Вам также может понравиться
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesОт EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesРейтинг: 4 из 5 звезд4/5 (2)
- Muestra Elsevier's Veterynary Assisting WBДокумент10 страницMuestra Elsevier's Veterynary Assisting WBclau aОценок пока нет
- Immunisation HandbookДокумент546 страницImmunisation HandbookPritam Dugar100% (1)
- Drug Study CardinalДокумент21 страницаDrug Study CardinalDrei LanuzoОценок пока нет
- The 10 Most Common Emergency DrugsДокумент28 страницThe 10 Most Common Emergency DrugsKrishna BalsarzaОценок пока нет
- Treatment Algorithm For Autonomic Dysreflexia (Hypertensive Crisis) in Spinal Cord InjuryДокумент1 страницаTreatment Algorithm For Autonomic Dysreflexia (Hypertensive Crisis) in Spinal Cord InjuryHAYME THARRISОценок пока нет
- Nursing Pharmacology Handouts For ZamboДокумент7 страницNursing Pharmacology Handouts For ZamboAlexa Abidin Oldenborg100% (8)
- Drug Book On EmergencyДокумент21 страницаDrug Book On EmergencyDimpal Choudhary100% (3)
- High Flow Nasal Cannula Oxygen GuidelineДокумент24 страницыHigh Flow Nasal Cannula Oxygen GuidelinekkkssbbОценок пока нет
- High Flow Nasal Cannula Oxygen GuidelineДокумент24 страницыHigh Flow Nasal Cannula Oxygen GuidelinekkkssbbОценок пока нет
- Healthcare Case StudyДокумент31 страницаHealthcare Case StudyKanupriya MadanОценок пока нет
- Pediatric Genetics NotesДокумент96 страницPediatric Genetics Noteskkkssbb100% (1)
- Partograph BoДокумент60 страницPartograph BoRendy Adhitya PratamaОценок пока нет
- ASCIA Guidelines Acute Management Anaphylaxis 2017 Updated PDFДокумент8 страницASCIA Guidelines Acute Management Anaphylaxis 2017 Updated PDFAyu WahyuniОценок пока нет
- Drug Study On Emergency DrugsДокумент14 страницDrug Study On Emergency Drugsjcarysuitos100% (4)
- EpinephrineДокумент3 страницыEpinephrinealexjerimiahОценок пока нет
- High Alert MedicationsДокумент17 страницHigh Alert MedicationsJoanna Marie Datahan EstomoОценок пока нет
- Emergency Pharmacology Drugs GuideДокумент5 страницEmergency Pharmacology Drugs GuideAce RegellanaОценок пока нет
- Pediatric NotesДокумент45 страницPediatric NoteskkkssbbОценок пока нет
- ASCIA Guidelines Acute Management Anaphylaxis 2019Документ8 страницASCIA Guidelines Acute Management Anaphylaxis 2019Asadulla KhanОценок пока нет
- Survival Guide For Medical InternshipДокумент16 страницSurvival Guide For Medical Internshipsuggaplum0% (1)
- Drug StudyДокумент10 страницDrug StudyFritzie Beatrice NomusОценок пока нет
- AnaphylaxisДокумент1 страницаAnaphylaxisMazo KhanОценок пока нет
- Haad ExamДокумент5 страницHaad ExamGamaliel Season100% (3)
- Katerero KunyazaДокумент6 страницKaterero KunyazaPeter Kamala100% (1)
- Bibliometric AnalysisДокумент6 страницBibliometric AnalysisMuhammad Jamshaid RasheedОценок пока нет
- Emergency Drugs Drug StudyДокумент15 страницEmergency Drugs Drug StudyCathrine Sandile Tangwara100% (1)
- Tetraplegia & Paraplegia PDFДокумент278 страницTetraplegia & Paraplegia PDFAnca50% (2)
- Drug StudyДокумент14 страницDrug StudyJho Ocampo NungayОценок пока нет
- ASCIA Guidelines ADVANCED Acute Management Anaphylaxis Dec2016Документ7 страницASCIA Guidelines ADVANCED Acute Management Anaphylaxis Dec2016SPV DoctorОценок пока нет
- ASCIA Acute Management of Anaphylaxis Guidelines 2015Документ4 страницыASCIA Acute Management of Anaphylaxis Guidelines 2015tom8989Оценок пока нет
- Acute Management of Anaphylaxis: Adrenaline (Epinephrine) Is The First Line Treatment For AnaphylaxisДокумент8 страницAcute Management of Anaphylaxis: Adrenaline (Epinephrine) Is The First Line Treatment For AnaphylaxissigmapomalОценок пока нет
- ASCIA HP Guidelines Acute Management Anaphylaxis 2020Документ8 страницASCIA HP Guidelines Acute Management Anaphylaxis 2020Munshi KamrulОценок пока нет
- Anaphylaxis emergency managementДокумент1 страницаAnaphylaxis emergency managementAymane El KandoussiОценок пока нет
- Anaphylaxis Wallchart 2018Документ1 страницаAnaphylaxis Wallchart 2018simranОценок пока нет
- Pediatric Life SupportДокумент33 страницыPediatric Life SupportAndre montolaluОценок пока нет
- Emergency Pediatric AidsДокумент29 страницEmergency Pediatric AidsRana SalemОценок пока нет
- Anaphylaxis Articulo CompletoДокумент6 страницAnaphylaxis Articulo CompletoFrancelia Quiñonez RuvalcabaОценок пока нет
- Should Be Available at All Sites If Feasible, Include at Sites (Not Required)Документ5 страницShould Be Available at All Sites If Feasible, Include at Sites (Not Required)Ahmed QlhamdОценок пока нет
- Opiates (E.g. Codeine, Heroin, Pethidine, Morphine, Methadone)Документ7 страницOpiates (E.g. Codeine, Heroin, Pethidine, Morphine, Methadone)Ali HussnainОценок пока нет
- Aclspediatric BradycardiaДокумент2 страницыAclspediatric BradycardiasalamredОценок пока нет
- EMERGENCY TREATMENT OF ANAPHYLACTIC REACTIONSДокумент40 страницEMERGENCY TREATMENT OF ANAPHYLACTIC REACTIONS'ranu HerjunaОценок пока нет
- DrugmedsДокумент52 страницыDrugmedsshirleyОценок пока нет
- Paracetamol IV administration side effects nursing considerationsДокумент7 страницParacetamol IV administration side effects nursing considerationsCharm LorenzoОценок пока нет
- Nursing responsibilities for magnesium sulfate, ferrous sulfate, antibiotics, and postoperative careДокумент13 страницNursing responsibilities for magnesium sulfate, ferrous sulfate, antibiotics, and postoperative careabrokenheartedgirlОценок пока нет
- Pediatric Life Support SHGДокумент32 страницыPediatric Life Support SHGIwan SinagaОценок пока нет
- Syok Anafilaksis 1Документ4 страницыSyok Anafilaksis 1Mariatun Zahro NasutionОценок пока нет
- Medical Emergencies at a GlanceДокумент31 страницаMedical Emergencies at a GlanceNigam SattarОценок пока нет
- Management of Medical Emeregency in Dental PracticeДокумент51 страницаManagement of Medical Emeregency in Dental Practicechoudharyishita163Оценок пока нет
- Emergency Oxygen Therapy for Cardiac IssuesДокумент11 страницEmergency Oxygen Therapy for Cardiac IssuesMin Hong LuoОценок пока нет
- DX StdieДокумент22 страницыDX Stdietimie_reyesОценок пока нет
- Paediatric Clinical GuidelinesДокумент7 страницPaediatric Clinical GuidelinesAndriОценок пока нет
- Medications for Pain ManagementДокумент8 страницMedications for Pain ManagementapalestiОценок пока нет
- Status Epilepticus: Kenya Medical Training CollegeДокумент21 страницаStatus Epilepticus: Kenya Medical Training CollegeSalman KhanОценок пока нет
- Generic Name: Albuterol Brand Name: Salbutamol, Proventil, Ventolin, Accuneb, Airet, Novo-SalbutamolДокумент26 страницGeneric Name: Albuterol Brand Name: Salbutamol, Proventil, Ventolin, Accuneb, Airet, Novo-SalbutamolAnna Joy Antone100% (1)
- Anaphylactic Shock Pediatrics: Sarit Levinsky GROUP M1656Документ24 страницыAnaphylactic Shock Pediatrics: Sarit Levinsky GROUP M1656Sarit LevinskyОценок пока нет
- Drug StudyДокумент16 страницDrug StudyJhann0% (1)
- Protocol for managing pesticide poisoningДокумент6 страницProtocol for managing pesticide poisoningJesicca SОценок пока нет
- Scribd 123Документ11 страницScribd 123'Prasada WedatamaОценок пока нет
- Anaphylaxis Acute Management ABCDEДокумент8 страницAnaphylaxis Acute Management ABCDESSОценок пока нет
- 12.0 Emergency Protocol Allergic ReactionsДокумент9 страниц12.0 Emergency Protocol Allergic ReactionsConstantin BudinОценок пока нет
- NOVALGINДокумент4 страницыNOVALGINEkyPratamaОценок пока нет
- ANAPHYLAXIS GUIDELINESДокумент1 страницаANAPHYLAXIS GUIDELINESihtisham1Оценок пока нет
- Drug StudyДокумент14 страницDrug StudyCj LowryОценок пока нет
- Pediatric Emergencies ?-1Документ96 страницPediatric Emergencies ?-1zahraaОценок пока нет
- Management of Anaphylactic Shock: DR Veerendra K H Asst Prof, Dept of MedicineДокумент31 страницаManagement of Anaphylactic Shock: DR Veerendra K H Asst Prof, Dept of MedicineveerendrakhОценок пока нет
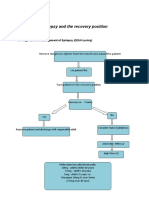
- Epilepsy Recovery Period - Second YrДокумент3 страницыEpilepsy Recovery Period - Second YrBrian MaloneyОценок пока нет
- Drug File SupriyaДокумент36 страницDrug File SupriyaSalim MinjОценок пока нет
- Ascia Hae Action Plan Au 2013Документ1 страницаAscia Hae Action Plan Au 2013kkkssbbОценок пока нет
- Live Vaccines For Adults Following Immunosuppression CA5028 v3Документ8 страницLive Vaccines For Adults Following Immunosuppression CA5028 v3kkkssbbОценок пока нет
- ASCIA HP Penicillin Allergy Guide 2016Документ1 страницаASCIA HP Penicillin Allergy Guide 2016kkkssbbОценок пока нет
- ASCIA HP Clinical Update Food Allergy 2016 HP Version UPDATEDДокумент25 страницASCIA HP Clinical Update Food Allergy 2016 HP Version UPDATEDkkkssbbОценок пока нет
- ASCIA Guidelines Infant Feeding and Allergy PreventionДокумент3 страницыASCIA Guidelines Infant Feeding and Allergy PreventionkkkssbbОценок пока нет
- Poisoning GuidelineДокумент14 страницPoisoning GuidelinekkkssbbОценок пока нет
- ASCIA HP Clinical Update Antibiotic Allergy 2014Документ6 страницASCIA HP Clinical Update Antibiotic Allergy 2014kkkssbbОценок пока нет
- Haematology - Blood Films.Документ6 страницHaematology - Blood Films.kkkssbbОценок пока нет
- RANZCR Annual Report 2015Документ28 страницRANZCR Annual Report 2015kkkssbbОценок пока нет
- Tumbling E ChartДокумент2 страницыTumbling E ChartkkkssbbОценок пока нет
- Apeg Handbook FinalДокумент315 страницApeg Handbook FinalkkkssbbОценок пока нет
- Breastfeeding and The Australian EconomyДокумент22 страницыBreastfeeding and The Australian EconomykkkssbbОценок пока нет
- Fried Rice With Kecap ManisДокумент1 страницаFried Rice With Kecap ManiskkkssbbОценок пока нет
- STRIDORДокумент5 страницSTRIDORkkkssbbОценок пока нет
- Second Year Advanced Fellowship Master Spreadsheet FINAL2 3-6-2015Документ191 страницаSecond Year Advanced Fellowship Master Spreadsheet FINAL2 3-6-2015Gbotemi AlaladeОценок пока нет
- Operative Vaginal Delivery PDFДокумент56 страницOperative Vaginal Delivery PDFFarehan Md IsaОценок пока нет
- Saudi Commission For Health SpecialtiesДокумент35 страницSaudi Commission For Health SpecialtiesDrPrajwal KCОценок пока нет
- Genomics in India - Kapil Khandelwal - EquNev CapitalДокумент5 страницGenomics in India - Kapil Khandelwal - EquNev CapitalKapil KhandelwalОценок пока нет
- Keratinization - Dr. PriyaДокумент37 страницKeratinization - Dr. PriyaDr. Priya Patel75% (4)
- Leslies Resume and Cover LetterДокумент4 страницыLeslies Resume and Cover Letterapi-237845240Оценок пока нет
- Curriculum Vitae: Personal Identification - : Name: Date of Birth Nationality: Gender: Social Situation: ResidencyДокумент3 страницыCurriculum Vitae: Personal Identification - : Name: Date of Birth Nationality: Gender: Social Situation: ResidencyABDEL NASER TAWFIKОценок пока нет
- REVISI 1st Announcement Book 27th ASMIHA 2018 - 12des2017Документ21 страницаREVISI 1st Announcement Book 27th ASMIHA 2018 - 12des2017Jimmy Oi SantosoОценок пока нет
- Procedeul Putti PlatДокумент7 страницProcedeul Putti PlatLoredanaNovacОценок пока нет
- Preface Orofacialpain:Whereweareand Wherewearegoing: Steven D. Bender, Dds EditorДокумент2 страницыPreface Orofacialpain:Whereweareand Wherewearegoing: Steven D. Bender, Dds EditorErick Antonio Castillo GurdianОценок пока нет
- Diseases of The ThyroidДокумент303 страницыDiseases of The ThyroidAtu OanaОценок пока нет
- Instructions For Making The Model of Pelvic Floor MusclesДокумент3 страницыInstructions For Making The Model of Pelvic Floor MusclesCarolynMcIntoshОценок пока нет
- Physical Therapist resume for prestigious rehabilitation setupДокумент2 страницыPhysical Therapist resume for prestigious rehabilitation setupIqra ghafoorОценок пока нет
- Raj TilakДокумент4 страницыRaj TilakObamaОценок пока нет
- AO - CMF Fellowship 0220 LOWДокумент12 страницAO - CMF Fellowship 0220 LOWHarsha VardhanОценок пока нет
- NCHD ApplicationДокумент14 страницNCHD ApplicationIkramullah KhattakОценок пока нет
- Practitioners of Indian Medicine (Standards of Professional Conduct, Etiquette and Code of Ethics) Regulations, 1982Документ9 страницPractitioners of Indian Medicine (Standards of Professional Conduct, Etiquette and Code of Ethics) Regulations, 1982Latest Laws TeamОценок пока нет
- ERAS Personal Statement UCSFДокумент3 страницыERAS Personal Statement UCSFmmkassirОценок пока нет
- The Reproductive System1Документ19 страницThe Reproductive System1Elijah Mae CubaОценок пока нет
- Genetic Disorders Project Rubric 17-18Документ3 страницыGenetic Disorders Project Rubric 17-18api-394564312Оценок пока нет
- Making E.coli Competent and Cloning pUC18Документ2 страницыMaking E.coli Competent and Cloning pUC18Shruti PillaiОценок пока нет