Вам также может понравиться
- Pain scale guideДокумент4 страницыPain scale guidethilaga88Оценок пока нет
- Best Test - Mini Best TestДокумент23 страницыBest Test - Mini Best Testjorgelina_riveraОценок пока нет
- Quick DASHДокумент4 страницыQuick DASHKennedy Hindley100% (1)
- FunctionalДокумент1 страницаFunctionalotmom18Оценок пока нет
- Assessment of HandДокумент76 страницAssessment of Handchirag0% (1)
- Home Environmental AssessmentДокумент2 страницыHome Environmental AssessmentSelvi Puspa SariОценок пока нет
- Occupational Therapy Now Volume 14.5Документ32 страницыOccupational Therapy Now Volume 14.5Sara Gomes CastroОценок пока нет
- OT Self Care Modified Barthel IndexДокумент4 страницыOT Self Care Modified Barthel Indexlolocy LОценок пока нет
- FIM or WeeFIM Assessment Scoresheet 2020Документ3 страницыFIM or WeeFIM Assessment Scoresheet 2020Mayco BiasibettiОценок пока нет
- Barthel IndexДокумент4 страницыBarthel IndexrlinaoОценок пока нет
- Fim Item ScoringДокумент10 страницFim Item Scoringhaythamalshikh0120% (1)
- Sitbat 16item FinalДокумент6 страницSitbat 16item FinalMae NocheОценок пока нет
- FIM ManualДокумент24 страницыFIM ManualAnshuman MihirОценок пока нет
- OT8 - Thumb Immobilization SplintДокумент4 страницыOT8 - Thumb Immobilization SplintAnnbe Barte100% (1)
- Sensory Re-Education: Hand Physiotherapy DepartmentДокумент2 страницыSensory Re-Education: Hand Physiotherapy DepartmentEmanuel George StoenescuОценок пока нет
- Design of A Hand OrthosisДокумент251 страницаDesign of A Hand OrthosisIsrael BlancoОценок пока нет
- Spinal Cord DisordersДокумент50 страницSpinal Cord DisordersIsaac Mwangi100% (1)
- Spinal Cord Assesment Form PTДокумент8 страницSpinal Cord Assesment Form PTSureaka PonnusamyОценок пока нет
- Part 2: Social Skills Training: RatingДокумент3 страницыPart 2: Social Skills Training: RatingGina GucioОценок пока нет
- Week 9 - Ch. 31 - SkinДокумент31 страницаWeek 9 - Ch. 31 - SkinMary SingletonОценок пока нет
- EBRSR Handbook Chapter 4 - Upper Extremity Post Stroke - MLДокумент60 страницEBRSR Handbook Chapter 4 - Upper Extremity Post Stroke - MLanjelikaОценок пока нет
- Strategies Used by Occupational Therapy To Maximize ADL IndependenceДокумент53 страницыStrategies Used by Occupational Therapy To Maximize ADL IndependenceNizam lotfiОценок пока нет
- OARS Adl IadlДокумент5 страницOARS Adl IadlSamuelОценок пока нет
- 6соurse 2 variant 2019Документ57 страниц6соurse 2 variant 2019Sampath KumarОценок пока нет
- ROM and manual stretching worksheetДокумент12 страницROM and manual stretching worksheetMike ConnorsОценок пока нет
- Wolf Motor Function TestДокумент23 страницыWolf Motor Function TestSai RamОценок пока нет
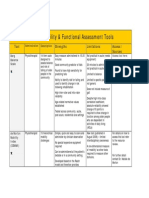
- Assessment Tools for Mobility & Functional IndependenceДокумент4 страницыAssessment Tools for Mobility & Functional Independencesonya63265Оценок пока нет
- Valparcomponent Work Sampel4: Upper Extremity Range of MotionДокумент6 страницValparcomponent Work Sampel4: Upper Extremity Range of MotionLc DafhnyeОценок пока нет
- Cognitive Rehabilitation For Occupational Outcomes After Traumatic Brain InjuryДокумент9 страницCognitive Rehabilitation For Occupational Outcomes After Traumatic Brain InjuryHardeep Singh BaliОценок пока нет
- LOTCA Assessment ReviewДокумент10 страницLOTCA Assessment ReviewManik MishraОценок пока нет
- Tetraplegia Hand Activity QuestionnaireДокумент20 страницTetraplegia Hand Activity QuestionnaireISLinkОценок пока нет
- Gait in Children With Cerebral PalsyДокумент5 страницGait in Children With Cerebral PalsyvarahamihirОценок пока нет
- Discharge ReportДокумент3 страницыDischarge Reportapi-383274221Оценок пока нет
- Sternal PrecautionsДокумент33 страницыSternal PrecautionsJennifer Snell WelterОценок пока нет
- Rol Del To en Disfagia OrofaringeaДокумент24 страницыRol Del To en Disfagia OrofaringeaMCris EsSemОценок пока нет
- Malnutrition Prevalence, Outcomes, and CostsДокумент18 страницMalnutrition Prevalence, Outcomes, and CostsNOTHING KarmaОценок пока нет
- SCI Acute Care and Rehabilitation PT 2009Документ265 страницSCI Acute Care and Rehabilitation PT 2009api-3822828Оценок пока нет
- Katz Index of Independence in Activities of Daily LivingДокумент1 страницаKatz Index of Independence in Activities of Daily LivingWarnet IlalangОценок пока нет
- Development Chart For BookletДокумент13 страницDevelopment Chart For BookletzapelОценок пока нет
- Wota2: Water Orientation Test Alyn 2Документ2 страницыWota2: Water Orientation Test Alyn 2Sergio CurteanОценок пока нет
- Jebsen Hand Function TestДокумент2 страницыJebsen Hand Function TestAtiKa YuLiantiОценок пока нет
- Lateral Epicondylitis - Tennis Ellbow HandoutДокумент5 страницLateral Epicondylitis - Tennis Ellbow Handoutgermany23Оценок пока нет
- Berg Balance ScaleДокумент4 страницыBerg Balance ScaleMeibyInginkhanKhasanahCintaОценок пока нет
- OT 460 Intervention Kit AssignmentДокумент2 страницыOT 460 Intervention Kit AssignmentMegan McCarthyОценок пока нет
- Assessment of Activities of Daily Living in Patients Post COVID-19: A Systematic ReviewДокумент18 страницAssessment of Activities of Daily Living in Patients Post COVID-19: A Systematic Reviewjavieron11Оценок пока нет
- Instrumental Activities Daily Living: Try ThisДокумент11 страницInstrumental Activities Daily Living: Try ThisbalryoОценок пока нет
- Orthosisofhandppt 181202162551Документ65 страницOrthosisofhandppt 181202162551Khageswar SamalОценок пока нет
- CLOXДокумент3 страницыCLOXanouk_dirkx6883Оценок пока нет
- AprJul2017 PublicReportДокумент130 страницAprJul2017 PublicReportAgnes Claudia100% (1)
- Dysphagia in Huntington's Disease ReviewedДокумент5 страницDysphagia in Huntington's Disease ReviewedDani PiñaОценок пока нет
- Assessing Functional AbilityДокумент15 страницAssessing Functional AbilitySonali Soumyashree100% (2)
- PANat - Thetrical - Air Splints - Talas Pneumaticas Margaret JohnstoneДокумент44 страницыPANat - Thetrical - Air Splints - Talas Pneumaticas Margaret JohnstonePedro GouveiaОценок пока нет
- The Canadian Model of Occupational Performance and EngagementДокумент16 страницThe Canadian Model of Occupational Performance and Engagementalepati29Оценок пока нет
- Stroke UE ToolkitДокумент69 страницStroke UE ToolkitWhitney JosephОценок пока нет
- Ot Cota Skills Checklist 2Документ4 страницыOt Cota Skills Checklist 2Monica Smith FoxОценок пока нет
- Occupation Analysis in PracticeОт EverandOccupation Analysis in PracticeLynette MackenzieОценок пока нет
- Balance Dysfunction in Parkinson’s Disease: Basic Mechanisms to Clinical ManagementОт EverandBalance Dysfunction in Parkinson’s Disease: Basic Mechanisms to Clinical ManagementОценок пока нет
- The Multicontext Approach to Cognitive Rehabilitation: A Metacognitive Strategy Intervention to Optimize Functional CognitionОт EverandThe Multicontext Approach to Cognitive Rehabilitation: A Metacognitive Strategy Intervention to Optimize Functional CognitionОценок пока нет
- Movement Difficulties in Developmental Disorders: Practical Guidelines for Assessment and ManagementОт EverandMovement Difficulties in Developmental Disorders: Practical Guidelines for Assessment and ManagementОценок пока нет
- Belageddu Yaara Mukava Naanu NodideДокумент2 страницыBelageddu Yaara Mukava Naanu NodidedrrselvarajОценок пока нет
- Weight loss Diet Chart for 7 DaysДокумент5 страницWeight loss Diet Chart for 7 DaysdrrselvarajОценок пока нет
- What Is AcupunctureДокумент6 страницWhat Is AcupuncturedrrselvarajОценок пока нет
- Belageddu Yaara Mukava Naanu NodideДокумент2 страницыBelageddu Yaara Mukava Naanu NodidedrrselvarajОценок пока нет
- Social Change and Adolescent Development: Issues and ChallengesДокумент15 страницSocial Change and Adolescent Development: Issues and ChallengesdrrselvarajОценок пока нет
- Affidavit 1Документ3 страницыAffidavit 1drrselvarajОценок пока нет
- Low Back PainДокумент2 страницыLow Back PaindrrselvarajОценок пока нет
- NATUROPATHYДокумент2 страницыNATUROPATHYdrrselvarajОценок пока нет
- Guide to internship rolesДокумент18 страницGuide to internship rolesShowketОценок пока нет
- List of Conditions That Can Be Treated With Yoga InterventionДокумент2 страницыList of Conditions That Can Be Treated With Yoga InterventiondrrselvarajОценок пока нет
- ReadmeДокумент2 страницыReadmedrrselvarajОценок пока нет
- NSIC & GOVT - Bengaluru Whom To ContactДокумент2 страницыNSIC & GOVT - Bengaluru Whom To ContactdrrselvarajОценок пока нет
- Belageddu Yaara Mukava Naanu NodideДокумент2 страницыBelageddu Yaara Mukava Naanu NodidedrrselvarajОценок пока нет
- MPC 003Документ2 страницыMPC 003KalyaniGadreОценок пока нет
- MPC 003 Dec 2011Документ7 страницMPC 003 Dec 2011drrselvarajОценок пока нет
- Kasturi Ispat PVT LTDДокумент5 страницKasturi Ispat PVT LTDdrrselvarajОценок пока нет
- Kasturi Ispat PVT LTDДокумент3 страницыKasturi Ispat PVT LTDdrrselvarajОценок пока нет
- 11 Factorial Designs ShortДокумент25 страниц11 Factorial Designs ShortdrrselvarajОценок пока нет
- Kasturi Ispat PVT LTDДокумент3 страницыKasturi Ispat PVT LTDdrrselvarajОценок пока нет
- Appendix 1 Preliminary Study Report PDFДокумент3 страницыAppendix 1 Preliminary Study Report PDFdrrselvarajОценок пока нет
- MDS Research Criteria for Prodromal Parkinson's DiseaseДокумент10 страницMDS Research Criteria for Prodromal Parkinson's DiseasedrrselvarajОценок пока нет
- I-Aim Health Care Centre: Patients Daily Yoga Schedule Date: 1/10/2016 Sl. No MR No Name Referred by TimeДокумент1 страницаI-Aim Health Care Centre: Patients Daily Yoga Schedule Date: 1/10/2016 Sl. No MR No Name Referred by TimedrrselvarajОценок пока нет
- LDOPA Asso Recovery PDFДокумент4 страницыLDOPA Asso Recovery PDFdrrselvarajОценок пока нет
- Appendix 3. Uk Brain Bank Criteria PDFДокумент1 страницаAppendix 3. Uk Brain Bank Criteria PDFdrrselvarajОценок пока нет
- I-Aim Health Care Centre: OP 10am-11amДокумент2 страницыI-Aim Health Care Centre: OP 10am-11amAyyush RajalingaОценок пока нет
- I-AIM Health Centre Daily Yoga ScheduleДокумент1 страницаI-AIM Health Centre Daily Yoga ScheduleAyyush RajalingaОценок пока нет
- Assembling Ayurveda's Best-Selling MedicineДокумент13 страницAssembling Ayurveda's Best-Selling MedicinedrrselvarajОценок пока нет
- I-AIM Healthcare Centre Daily Yoga ScheduleДокумент1 страницаI-AIM Healthcare Centre Daily Yoga ScheduleAyyush RajalingaОценок пока нет
- Jan 26th 29thДокумент1 страницаJan 26th 29thdrrselvarajОценок пока нет
- FCM 2.06Документ4 страницыFCM 2.06Maikka IlaganОценок пока нет
- Conversion Disorder and Spinal Cord Injury Case ReportДокумент5 страницConversion Disorder and Spinal Cord Injury Case ReportHerald Scholarly Open AccessОценок пока нет
- Reproductive and Gender Related AgentsДокумент85 страницReproductive and Gender Related AgentsAyumi StarОценок пока нет
- Liver DiseasesДокумент114 страницLiver DiseasesDayang Feineliza Samman BahjinОценок пока нет
- 1 Q&A Usmle Step 1Документ72 страницы1 Q&A Usmle Step 1Villia DamayantieОценок пока нет
- Rashes: Paediatric Dermatology: Ellis HonДокумент95 страницRashes: Paediatric Dermatology: Ellis HonB AuОценок пока нет
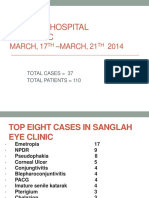
- Sanglah Hospital Eye Clinic: MARCH, 17 - MARCH, 21 2014Документ25 страницSanglah Hospital Eye Clinic: MARCH, 17 - MARCH, 21 2014krisadi30Оценок пока нет
- Drug Study For Multiple Sclerosis (Betaseron)Документ4 страницыDrug Study For Multiple Sclerosis (Betaseron)Leslie Lagat PaguioОценок пока нет
- ParkinsonismДокумент18 страницParkinsonismShivsharanОценок пока нет
- Fundamentals of Nursing Exam 1Документ38 страницFundamentals of Nursing Exam 1Annjelyn Espeleta85% (13)
- 861 Drug Prescribing For Dentistry 2 Web 2 Email PDFДокумент94 страницы861 Drug Prescribing For Dentistry 2 Web 2 Email PDFRaphaela TravassosОценок пока нет
- Nervous System Infections GuideДокумент91 страницаNervous System Infections GuideBea Bianca CruzОценок пока нет
- Top 200 Drugs in OrderДокумент7 страницTop 200 Drugs in OrderEamon BarkhordarianОценок пока нет
- Nejmra 2023911Документ8 страницNejmra 2023911Merry LeeОценок пока нет
- (REV) Neuroanatomy and NeurophysiologyДокумент8 страниц(REV) Neuroanatomy and NeurophysiologyReichelleОценок пока нет
- 4 - LDC Revised Grading of Acute Kidney Injury (1 5)Документ7 страниц4 - LDC Revised Grading of Acute Kidney Injury (1 5)kradoОценок пока нет
- QuestionsДокумент21 страницаQuestionsashaaman0325Оценок пока нет
- Differential Diagnosis of Neck MassesДокумент10 страницDifferential Diagnosis of Neck Massesapi-19916399Оценок пока нет
- About Medical ResearchДокумент21 страницаAbout Medical ResearchMohebОценок пока нет
- ReflectionДокумент4 страницыReflectionelizaviraniОценок пока нет
- Helminth 4Документ1 страницаHelminth 4FarlogyОценок пока нет
- N8 R 9 W3 Pupeyo RF RTWB 42 BRДокумент2 страницыN8 R 9 W3 Pupeyo RF RTWB 42 BRPrashant KumarОценок пока нет
- Manifestations of Systemic Diseases and Conditions That Affect The Periodontal Attachment Apparatus: Case Definitions and Diagnostic ConsiderationsДокумент22 страницыManifestations of Systemic Diseases and Conditions That Affect The Periodontal Attachment Apparatus: Case Definitions and Diagnostic ConsiderationsMarco Antonio García LunaОценок пока нет
- MMDS (Medical Morrtality Data System)Документ1 241 страницаMMDS (Medical Morrtality Data System)Bhella GuntoroОценок пока нет
- Edema Assessment - PhysiopediaДокумент3 страницыEdema Assessment - PhysiopediaJovie Anne Cabangal100% (1)
- Hypertension in Geriatrics 2010Документ51 страницаHypertension in Geriatrics 2010Andre HawkОценок пока нет
- Liver Cirrhosis Pathophysiology and EvaluationДокумент91 страницаLiver Cirrhosis Pathophysiology and EvaluationGiorgi PopiashviliОценок пока нет
- The Hemoglobin E ThalassemiasДокумент16 страницThe Hemoglobin E ThalassemiasJohan EspinozaОценок пока нет
- Pernicious Anemia: BSMT 3D Group 1 Paniza, Erika Joy Villanueva, Andrewarnold Yandan, CharisДокумент53 страницыPernicious Anemia: BSMT 3D Group 1 Paniza, Erika Joy Villanueva, Andrewarnold Yandan, CharisAndrew Arnold David VillanuevaОценок пока нет
- Aubf Review UermДокумент18 страницAubf Review UermZhiddah Japzon0% (1)