Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Scra 2014Документ3 страницыScra 2014Czara DyОценок пока нет
- Barcelote Vs - RepublicДокумент2 страницыBarcelote Vs - RepublicCzara DyОценок пока нет
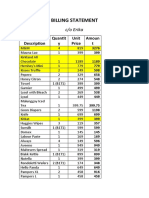
- S&R - Billing StatementДокумент4 страницыS&R - Billing StatementCzara DyОценок пока нет
- Marie Ivonne F. Reyes: Pasig Catholic SchoolДокумент1 страницаMarie Ivonne F. Reyes: Pasig Catholic SchoolCzara DyОценок пока нет
- Corpo Notes 2018 PrelimsДокумент14 страницCorpo Notes 2018 PrelimsCzara DyОценок пока нет
- Banking Mon 7718Документ2 страницыBanking Mon 7718Czara DyОценок пока нет
- Castillo vs. RepublicДокумент2 страницыCastillo vs. RepublicCzara DyОценок пока нет
- Q&A Wills Dean AligadaДокумент5 страницQ&A Wills Dean AligadaCzara DyОценок пока нет
- G.R. No. L-48955, June 30, 1987)Документ8 страницG.R. No. L-48955, June 30, 1987)Czara DyОценок пока нет
- Sunio v. NLRCДокумент3 страницыSunio v. NLRCCzara DyОценок пока нет
- Policarpio Vs Active BankДокумент2 страницыPolicarpio Vs Active BankCzara DyОценок пока нет
- Institution of Heirs. It Will Not Result To IntestacyДокумент9 страницInstitution of Heirs. It Will Not Result To IntestacyCzara DyОценок пока нет
- Nil Cases FinalsДокумент37 страницNil Cases FinalsCzara DyОценок пока нет
- Jimenez vs. FranciscoДокумент1 страницаJimenez vs. FranciscoCzara DyОценок пока нет
- PNB Vs CA DigestДокумент3 страницыPNB Vs CA DigestCzara DyОценок пока нет
- Annum From July 1, 2013 Until Full PaymentДокумент1 страницаAnnum From July 1, 2013 Until Full PaymentCzara DyОценок пока нет
- Reynolds v. Ca (Dy)Документ2 страницыReynolds v. Ca (Dy)Czara DyОценок пока нет
- Memorandum On Charter Change: Presidential Federal ConstitutionДокумент1 страницаMemorandum On Charter Change: Presidential Federal ConstitutionCzara DyОценок пока нет
- Carpio CalaycayДокумент4 страницыCarpio CalaycayCzara DyОценок пока нет
- TORTS Page 2 Cases SyllabusДокумент77 страницTORTS Page 2 Cases SyllabusCzara DyОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- 16 MSDS NaHSO3Документ6 страниц16 MSDS NaHSO3Furqan SiddiquiОценок пока нет
- Fluid Overload and Kidney Injury Score As A PredicДокумент7 страницFluid Overload and Kidney Injury Score As A Predicmira srikandiОценок пока нет
- The Litigation Explosion - Walter K. OlsonДокумент424 страницыThe Litigation Explosion - Walter K. OlsonNaturaleza Salvaje100% (1)
- Psychiatric Clinical SkillsДокумент376 страницPsychiatric Clinical SkillsSamuel Agunbiade100% (5)
- BA 89402175 001100 Innopack EN 00 PDFДокумент293 страницыBA 89402175 001100 Innopack EN 00 PDFBruno GiffoniОценок пока нет
- Drug Name Actions Side Effects Adverse Effects Indications Contraindication S Nursing Responsibilities Generic NameДокумент2 страницыDrug Name Actions Side Effects Adverse Effects Indications Contraindication S Nursing Responsibilities Generic NameMae Abigail Mallonga BunaganОценок пока нет
- Export of SpicesДокумент57 страницExport of SpicesJunaid MultaniОценок пока нет
- Et CareДокумент15 страницEt CarePaulo GarciaОценок пока нет
- 5.3.1 Distinguish Between Learning and Performance: Skill in SportДокумент48 страниц5.3.1 Distinguish Between Learning and Performance: Skill in SportAiham AltayehОценок пока нет
- DLL - Mapeh 6 - Q4 - W6Документ4 страницыDLL - Mapeh 6 - Q4 - W6Bernard Martin100% (1)
- HSG 9 Hà Tĩnh 2021Документ6 страницHSG 9 Hà Tĩnh 2021Cachi100% (1)
- Platelet Analysis - An Overview: HistoryДокумент7 страницPlatelet Analysis - An Overview: HistoryPieter Du Toit-EnslinОценок пока нет
- Health EducationДокумент8 страницHealth EducationJamie Rose FontanillaОценок пока нет
- Dapus FixДокумент2 страницыDapus FixIkrima MuhdarmuhallyОценок пока нет
- Philhealth Circular 013-2015Документ12 страницPhilhealth Circular 013-2015Kim Patrick DayosОценок пока нет
- ORCULLO 3NC NCM114 JournalДокумент4 страницыORCULLO 3NC NCM114 JournalDudil GoatОценок пока нет
- Top 10 Ranking Universities in West Africa 2022Документ1 страницаTop 10 Ranking Universities in West Africa 2022Bright OtchereОценок пока нет
- TorigwiltresumeДокумент2 страницыTorigwiltresumeapi-231010151Оценок пока нет
- My Evaluation in LnuДокумент4 страницыMy Evaluation in LnuReyjan ApolonioОценок пока нет
- Jonathan Glover-Alien LandscapesДокумент448 страницJonathan Glover-Alien LandscapesIrina Soare100% (1)
- Climbing Training Log - TemplateДокумент19 страницClimbing Training Log - TemplateKam Iqar ZeОценок пока нет
- Jeehp 12 06Документ4 страницыJeehp 12 06Sohini KhushiОценок пока нет
- Futuristic Nursing: - Sister Elizabeth DavisДокумент14 страницFuturistic Nursing: - Sister Elizabeth DavisPhebeDimple100% (2)
- A Study To Assess The Effectiveness of Selected Teaching Strategies Knowledge Regarding Drug Calculation Among B.Sc. N Students in Selected College at ChennaiДокумент3 страницыA Study To Assess The Effectiveness of Selected Teaching Strategies Knowledge Regarding Drug Calculation Among B.Sc. N Students in Selected College at ChennaiEditor IJTSRDОценок пока нет
- Liver Disease NutritionДокумент76 страницLiver Disease NutritionIbrahem AlОценок пока нет
- Anemia in PregnancyДокумент5 страницAnemia in PregnancySandra GabasОценок пока нет
- Nebosh Exams Questions and Answers - Nebosh Question Paper 2021Документ4 страницыNebosh Exams Questions and Answers - Nebosh Question Paper 2021faceji67% (3)
- Nursing Exam Questions With AnswerДокумент7 страницNursing Exam Questions With AnswerjavedОценок пока нет
- Secret Chernobyl Documents Expose The CoverUpДокумент6 страницSecret Chernobyl Documents Expose The CoverUpTroy LivingstonОценок пока нет
- Med Tech LawsДокумент78 страницMed Tech LawsMarie LlanesОценок пока нет