Вам также может понравиться
- Endoscopic Procedures on the SpineОт EverandEndoscopic Procedures on the SpineJin-Sung KimОценок пока нет
- Huang 2017Документ6 страницHuang 2017Lucas HoldereggerОценок пока нет
- Tips and Tricks for Problem Fractures, Volume I: The Upper ExtremityОт EverandTips and Tricks for Problem Fractures, Volume I: The Upper ExtremityDaniel S. HorwitzОценок пока нет
- Anterior Anterolateral Posterior App Advantages DisadvantagesДокумент8 страницAnterior Anterolateral Posterior App Advantages Disadvantagesmuhammad bayu wicaksonoОценок пока нет
- Surgery of the Cranio-Vertebral JunctionОт EverandSurgery of the Cranio-Vertebral JunctionEnrico TessitoreОценок пока нет
- Aaos Elbow Surgical Approaches-1Документ9 страницAaos Elbow Surgical Approaches-1Mossa SultanyОценок пока нет
- Mandibular Surgery Technologic and Technical Improvements - 2014 - Oral and Maxillofacial Surgery Clinics of North AmericaДокумент35 страницMandibular Surgery Technologic and Technical Improvements - 2014 - Oral and Maxillofacial Surgery Clinics of North AmericaGabriela Lizbeth ArmentaОценок пока нет
- InterLaminar Window DescriptionДокумент6 страницInterLaminar Window DescriptionTiger PowerОценок пока нет
- Art:10.1007/s00586 012 2344 6Документ10 страницArt:10.1007/s00586 012 2344 6Dennis ChenОценок пока нет
- Proximal Humerus Fracture Fixation Surgical TechnicДокумент6 страницProximal Humerus Fracture Fixation Surgical TechnicAdhimas WicaksanaОценок пока нет
- Whats New Perctaneuous Pelvis FX Surg ClinOrtNAm20Документ8 страницWhats New Perctaneuous Pelvis FX Surg ClinOrtNAm20Antonio PáezОценок пока нет
- Minimally Invasive Treatment of Displaced Intra-Articular Calcaneal FracturesДокумент14 страницMinimally Invasive Treatment of Displaced Intra-Articular Calcaneal FracturesAnonymous kdBDppigEОценок пока нет
- Ormond 2013Документ12 страницOrmond 2013Hafiz AlfarizieОценок пока нет
- Crawley 2015Документ6 страницCrawley 2015Eduardo HernándezОценок пока нет
- Zimmer MIS Surgical Technique For NexGen CR and LPS Knees (97-5967-002-00 RevДокумент38 страницZimmer MIS Surgical Technique For NexGen CR and LPS Knees (97-5967-002-00 RevNIku ChanОценок пока нет
- Rib FractureДокумент6 страницRib FracturenasyilaputriОценок пока нет
- Inside Out Meniscus Repair 2013 Arthroscopy TechniquesДокумент8 страницInside Out Meniscus Repair 2013 Arthroscopy TechniqueschinthakawijedasaОценок пока нет
- Successful Outcome With Minimally Invasive Plate Osteosynthesis For Periprosthetic Tibial Fracture After Total Knee ArthroplastyДокумент6 страницSuccessful Outcome With Minimally Invasive Plate Osteosynthesis For Periprosthetic Tibial Fracture After Total Knee ArthroplastyMohebОценок пока нет
- Surgical Approaches For Tibial Plateau Fractures: Utku Kandemir, MD Jeffrey Maclean, MS, MDДокумент9 страницSurgical Approaches For Tibial Plateau Fractures: Utku Kandemir, MD Jeffrey Maclean, MS, MDGustavoBecerraОценок пока нет
- Posterior Approaches To The Tibial PlateauДокумент5 страницPosterior Approaches To The Tibial Plateauana starcevicОценок пока нет
- Pi Is 1043181008000225Документ5 страницPi Is 1043181008000225drbhaskar128Оценок пока нет
- Sebastian Ruetten, MD, PHD, Martin Komp, MD, PHD, and Georgios Godolias, MD, ProfДокумент9 страницSebastian Ruetten, MD, PHD, Martin Komp, MD, PHD, and Georgios Godolias, MD, ProfKaustubh KeskarОценок пока нет
- +++kellman-Biomekanik MF TraumaДокумент29 страниц+++kellman-Biomekanik MF TraumamedicamedicaОценок пока нет
- Ruetten 2008Документ9 страницRuetten 2008Creator DocОценок пока нет
- Cephalomedullary Nailing of Pertrochanteric Femur Fractures Using A Large Distractor and Standard Radiolucent TableДокумент4 страницыCephalomedullary Nailing of Pertrochanteric Femur Fractures Using A Large Distractor and Standard Radiolucent Tabledrbane123Оценок пока нет
- CME Trunk, Abdomen, and Pressure Sore ReconstructionДокумент15 страницCME Trunk, Abdomen, and Pressure Sore ReconstructionVeronica TomaselloОценок пока нет
- Management of Complex Orbital Fractures: Article in PressДокумент5 страницManagement of Complex Orbital Fractures: Article in Pressstoia_sebiОценок пока нет
- 1 s2.0 S1877056812001089 MainДокумент6 страниц1 s2.0 S1877056812001089 Mainjmhinos4833Оценок пока нет
- Artigo ClamshellДокумент15 страницArtigo ClamshellbritocirurgiadamaoОценок пока нет
- Transition To Anterior Approach in Primary Total Hip Arthroplasty Learning Curve ComplicationsДокумент7 страницTransition To Anterior Approach in Primary Total Hip Arthroplasty Learning Curve ComplicationsAthenaeum Scientific PublishersОценок пока нет
- Flexible 3D Laparoscopic Assisted Reduction andДокумент9 страницFlexible 3D Laparoscopic Assisted Reduction andgevowo3277Оценок пока нет
- CHAPTER 19 - Mini Open Rota - 2008 - Surgical Techniques of The Shoulder ElbowДокумент7 страницCHAPTER 19 - Mini Open Rota - 2008 - Surgical Techniques of The Shoulder ElbowJaime Vázquez ZárateОценок пока нет
- Abordagem Lateral ExtracavitáriaДокумент9 страницAbordagem Lateral ExtracavitáriaMarcelo MudoОценок пока нет
- Stacey 2016Документ9 страницStacey 2016Hamoud AlhaidariОценок пока нет
- Surgical Tips Tricks On Minimally Invasive.6Документ5 страницSurgical Tips Tricks On Minimally Invasive.6orthogupta923Оценок пока нет
- Muscle-Splitting Posterolateral Thoracotomy: A Novel TechniqueДокумент5 страницMuscle-Splitting Posterolateral Thoracotomy: A Novel TechniqueRizky Angga PОценок пока нет
- 17 - Distal Radius FracturesДокумент78 страниц17 - Distal Radius FracturesFlorin PanduruОценок пока нет
- PM 070 E0Документ23 страницыPM 070 E0Radu HarliscaОценок пока нет
- rayДокумент14 страницraypascallindaОценок пока нет
- Distal Humeral Fractures-Current Concepts PDFДокумент11 страницDistal Humeral Fractures-Current Concepts PDFRina AlvionitaОценок пока нет
- Latissimus Dorsi Tendon Transfer For Massive, Irreparable Posterosuperior Rotator Cuff Tears: Surgical TechniqueДокумент6 страницLatissimus Dorsi Tendon Transfer For Massive, Irreparable Posterosuperior Rotator Cuff Tears: Surgical TechniquemichellmariottiОценок пока нет
- Completely thoracoscopic surgical stabilizationДокумент9 страницCompletely thoracoscopic surgical stabilizationduke3443Оценок пока нет
- 10 11607@jomi 8122Документ8 страниц10 11607@jomi 8122Marlene Kasumi Gantier TakanoОценок пока нет
- Daes 2016Документ2 страницыDaes 2016pancholin_9Оценок пока нет
- Gibson Et Al-2012-Transforaminal Endoscopic Spinal SurgeryДокумент7 страницGibson Et Al-2012-Transforaminal Endoscopic Spinal SurgeryjuanguapoОценок пока нет
- The Lumbar MicrodiscectomyДокумент5 страницThe Lumbar Microdiscectomyokta fianОценок пока нет
- Minimally Invasive Transforaminal Lumbar Interbody Fusion (MI-TLIF) - A Review of Indications, Technique, Results and Complications - PMCДокумент15 страницMinimally Invasive Transforaminal Lumbar Interbody Fusion (MI-TLIF) - A Review of Indications, Technique, Results and Complications - PMCchhabraanОценок пока нет
- Transversus Abdominis Release As An AlternativeДокумент2 страницыTransversus Abdominis Release As An AlternativeLuiz ViannaОценок пока нет
- Intramedullary Headless Screw Fixation For Metacarpal FracturesДокумент7 страницIntramedullary Headless Screw Fixation For Metacarpal FracturesErlin EsauОценок пока нет
- Clinical Analysis of The Frosch Approach in The Treatment of Posterolateral Tibial Plateau Fractures Combined With Lateral Tibial Plateau FracturesДокумент11 страницClinical Analysis of The Frosch Approach in The Treatment of Posterolateral Tibial Plateau Fractures Combined With Lateral Tibial Plateau FracturesraynaldidjohariofcОценок пока нет
- Jaw Surgery: Robert M. Menard, Nikhil K. DesaiДокумент10 страницJaw Surgery: Robert M. Menard, Nikhil K. DesaiAlain AguirreОценок пока нет
- Locking Plate Fixation of Three-And Four-Part Proximal Humeral FracturesДокумент8 страницLocking Plate Fixation of Three-And Four-Part Proximal Humeral FracturesrezaaamuhammadОценок пока нет
- (123doc) Opthalmic Microsurgical Suturing Techniques Part 9Документ15 страниц(123doc) Opthalmic Microsurgical Suturing Techniques Part 9TEODORA MIHAELA PELEASAОценок пока нет
- Total Hip IrrДокумент14 страницTotal Hip IrrHamish JugrooОценок пока нет
- Temporary External Fixation For The Management of Complex Intra - and Periarticular Fractures of The Lower ExtremityДокумент8 страницTemporary External Fixation For The Management of Complex Intra - and Periarticular Fractures of The Lower ExtremityLuigi Paolo Zapata DelgadoОценок пока нет
- Boyd Approach To ElbowДокумент4 страницыBoyd Approach To ElbowGiulio PriftiОценок пока нет
- Kanabur2017nail and Locking Plate For Periprosthetic FracturesДокумент7 страницKanabur2017nail and Locking Plate For Periprosthetic FracturesLenin EstrellaОценок пока нет
- Below Knee AmputationДокумент8 страницBelow Knee AmputationJohan harjono100% (3)
- Fronto-Orbital Advancement Using An en Bloc Frontal Bone CraniectomyДокумент7 страницFronto-Orbital Advancement Using An en Bloc Frontal Bone Craniectomyandredwijaya8Оценок пока нет
- Wolff 2019Документ7 страницWolff 2019Christopher BermeoОценок пока нет
- LWBK836 Ch147 p1581-1583Документ3 страницыLWBK836 Ch147 p1581-1583metasoniko81Оценок пока нет
- LWBK836 Ch140 p1511-1519Документ9 страницLWBK836 Ch140 p1511-1519metasoniko81Оценок пока нет
- Intradural, Extramedullary Spinal Tumors: BackgroundДокумент9 страницIntradural, Extramedullary Spinal Tumors: Backgroundmetasoniko81Оценок пока нет
- LWBK836 Ch146 p1575-1580Документ6 страницLWBK836 Ch146 p1575-1580metasoniko81Оценок пока нет
- LWBK836 Ch135 p1460-1473Документ14 страницLWBK836 Ch135 p1460-1473metasoniko81Оценок пока нет
- Intramedullary Spinal Cord Tumors: Clinical PresentationДокумент15 страницIntramedullary Spinal Cord Tumors: Clinical Presentationmetasoniko81Оценок пока нет
- LWBK836 Ch154 p1633-1648Документ16 страницLWBK836 Ch154 p1633-1648metasoniko81Оценок пока нет
- LWBK836 Ch152 p1617-1621Документ5 страницLWBK836 Ch152 p1617-1621metasoniko81Оценок пока нет
- LWBK836 Ch150 p1598-1607Документ10 страницLWBK836 Ch150 p1598-1607metasoniko81Оценок пока нет
- LWBK836 Ch137 p1485-1486Документ2 страницыLWBK836 Ch137 p1485-1486metasoniko81Оценок пока нет
- LWBK836 Ch148 p1584-1590Документ7 страницLWBK836 Ch148 p1584-1590metasoniko81Оценок пока нет
- LWBK836 Ch144 p1553-1559Документ7 страницLWBK836 Ch144 p1553-1559metasoniko81Оценок пока нет
- LWBK836 Ch151 p1608-1616Документ9 страницLWBK836 Ch151 p1608-1616metasoniko81Оценок пока нет
- LWBK836 Ch06 p65-73Документ9 страницLWBK836 Ch06 p65-73metasoniko81Оценок пока нет
- Spinal Vascular Malformations: Michelle J. Clarke William E. Krauss Mark A. PichelmannДокумент9 страницSpinal Vascular Malformations: Michelle J. Clarke William E. Krauss Mark A. Pichelmannmetasoniko81Оценок пока нет
- Primary Malignant Tumors of The Spine: Gregory S. Mcloughlin Daniel M. Sciubba Jean-Paul WolinskyДокумент12 страницPrimary Malignant Tumors of The Spine: Gregory S. Mcloughlin Daniel M. Sciubba Jean-Paul Wolinskymetasoniko81Оценок пока нет
- Anterior Decompression Techniques For Thoracic and Lumbar FracturesДокумент10 страницAnterior Decompression Techniques For Thoracic and Lumbar Fracturesmetasoniko81Оценок пока нет
- LWBK836 Ch138 p1487-1498Документ12 страницLWBK836 Ch138 p1487-1498metasoniko81Оценок пока нет
- LWBK836 Ch129 p1390-1398Документ9 страницLWBK836 Ch129 p1390-1398metasoniko81Оценок пока нет
- LWBK836 Ch130 p1399-1410Документ12 страницLWBK836 Ch130 p1399-1410metasoniko81Оценок пока нет
- Postlaminectomy Deformities in The Thoracic and Lumbar SpineДокумент6 страницPostlaminectomy Deformities in The Thoracic and Lumbar Spinemetasoniko81Оценок пока нет
- LWBK836 Ch136 p1474-1484Документ11 страницLWBK836 Ch136 p1474-1484metasoniko81Оценок пока нет
- LWBK836 Ch131 p1411-1423Документ13 страницLWBK836 Ch131 p1411-1423metasoniko81Оценок пока нет
- LWBK836 Ch134 p1449-1459Документ11 страницLWBK836 Ch134 p1449-1459metasoniko81Оценок пока нет
- LWBK836 Ch126 p1355-1376Документ22 страницыLWBK836 Ch126 p1355-1376metasoniko81Оценок пока нет
- LWBK836 Ch128 p1381-1389Документ9 страницLWBK836 Ch128 p1381-1389metasoniko81Оценок пока нет
- Bone Grafting and Spine FusionДокумент8 страницBone Grafting and Spine Fusionmetasoniko81Оценок пока нет
- LWBK836 Ch127 p1377-1380Документ4 страницыLWBK836 Ch127 p1377-1380metasoniko81Оценок пока нет
- LWBK836 Ch125 p1345-1354Документ10 страницLWBK836 Ch125 p1345-1354metasoniko81Оценок пока нет
- LWBK836 Ch132 p1424-1438Документ15 страницLWBK836 Ch132 p1424-1438metasoniko81Оценок пока нет
- ORTHOPAEDICS TRAUMAДокумент33 страницыORTHOPAEDICS TRAUMARhomizal MazaliОценок пока нет
- EBM Research DesignДокумент107 страницEBM Research DesignAdhika WijayantiОценок пока нет
- Wiley Milbank Memorial FundДокумент22 страницыWiley Milbank Memorial FundRob21aОценок пока нет
- Meningitis Beyond Neonatal AgeДокумент57 страницMeningitis Beyond Neonatal AgeTilahun Kegne100% (2)
- Hydrocephalus UpdatesДокумент65 страницHydrocephalus Updatescddinchimm100% (1)
- Psych 10Документ10 страницPsych 10karenkaren09Оценок пока нет
- Cholera El TorДокумент16 страницCholera El Torisabelleilagan0% (1)
- How (Not What) To Prescribe Nonpharmacologic Aspects of Psychopharmacology 2012Документ21 страницаHow (Not What) To Prescribe Nonpharmacologic Aspects of Psychopharmacology 2012Wal AlbuquerqueОценок пока нет
- Kokinakos Chris ResumeДокумент1 страницаKokinakos Chris Resumeapi-375717994Оценок пока нет
- Differentiating Physiologic vs Pathologic Jaundice in NewbornsДокумент2 страницыDifferentiating Physiologic vs Pathologic Jaundice in Newbornscheem_porkeezОценок пока нет
- Digital Universe Healthcare Vertical Report ArДокумент16 страницDigital Universe Healthcare Vertical Report ArAmrОценок пока нет
- Ross Case Book 2016Документ305 страницRoss Case Book 2016S86% (7)
- Group 7Документ49 страницGroup 7Muhammad Masoom AkhtarОценок пока нет
- PericarditisДокумент11 страницPericarditisrbarcellonaОценок пока нет
- Insturments & Techniques of Local AnaesthesiaДокумент47 страницInsturments & Techniques of Local AnaesthesiaRohan GroverОценок пока нет
- Nursing Care Plan for a Client with Acute Gouty ArthritisДокумент4 страницыNursing Care Plan for a Client with Acute Gouty ArthritisTikTok TrendzОценок пока нет
- Week 1 MCQ VMPFДокумент25 страницWeek 1 MCQ VMPFZainab_Wajih_2544100% (1)
- ICU-Acquired Weakness and Recovery From Critical IllnessДокумент9 страницICU-Acquired Weakness and Recovery From Critical IllnessFebrian ParuraОценок пока нет
- Krohn Vs CA G.R. No. 108854Документ2 страницыKrohn Vs CA G.R. No. 108854Francise Mae Montilla MordenoОценок пока нет
- Agen HematinikДокумент77 страницAgen HematinikErinaGeraldiОценок пока нет
- NFDN 2007 Assignment 2Документ7 страницNFDN 2007 Assignment 2api-287705803100% (2)
- Exodus SMLXL Rem KoolhaasДокумент11 страницExodus SMLXL Rem Koolhaasjako60Оценок пока нет
- 8 Emergency Formative Clinical Evaluation ChecklistДокумент1 страница8 Emergency Formative Clinical Evaluation Checklistمهند الرحيليОценок пока нет
- HypothyroidismДокумент2 страницыHypothyroidismDanteAndreiОценок пока нет
- Breast LumpsДокумент77 страницBreast LumpsAliyah Tofani PawelloiОценок пока нет
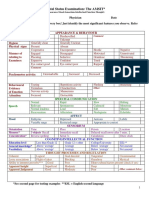
- Mental Status Examination: The AMSIT : Neat and Tidy DisshevelledДокумент2 страницыMental Status Examination: The AMSIT : Neat and Tidy Disshevellednisreen100% (1)
- TW Case StudyДокумент27 страницTW Case Studyapi-346311171Оценок пока нет
- Early Enteral NutritionДокумент55 страницEarly Enteral NutritionAdya ArradikhaОценок пока нет
- Nurs FPX 4020 Assessment 2 Root Cause Analysis and Safety Improvement PlanДокумент5 страницNurs FPX 4020 Assessment 2 Root Cause Analysis and Safety Improvement PlanEmma WatsonОценок пока нет
- Psychiatry IntroductionДокумент26 страницPsychiatry IntroductionMunir AhmedОценок пока нет
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionОт EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionРейтинг: 4 из 5 звезд4/5 (402)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingОт EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingРейтинг: 5 из 5 звезд5/5 (4)
- The Age of Magical Overthinking: Notes on Modern IrrationalityОт EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityРейтинг: 4 из 5 звезд4/5 (13)
- The Happiness Trap: How to Stop Struggling and Start LivingОт EverandThe Happiness Trap: How to Stop Struggling and Start LivingРейтинг: 4 из 5 звезд4/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeОт EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeОценок пока нет
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsОт EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsРейтинг: 3.5 из 5 звезд3.5/5 (3)
- The Obesity Code: Unlocking the Secrets of Weight LossОт EverandThe Obesity Code: Unlocking the Secrets of Weight LossРейтинг: 5 из 5 звезд5/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedОт EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedРейтинг: 5 из 5 звезд5/5 (78)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisОт EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisРейтинг: 4 из 5 звезд4/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityОт EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityРейтинг: 3.5 из 5 звезд3.5/5 (2)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsОт EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsОценок пока нет
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsОт EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsРейтинг: 4.5 из 5 звезд4.5/5 (169)
- The Ultimate Guide To Memory Improvement TechniquesОт EverandThe Ultimate Guide To Memory Improvement TechniquesРейтинг: 5 из 5 звезд5/5 (34)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsОт EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsОценок пока нет
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingОт EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingРейтинг: 3.5 из 5 звезд3.5/5 (31)
- Techniques Exercises And Tricks For Memory ImprovementОт EverandTechniques Exercises And Tricks For Memory ImprovementРейтинг: 4.5 из 5 звезд4.5/5 (40)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisОт EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisРейтинг: 5 из 5 звезд5/5 (3)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.От EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Рейтинг: 4.5 из 5 звезд4.5/5 (110)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaОт EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeОт EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeРейтинг: 4.5 из 5 звезд4.5/5 (253)
- Secure Love: Create a Relationship That Lasts a LifetimeОт EverandSecure Love: Create a Relationship That Lasts a LifetimeРейтинг: 5 из 5 звезд5/5 (16)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessОт EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessРейтинг: 4.5 из 5 звезд4.5/5 (327)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryОт EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryРейтинг: 4 из 5 звезд4/5 (44)