Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- EDIT Respiratory Failure Assessment and Problem SolvingДокумент66 страницEDIT Respiratory Failure Assessment and Problem Solvingmursidstone.mursidОценок пока нет
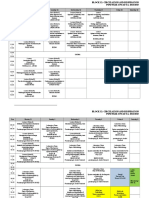
- Revisi Jadwal Blok 12 PK - 2015Документ7 страницRevisi Jadwal Blok 12 PK - 2015mursidstone.mursidОценок пока нет
- Circulation and RespirationДокумент18 страницCirculation and Respirationmursidstone.mursidОценок пока нет
- Recommendations For The Cardiovascular Screening of AthletesДокумент8 страницRecommendations For The Cardiovascular Screening of Athletesmursidstone.mursidОценок пока нет
- Lampiran 2 Analisis Data Pengujian Distribusi Data: Case Processing SummaryДокумент8 страницLampiran 2 Analisis Data Pengujian Distribusi Data: Case Processing Summarymursidstone.mursidОценок пока нет
- Daftar Pustaka: Systematic Review. WHO. (Cited 2016 September 03) - Available FromДокумент6 страницDaftar Pustaka: Systematic Review. WHO. (Cited 2016 September 03) - Available Frommursidstone.mursidОценок пока нет
- Anova Atp Basf Che Adenosine Trifosfat: Analysis of VariansДокумент1 страницаAnova Atp Basf Che Adenosine Trifosfat: Analysis of Variansmursidstone.mursidОценок пока нет
- Daftar Pustak1Документ4 страницыDaftar Pustak1mursidstone.mursidОценок пока нет
- Aedes Sp. Analysis of Variance Baden Aniline and Soda FactoryДокумент3 страницыAedes Sp. Analysis of Variance Baden Aniline and Soda Factorymursidstone.mursidОценок пока нет
- Balai Litbang P2B2Документ1 страницаBalai Litbang P2B2mursidstone.mursidОценок пока нет
- Analysis of Variance: LC: Lethal Concentration 50 LDДокумент1 страницаAnalysis of Variance: LC: Lethal Concentration 50 LDmursidstone.mursidОценок пока нет
- Six Steps On Prescribing: Rustamaji/dr. Fian Faculty of Medicine Universitas Gadjah Mada/ Univ Tadulako 2016Документ28 страницSix Steps On Prescribing: Rustamaji/dr. Fian Faculty of Medicine Universitas Gadjah Mada/ Univ Tadulako 2016mursidstone.mursidОценок пока нет
- Drug and Therapeutics Committee: Standard Treatment GuidelinesДокумент26 страницDrug and Therapeutics Committee: Standard Treatment Guidelinesmursidstone.mursidОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- OrganigramДокумент1 страницаOrganigramCrys TahОценок пока нет
- Atlas of Osteopathic TechniquesДокумент81 страницаAtlas of Osteopathic TechniquesDanieleОценок пока нет
- Accredited Naga DoctorsДокумент5 страницAccredited Naga DoctorsAlt Joe BeeОценок пока нет
- 2018 Physician Compensation ReportДокумент23 страницы2018 Physician Compensation ReportPОценок пока нет
- Neurosurgery Direct 6 Yrs PDFДокумент31 страницаNeurosurgery Direct 6 Yrs PDFSoumitraОценок пока нет
- Dr. Sahar RakhshanfarДокумент2 страницыDr. Sahar RakhshanfarsaharrakhshanfarinfОценок пока нет
- Colitis UlcerrosaДокумент5 страницColitis UlcerrosaCarlos MichasОценок пока нет
- Journal Club: Surfactant Therapy in Premature InfantsДокумент44 страницыJournal Club: Surfactant Therapy in Premature InfantsSubash PaudealОценок пока нет
- Benign Paroxysmal Positional Vertigo Pathophysiology, Causes, Canal Variants and Treatment PDFДокумент8 страницBenign Paroxysmal Positional Vertigo Pathophysiology, Causes, Canal Variants and Treatment PDFegyzellahsОценок пока нет
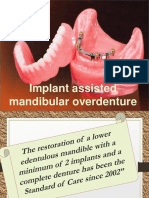
- Mandibular Overdenture PDFДокумент103 страницыMandibular Overdenture PDFIbrahim Ahmed Dahab100% (1)
- Monocular Elevation Deficiency (Double Elevator Palsy) A Cautionary NoteДокумент2 страницыMonocular Elevation Deficiency (Double Elevator Palsy) A Cautionary NotePhilip McNelson100% (1)
- 2015 Motor Skills Development in InfancyДокумент7 страниц2015 Motor Skills Development in InfancyFany Videla FredesОценок пока нет
- Pulmonary Function TestsДокумент24 страницыPulmonary Function TestsSachin KonkaniОценок пока нет
- Developmental Dysplasia of The HipДокумент5 страницDevelopmental Dysplasia of The HipMavra zОценок пока нет
- Carlie's Story: by Tami Perez-MesaДокумент6 страницCarlie's Story: by Tami Perez-MesaJennifer HeinОценок пока нет
- Quality Awards: HealthcareДокумент15 страницQuality Awards: HealthcareNambi WanguluОценок пока нет
- 1185-Liite EASA - Safety Facts Requiring Cabin Crew Unaffected Colour VisionДокумент18 страниц1185-Liite EASA - Safety Facts Requiring Cabin Crew Unaffected Colour VisionGiorgio PupilloОценок пока нет
- Cis Self-Study Lesson Plan: Otolaryngological InstrumentationДокумент4 страницыCis Self-Study Lesson Plan: Otolaryngological Instrumentationjerimiah_manzonОценок пока нет
- Effects of Herbal Lollipops On Streptococcus Mutans Levels and The Dental Caries Experience of Children With Asthma Taking B2-Adrenergic Agonish DrugsДокумент23 страницыEffects of Herbal Lollipops On Streptococcus Mutans Levels and The Dental Caries Experience of Children With Asthma Taking B2-Adrenergic Agonish Drugsinfo6680Оценок пока нет
- Visual PathwayДокумент36 страницVisual PathwayVishakh Isloor100% (1)
- Bladder PDFДокумент22 страницыBladder PDFSuci Mega SariОценок пока нет
- Congenital Lobar EmphysemaДокумент25 страницCongenital Lobar Emphysemasheme1711Оценок пока нет
- 1 Childhood Nephrotic Syndrome - Diagnosis and ManagementДокумент52 страницы1 Childhood Nephrotic Syndrome - Diagnosis and ManagementThana Balan100% (1)
- Basal Cell Carcinoma: CausesДокумент5 страницBasal Cell Carcinoma: CausesRini LianingsihОценок пока нет
- FibroScan Physician Slideset 1.11.2016Документ37 страницFibroScan Physician Slideset 1.11.2016Prudhvi Krishna Reddy100% (1)
- Root Word Lists 1-12, As English IIДокумент9 страницRoot Word Lists 1-12, As English IIakvssakthivelОценок пока нет
- Nephrotic Case Study With AnswersДокумент3 страницыNephrotic Case Study With AnswersKBОценок пока нет
- First Aid 2013 PDFДокумент725 страницFirst Aid 2013 PDFTom0% (2)
- Atlas NeuroanatomyДокумент874 страницыAtlas NeuroanatomyBilge Yilmaz100% (3)
- Visual Requirements For Driving: by Catharine Chisholm PHD Mcoptom, University of BradfordДокумент5 страницVisual Requirements For Driving: by Catharine Chisholm PHD Mcoptom, University of Bradfordagisab100% (1)