Вам также может понравиться
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Macrocycle-Antibiotic Hybrids: A Path To Clinical CandidatesДокумент16 страницMacrocycle-Antibiotic Hybrids: A Path To Clinical CandidatesMung MingОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Microbiology ProfileДокумент52 страницыMicrobiology ProfileRushikesh LadОценок пока нет
- 1 2 2 A WhichantibioticbestДокумент4 страницы1 2 2 A Whichantibioticbestapi-327503253Оценок пока нет
- Dry Powder Injectables TheonДокумент1 страницаDry Powder Injectables TheonshugarcontrollОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Medicinal Chemistry - PenicillinДокумент39 страницMedicinal Chemistry - PenicillinV G Viju KumarОценок пока нет
- Management of Medical Emergencies in The Dental OfficeДокумент38 страницManagement of Medical Emergencies in The Dental OfficeJohan Edward Franklin MarpaungОценок пока нет
- Texila American University: Article Review GuidelineДокумент10 страницTexila American University: Article Review GuidelinecindyОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- NCP SinusitisДокумент7 страницNCP SinusitisBeverly May Ambut71% (7)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- ? PHARMA 3. Anti InfectivesДокумент130 страниц? PHARMA 3. Anti InfectivesMiguel Luis NavarreteОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- BED12 - Antibiotics PharmacologyДокумент2 страницыBED12 - Antibiotics PharmacologyAmir AmirulОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Microbiology SyllabusДокумент5 страницMicrobiology SyllabushhgОценок пока нет
- Injeksi & Oplosan ObatДокумент16 страницInjeksi & Oplosan ObatFebriani RatnaОценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- WDDTYДокумент100 страницWDDTYgfrankel72100% (1)
- Preps 4-61Документ57 страницPreps 4-61fianaОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Jurnal Cefpirome Sulfat PDFДокумент8 страницJurnal Cefpirome Sulfat PDFd_mayavieОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- DAFTAR PENERIMAAN (Version 1)Документ342 страницыDAFTAR PENERIMAAN (Version 1)fennyrahmaОценок пока нет
- B.Sc. TY Biotechnology PDFДокумент26 страницB.Sc. TY Biotechnology PDFHanumant Suryawanshi0% (1)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Committee On Herbal Medicinal Products (HMPC) : Evaluation of Medicines For Human UseДокумент11 страницCommittee On Herbal Medicinal Products (HMPC) : Evaluation of Medicines For Human Useroger024Оценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- PT Quantum LabsДокумент4 страницыPT Quantum LabsCipuut PutriОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- AntisepticДокумент6 страницAntisepticSaud AhmadОценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Overview On Mechanisms of Antibacterial Resistance: Alemayehu Toma, Serawit DeynoДокумент10 страницOverview On Mechanisms of Antibacterial Resistance: Alemayehu Toma, Serawit DeynowaelОценок пока нет
- Antibiotics &anti-Infective AgentsДокумент39 страницAntibiotics &anti-Infective AgentsKC PalattaoОценок пока нет
- Etanol BacteriaДокумент38 страницEtanol BacteriaWida YantiОценок пока нет
- Chapter 09 Controlling Microbial Growth in Vivo Using Antimicrobial AgentsДокумент49 страницChapter 09 Controlling Microbial Growth in Vivo Using Antimicrobial AgentsSherinne Jane Cariazo100% (1)
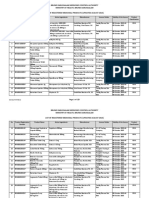
- Brunei Registered Medicinal ProductsДокумент123 страницыBrunei Registered Medicinal ProductsportosinОценок пока нет
- The Eagle Effect and Antibiotic-Induced PersistenceДокумент16 страницThe Eagle Effect and Antibiotic-Induced PersistenceClaudio Daniel UbillaОценок пока нет
- Beta - Lactam Antibiotics: Prof. R. K. Dixit Pharmacology and Therapeutics K. G. M. U. LucknowДокумент29 страницBeta - Lactam Antibiotics: Prof. R. K. Dixit Pharmacology and Therapeutics K. G. M. U. LucknowHely PatelОценок пока нет
- Stok 4 Juli 19Документ27 страницStok 4 Juli 19Pujiastuti WahidahОценок пока нет
- Irrational Use of DrugДокумент9 страницIrrational Use of Drugsreedam100% (2)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Chapter 5 FT EditedДокумент35 страницChapter 5 FT EditedPuvenez Tamalantan100% (5)