Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
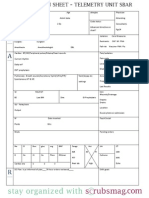
- Nurse Brain Sheet Telemetry Unit SBARДокумент1 страницаNurse Brain Sheet Telemetry Unit SBARvsosa624Оценок пока нет
- Nurse Brain Sheet With Shift HoursДокумент2 страницыNurse Brain Sheet With Shift HoursLauren Cournoyer Foreman100% (4)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Nurse Brain Sheet Half SizeДокумент1 страницаNurse Brain Sheet Half SizeRobyn GrogitskyОценок пока нет
- Alcohol Withdrawal Care PlanДокумент1 страницаAlcohol Withdrawal Care PlanVanessaMUeller100% (1)
- Comprehensive Head To Toe Assessment PDFДокумент22 страницыComprehensive Head To Toe Assessment PDFVanessaMUellerОценок пока нет
- A Case Study On Anemia of Chronic DiseaseДокумент44 страницыA Case Study On Anemia of Chronic DiseaseKeThSantiban100% (3)
- Lab Values Chart GuideДокумент5 страницLab Values Chart GuideVanessaMUeller100% (3)
- AssessingWounds ProcedureДокумент3 страницыAssessingWounds ProcedureVanessaMUellerОценок пока нет
- Alcohol Withdrawal Care PlanДокумент1 страницаAlcohol Withdrawal Care PlanVanessaMUellerОценок пока нет
- Physical Assessment ChartДокумент1 страницаPhysical Assessment ChartVanessaMUellerОценок пока нет
- AdmimДокумент2 страницыAdmimVanessaMUellerОценок пока нет
- ManagmentДокумент1 страницаManagmentVanessaMUellerОценок пока нет
- Penuemonia Care PalnДокумент2 страницыPenuemonia Care PalnVanessaMUellerОценок пока нет
- Updated Clinical SheetДокумент1 страницаUpdated Clinical SheetVanessaMUellerОценок пока нет
- Name Age Room Code Dr. Isolation Activity Diet Allergy: DX: HXДокумент1 страницаName Age Room Code Dr. Isolation Activity Diet Allergy: DX: HXVanessaMUellerОценок пока нет
- Newborn Assessment NORMALДокумент2 страницыNewborn Assessment NORMALVanessaMUellerОценок пока нет
- Example 1 - Focus: Nausea Related To AnestheticДокумент1 страницаExample 1 - Focus: Nausea Related To AnestheticVanessaMUellerОценок пока нет
- COPD Care PLAN PDFДокумент2 страницыCOPD Care PLAN PDFVanessaMUeller100% (1)
- Fluid/Electrolyte Imbalance S/S Nursing Care Fluid DeficitДокумент1 страницаFluid/Electrolyte Imbalance S/S Nursing Care Fluid DeficitVanessaMUellerОценок пока нет
- Nurse Brain Sheet Half SizeДокумент1 страницаNurse Brain Sheet Half Sizevsosa624Оценок пока нет
- Fluid/Electrolyte Imbalance S/S Nursing Care Fluid DeficitДокумент1 страницаFluid/Electrolyte Imbalance S/S Nursing Care Fluid DeficitVanessaMUellerОценок пока нет
- Diseases With Dermatologic ManifestationsДокумент1 страницаDiseases With Dermatologic ManifestationsVanessaMUellerОценок пока нет
- (Chapter 3) : Cell BiologyДокумент80 страниц(Chapter 3) : Cell BiologyVanessaMUellerОценок пока нет
- IV PushДокумент3 страницыIV PushVanessaMUeller100% (1)
- Example 1 - Focus: Nausea Related To AnestheticДокумент1 страницаExample 1 - Focus: Nausea Related To AnestheticVanessaMUellerОценок пока нет
- Medication Guide with Side Effects and UsesДокумент10 страницMedication Guide with Side Effects and UsesVanessaMUellerОценок пока нет
- Clinical AssessementДокумент2 страницыClinical AssessementVanessaMUellerОценок пока нет
- Wound Care PDFДокумент100 страницWound Care PDFVanessaMUellerОценок пока нет
- HR Ocampo Danilo s2 E10 PDFДокумент4 страницыHR Ocampo Danilo s2 E10 PDFVanessaMUellerОценок пока нет
- Wound Care PDFДокумент100 страницWound Care PDFVanessaMUeller100% (2)
- Decongestants & Anti-Histamine Jul 2009Документ63 страницыDecongestants & Anti-Histamine Jul 2009Anonymous JLfSQ29FZPОценок пока нет
- Escala BristolДокумент7 страницEscala BristolAlvaro Jose Cabral MicucciОценок пока нет
- D H AДокумент250 страницD H AKath Cuevas0% (1)
- Milieu TherapyДокумент22 страницыMilieu TherapyAnusikta PandaОценок пока нет
- Referat - Trauma OculiДокумент22 страницыReferat - Trauma OculiBesseMarwah AgusHusainОценок пока нет
- LSHTM ProspectusДокумент32 страницыLSHTM ProspectusNayeon KimОценок пока нет
- TB PolicyДокумент174 страницыTB PolicyDrashua AshuaОценок пока нет
- Test Bank of Neurocognitive DisordersДокумент27 страницTest Bank of Neurocognitive DisordersmОценок пока нет
- Legal standard of care shifts from BolamДокумент4 страницыLegal standard of care shifts from BolamthanasegarОценок пока нет
- Pharmacology of The BloodДокумент63 страницыPharmacology of The BloodSawsan Z. JwaiedОценок пока нет
- Aspartame's DangersДокумент67 страницAspartame's DangersCrazy LukeОценок пока нет
- 3) Ayushman Bharat - CPHCДокумент18 страниц3) Ayushman Bharat - CPHCShankar MurariОценок пока нет
- Jonsen SieglerДокумент2 страницыJonsen SieglerBramantyo NugrahaОценок пока нет
- Epigenetics Congress 2018 BookДокумент120 страницEpigenetics Congress 2018 BookAnonymous FoOawtbV8Оценок пока нет
- Hiv-Aids: Gladys Ziregbe (MRS.)Документ25 страницHiv-Aids: Gladys Ziregbe (MRS.)Esther Anabu EzimaОценок пока нет
- Sign 116Документ170 страницSign 116Nick TarazonaОценок пока нет
- Pentecostal Perspectives: Faith Healing of Cancer and HIV/AIDSДокумент3 страницыPentecostal Perspectives: Faith Healing of Cancer and HIV/AIDStruevine_ministryОценок пока нет
- Ethics Quiz 1Документ4 страницыEthics Quiz 1Estelle LegrosОценок пока нет
- Perbedaan Vertigo Sentral Dan PeriferДокумент5 страницPerbedaan Vertigo Sentral Dan PeriferAditya SahidОценок пока нет
- UntitledДокумент12 страницUntitledjhony192Оценок пока нет
- Delfinm QsenДокумент57 страницDelfinm Qsenapi-346220114Оценок пока нет
- Guide to Cardiovascular Exam StepsДокумент8 страницGuide to Cardiovascular Exam StepsMark GuirguisОценок пока нет
- A Single-Arm Study of Sublobar Resection For Ground-Glass Opacity Dominant Peripheral Lung CancerДокумент15 страницA Single-Arm Study of Sublobar Resection For Ground-Glass Opacity Dominant Peripheral Lung CancerYTM LoongОценок пока нет
- Reaction PaperДокумент4 страницыReaction PaperJam Knows RightОценок пока нет
- Berra 2020Документ12 страницBerra 2020Indri AswariОценок пока нет
- GDM Patient TeachingДокумент2 страницыGDM Patient TeachingBel CortezОценок пока нет
- DXN Testimonies On Health by Edwin MamarilДокумент18 страницDXN Testimonies On Health by Edwin MamarilEdwin Mamaril33% (3)
- 1st IBRO UM5 School ProgramДокумент9 страниц1st IBRO UM5 School ProgramInternational Brain Research OrganizationОценок пока нет
- Ent Secretory Otitis MediaДокумент3 страницыEnt Secretory Otitis MediaIrena DayehОценок пока нет