок пока нет
- Metabolic Acidosis FinalДокумент29 страницMetabolic Acidosis FinalTera SurbaktiОценок пока нет
- Fluoride Toxicity: Effects, Dosages, TreatmentsДокумент25 страницFluoride Toxicity: Effects, Dosages, TreatmentsNandita KshetrimayumОценок пока нет
- 1introДокумент158 страниц1introDea MaharanisОценок пока нет
- Causes of Stroke PDFДокумент16 страницCauses of Stroke PDFEmmanuel AguilarОценок пока нет
- 2-60-1 - Colon Cancer TreatmentДокумент1 страница2-60-1 - Colon Cancer Treatmentlyocco1Оценок пока нет
- CAL GluconateДокумент29 страницCAL Gluconatehumag143100% (1)
- Cholinergic Agonists/ Cholinomimetic Agents: Dr. Kyi Kyi Tha Basic Medical Sciences Kulliyyah of Pharmacy IiumДокумент21 страницаCholinergic Agonists/ Cholinomimetic Agents: Dr. Kyi Kyi Tha Basic Medical Sciences Kulliyyah of Pharmacy IiumZhuan AhmadОценок пока нет
- Personal Protective Grounding - Training PresentationДокумент31 страницаPersonal Protective Grounding - Training PresentationIrfan UllahОценок пока нет
- Metabolism and NutritionДокумент52 страницыMetabolism and NutritionAlex SaljayОценок пока нет
- J Food Sci Technol, 2014, 51, 2271-2288Документ18 страницJ Food Sci Technol, 2014, 51, 2271-2288SonaliОценок пока нет
- ClostridumДокумент30 страницClostridumFrancesca VargasОценок пока нет
- Gut Microbiota-Targeted Diets Modulate Human Immune StatusДокумент42 страницыGut Microbiota-Targeted Diets Modulate Human Immune StatussimasОценок пока нет
- An 385Документ8 страницAn 385Indah GitaswariОценок пока нет
- 10 1016@j Oraloncology 2020 104804Документ5 страниц10 1016@j Oraloncology 2020 104804Indah GitaswariОценок пока нет
- Positioning The Instillation of Contrast Cystography: Does It Provide Any Clinical Benefit?Документ17 страницPositioning The Instillation of Contrast Cystography: Does It Provide Any Clinical Benefit?Indah GitaswariОценок пока нет
- A Randomized Clinical Trial Evaluating Negative Pressure Therapy To Decrease Vascular Groin Incision ComplicationsДокумент9 страницA Randomized Clinical Trial Evaluating Negative Pressure Therapy To Decrease Vascular Groin Incision ComplicationsIndah GitaswariОценок пока нет
- Research Journal of Pharmaceutical, Biological and Chemical SciencesДокумент7 страницResearch Journal of Pharmaceutical, Biological and Chemical SciencesIndah GitaswariОценок пока нет
- Management of The Injured Hand - Basic PrinciplesДокумент6 страницManagement of The Injured Hand - Basic PrinciplesIndah GitaswariОценок пока нет
- Body Contouring Surgery Improves Weight Loss After Bariatric Surgery - A Systematic Review and Meta-AnalysisДокумент12 страницBody Contouring Surgery Improves Weight Loss After Bariatric Surgery - A Systematic Review and Meta-AnalysisIndah GitaswariОценок пока нет
- Review Article: Recent Advances of Hemorrhage Management in Severe TraumaДокумент6 страницReview Article: Recent Advances of Hemorrhage Management in Severe TraumaIndah GitaswariОценок пока нет
- Stress Distribution in Mandible and Temporomandibular Joint by Mandibular Distraction: A 3-Dimensional Finite-Element AnalysisДокумент10 страницStress Distribution in Mandible and Temporomandibular Joint by Mandibular Distraction: A 3-Dimensional Finite-Element AnalysisIndah GitaswariОценок пока нет
- Journal Pre-Proof: Acta BiomaterialiaДокумент45 страницJournal Pre-Proof: Acta BiomaterialiaIndah GitaswariОценок пока нет
- Acute Tendon Injuries: The HandДокумент9 страницAcute Tendon Injuries: The HandIndah GitaswariОценок пока нет
- Thorax NormalДокумент1 страницаThorax NormalIndah GitaswariОценок пока нет
- Traumatic Extensor Tendon Injuries To The Hand: Clinical Anatomy, Biomechanics, and Surgical Procedure ReviewДокумент11 страницTraumatic Extensor Tendon Injuries To The Hand: Clinical Anatomy, Biomechanics, and Surgical Procedure ReviewJosua LouisОценок пока нет
- Thorax NormalДокумент1 страницаThorax NormalIndah GitaswariОценок пока нет
- Accepted Manuscript: NeuroscienceДокумент40 страницAccepted Manuscript: NeuroscienceIndah GitaswariОценок пока нет
- 4 The Role of BDNFДокумент22 страницы4 The Role of BDNFFajrina AyuОценок пока нет
- Principles of Hand Fracture Management: The Open Orthopaedics Journal February 2012Документ12 страницPrinciples of Hand Fracture Management: The Open Orthopaedics Journal February 2012Indah GitaswariОценок пока нет
- The Role of Brain-Derived Neurotrophic Factor (BDNF) in Cognitive FunctionsДокумент8 страницThe Role of Brain-Derived Neurotrophic Factor (BDNF) in Cognitive FunctionsIndah GitaswariОценок пока нет
- Gordon 2016Документ16 страницGordon 2016Indah GitaswariОценок пока нет
- Balog 2019nihms-1056643Документ14 страницBalog 2019nihms-1056643Indah GitaswariОценок пока нет
- Acute Tendon Injuries: The HandДокумент9 страницAcute Tendon Injuries: The HandIndah GitaswariОценок пока нет
- Traumatic Extensor Tendon Injuries To The Hand: Clinical Anatomy, Biomechanics, and Surgical Procedure ReviewДокумент11 страницTraumatic Extensor Tendon Injuries To The Hand: Clinical Anatomy, Biomechanics, and Surgical Procedure ReviewJosua LouisОценок пока нет
- M Ccomb H. Primary Repair of The Bilateral Cleft Lip Nose: A 15-Year Review and A New Treatment Plan. Plast Reconstr Surg. 1990 86:882Документ1 страницаM Ccomb H. Primary Repair of The Bilateral Cleft Lip Nose: A 15-Year Review and A New Treatment Plan. Plast Reconstr Surg. 1990 86:882Indah GitaswariОценок пока нет
- Acute Tendon Injuries: The HandДокумент9 страницAcute Tendon Injuries: The HandIndah GitaswariОценок пока нет
- Gordon 2009 Neurosurgical Focus) The Role of Neurotrophic Factors in Nerve RegenerationДокумент16 страницGordon 2009 Neurosurgical Focus) The Role of Neurotrophic Factors in Nerve RegenerationIndah GitaswariОценок пока нет
- Atls IndonesiaДокумент4 страницыAtls Indonesiabambangferdi irwantoОценок пока нет
- Al Majed2000Документ10 страницAl Majed2000Indah GitaswariОценок пока нет
- Electrical Stimulation Enhances Sensory Recovery - A Randomized Controlled TrialДокумент39 страницElectrical Stimulation Enhances Sensory Recovery - A Randomized Controlled TrialIndah GitaswariОценок пока нет
- REFERENCESДокумент1 страницаREFERENCESIndah GitaswariОценок пока нет
- Dafpus PITДокумент1 страницаDafpus PITIndah GitaswariОценок пока нет
- (SIRI Assessor Training) AM Guide Book - v2Документ19 страниц(SIRI Assessor Training) AM Guide Book - v2hadeelОценок пока нет
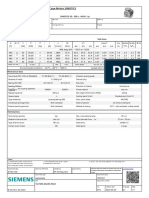
- 1LE1503-2AA43-4AA4 Datasheet enДокумент1 страница1LE1503-2AA43-4AA4 Datasheet enAndrei LupuОценок пока нет
- 3DS MAX SYLLABUSДокумент8 страниц3DS MAX SYLLABUSKannan RajaОценок пока нет
- Tata Chemicals Yearly Reports 2019 20Документ340 страницTata Chemicals Yearly Reports 2019 20AkchikaОценок пока нет
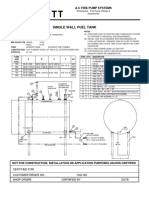
- Single Wall Fuel Tank: FP 2.7 A-C Fire Pump SystemsДокумент1 страницаSingle Wall Fuel Tank: FP 2.7 A-C Fire Pump Systemsricardo cardosoОценок пока нет
- Entrepreneurship WholeДокумент20 страницEntrepreneurship WholeKrizztian SiuaganОценок пока нет
- Ralf Behrens: About The ArtistДокумент3 страницыRalf Behrens: About The ArtistStavros DemosthenousОценок пока нет
- Software EngineeringДокумент3 страницыSoftware EngineeringImtiyaz BashaОценок пока нет
- Fabric Bursting StrengthДокумент14 страницFabric Bursting StrengthQaiseriqball100% (5)
- Backup and Recovery ScenariosДокумент8 страницBackup and Recovery ScenariosAmit JhaОценок пока нет
- Case Analysis - Compania de Telefonos de ChileДокумент4 страницыCase Analysis - Compania de Telefonos de ChileSubrata BasakОценок пока нет
- Code Description DSMCДокумент35 страницCode Description DSMCAnkit BansalОценок пока нет
- SAP PS Step by Step OverviewДокумент11 страницSAP PS Step by Step Overviewanand.kumarОценок пока нет
- Theme Meal ReportДокумент10 страницTheme Meal Reportapi-434982019Оценок пока нет
- DrugДокумент2 страницыDrugSaleha YounusОценок пока нет
- ARMOR Winter-Spring 2018 EditionДокумент84 страницыARMOR Winter-Spring 2018 Editionmai100Оценок пока нет
- Improvements To Increase The Efficiency of The Alphazero Algorithm: A Case Study in The Game 'Connect 4'Документ9 страницImprovements To Increase The Efficiency of The Alphazero Algorithm: A Case Study in The Game 'Connect 4'Lam Mai NgocОценок пока нет
- 7th Kannada Science 01Документ160 страниц7th Kannada Science 01Edit O Pics StatusОценок пока нет
- Gattu Madhuri's Resume for ECE GraduateДокумент4 страницыGattu Madhuri's Resume for ECE Graduatedeepakk_alpineОценок пока нет
- GS Ep Cor 356Документ7 страницGS Ep Cor 356SangaranОценок пока нет
- L-1 Linear Algebra Howard Anton Lectures Slides For StudentДокумент19 страницL-1 Linear Algebra Howard Anton Lectures Slides For StudentHasnain AbbasiОценок пока нет
- WitepsolДокумент21 страницаWitepsolAnastasius HendrianОценок пока нет
- Credentials List with Multiple Usernames, Passwords and Expiration DatesДокумент1 страницаCredentials List with Multiple Usernames, Passwords and Expiration DatesJOHN VEGAОценок пока нет
- Salary Slip Oct PacificДокумент1 страницаSalary Slip Oct PacificBHARAT SHARMAОценок пока нет
- Flare Finance Ecosystem MapДокумент1 страницаFlare Finance Ecosystem MapEssence of ChaОценок пока нет
- Dissolved Oxygen Primary Prod Activity1Документ7 страницDissolved Oxygen Primary Prod Activity1api-235617848Оценок пока нет
- Discretionary Lending Power Updated Sep 2012Документ28 страницDiscretionary Lending Power Updated Sep 2012akranjan888Оценок пока нет
- Employee Central Payroll PDFДокумент4 страницыEmployee Central Payroll PDFMohamed ShanabОценок пока нет
- A320 Normal ProceduresДокумент40 страницA320 Normal ProceduresRajesh KumarОценок пока нет
- Bancassurance Black Book Rahul 777-2Документ62 страницыBancassurance Black Book Rahul 777-2Shubham ShahОценок пока нет