Академический Документы
Профессиональный Документы
Культура Документы
Movilizacion PDF
Загружено:
Laura Camila ChavarroОригинальное название
Авторское право
Доступные форматы
Поделиться этим документом
Поделиться или встроить документ
Этот документ был вам полезен?
Это неприемлемый материал?
Пожаловаться на этот документАвторское право:
Доступные форматы
Movilizacion PDF
Загружено:
Laura Camila ChavarroАвторское право:
Доступные форматы
Early intensive care unit mobility therapy in the treatment of
acute respiratory failure*
Peter E. Morris, MD; Amanda Goad, RN; Clifton Thompson, RN; Karen Taylor, MPT; Bethany Harry, MPT;
Leah Passmore, MS; Amelia Ross, RN, MSN; Laura Anderson; Shirley Baker; Mary Sanchez;
Lauretta Penley; April Howard, RN; Luz Dixon, RN; Susan Leach, RN; Ronald Small, MBA;
R. Duncan Hite, MD; Edward Haponik, MD
Objective: Immobilization and subsequent weakness are conse- patients were out of bed earlier (5 vs. 11 days, p < .001), had
quences of critical illness. Despite the theoretical advantages of therapy initiated more frequently in the intensive care unit (91%
physical therapy to address this problem, it has not been shown that vs. 13%, p < .001), and had similar low complication rates
physical therapy initiated in the intensive care unit offers benefit. compared with Usual Care. For Protocol patients, intensive care
Design and Setting: Prospective cohort study in a university unit length of stay was 5.5 vs. 6.9 days for Usual Care (p .025);
medical intensive care unit that assessed whether a mobility hospital length of stay for Protocol patients was 11.2 vs. 14.5 days
protocol increased the proportion of intensive care unit patients for Usual Care (p .006) (intensive care unit/hospital length of
receiving physical therapy vs. usual care. stay adjusted for body mass index, Acute Physiology and Chronic
Patients: Medical intensive care unit patients with acute re- Health Evaluation II, vasopressor). There were no untoward events
spiratory failure requiring mechanical ventilation on admission: during an intensive care unit Mobility session and no cost differ-
Protocol, n 165; Usual Care, n 165. ence (survivors nonsurvivors) between the two arms, including
Interventions: An intensive care unit Mobility Team (critical Mobility Team costs.
care nurse, nursing assistant, physical therapist) initiated the Conclusions: A Mobility Team using a mobility protocol initi-
protocol within 48 hrs of mechanical ventilation. ated earlier physical therapy that was feasible, safe, did not
Measurements and Main Results: The primary outcome was increase costs, and was associated with decreased intensive care
the proportion of patients receiving physical therapy in patients unit and hospital length of stay in survivors who received physical
surviving to hospital discharge. Baseline characteristics were therapy during intensive care unit treatment compared with patients
similar between groups. Outcome data are reflective of survivors. who received usual care. (Crit Care Med 2008; 36:2238 2243)
More Protocol patients received at least one physical therapy KEY WORDS: respiratory failure; mechanical ventilation; mobility;
session than did Usual Care (80% vs. 47%, p < .001). Protocol intensive care units; physical therapy; passive range of motion
I mmobility, deconditioning, and hospitalization (1, 2). Although physical variability in the delivery of physical ther-
weakness are common problems therapy has a theoretical appeal and may apy to ICU patients may be the lack of a
in mechanically ventilated pa- address this problem, it has not been de- uniform protocolized approach for ICU
tients with acute respiratory fail- termined whether physical therapy has delivery of physical therapy. Such proto-
ure, and may contribute to prolonged increased benefit when initiated early cols exists for other ICU interventions:
during intensive care unit (ICU) treat- weaning from mechanical ventilation,
ment. There may be perceived barriers to liberation from sedation, and early goal
*See also p. 2444. the consistent delivery of passive range of directed therapies for severe sepsis (79).
From the Section on Pulmonary, Critical Care,
Allergy and Immunologic Diseases (PEM, AH, RDH, EH), motion (PROM) and physical therapy in To our knowledge there are no previous
and Public Health Sciences (Le.P), Wake Forest Uni- many ICUs, namely concern over appara- studies that assess efficacy, cost, or hos-
versity School of Medicine, Winston Salem, NC; De- tus dislodgment, integration of mobility pital or long-term benefits of early ICU
partments of Nursing, Physical Therapy, and Hospital with sedation needs, costs of physical Mobility therapy in medical ICU patients.
Administration (AG, CT, KT, BH, AR, LA, SB, MS, La.P,
LD, SL, RS), North Carolina Baptist Hospital, Winston therapists in ICUs and time restraints of As part of a quality improvement project
Salem, NC. both nurses and physical therapists (3). we developed a standard physical therapy
Supported, in part, by The North Carolina Baptist Although exercise has been shown to im- protocol for use in medical ICU patients.
Hospital and The Claude D. Pepper Older Americans
Independence Center of Wake Forest University, NIH
prove functional outcome in emphysema In our ICUs physical therapy is part of
Grant P60AG10484. and heart failure in the outpatient set- usual care; however, delivery and admin-
The authors have not disclosed any potential con- ting, few data exist regarding whether istration of physical therapy is often in-
flicts of interest. early mobility of the medical ICU patient frequent and occurs irregularly. The mo-
For information regarding this article, E-mail:
pemorris@wfubmc.edu will improve outcomes (4, 5). bility protocol was designed to provide a
Copyright 2008 by the Society of Critical Care Physical therapy practice in the ICU mechanism (i.e., the protocol and Mobil-
Medicine and Lippincott Williams & Wilkins setting varies greatly from one setting to ity Team) for standard and frequent (once
DOI: 10.1097/CCM.0b013e318180b90e another (6). One reason for the observed every day) administration of physical
2238 Crit Care Med 2008 Vol. 36, No. 8
therapy to acute respiratory failure pa- experimental movement procedures were in- line assessments included medical history, di-
tients. troduced. This study had Wake Forest Univer- agnosis, BMI, and Acute Physiology and
The purpose of this study was to assess sity Health Sciences Institutional Review Chronic Health Evaluation (APACHE II) score
the frequency of physical therapy, site of Board approval and informed consent was (11). Data were also collected for arterial cath-
waived. eters, central vascular access devices, insulin,
initiation of physical therapy, and patient
Participants were assigned to receive the steroids, and neuromuscular blocking agents.
outcomes comparing respiratory failure mobility protocol by unit using a block allo- The rates of ventilator-associated pneumonia,
patients who received usual care com- cation design. The MICU physician service ad- reintubation, pulmonary embolism, and deep
pared with patients who received physical mitted patients to seven separate ICU units vein thrombosis were recorded. Ventilator-
therapy from a Mobility Team using the based on bed availability. The Mobility Team associated pneumonia was determined by In-
mobility protocol. rotated among the ICUs (set order) until 50 fection Control nursing staff using Centers for
patients per arm had been enrolled in a block, Disease Control guidelines (12). Project out-
MATERIALS AND METHODS (but completed treatment on enrolled pa- come data included the number of ventilator
tients) and then the Mobility Team rotated to days, days until first episode out of bed, ICU
Study Population. Patients were identified the next block of patients. Units were assigned and hospital length of stay (LOS). A ventilator
prospectively and enrolled in the study within to the intervention and control groups in each day was defined as any portion of a calendar
48 hrs of intubation and 72 hrs of admission to block to maintain the balance of enrollment day in which the patient required a ventilator.
the Medical Intensive Care Unit (MICU). Study over time. A total of three blocks were used The first day out of bed was defined as when a
inclusion criteria were age 18 yrs and me- over the course of the study, with each unit patients foot first touched the floor.
chanically ventilated via an endotracheal tube. assigned to both intervention and control Protocol Implementation. The Mobility
Exclusion criteria were inability to walk with- groups at different points in time. Patients in protocol was administered to the Protocol
out assistance before acute ICU illness (use of the other ICUs, without the Mobility Team, group 7 days per week exclusively by the Mo-
a cane or walkers were not exclusions), cogni- were also enrolled in the study but received bility Team (critical care nurse, nursing assis-
tive impairment before acute ICU illness (non- usual physical therapy care (e.g., Usual Care tant, and physical therapist). The Mobility
verbal), preadmission immunocompromised group). Thus, eligible patients were designated Team nurse had no direct bedside nursing
status (prednisone 20 mg/d for 2 wks), neu- to either the Protocol or Usual Care group, care responsibilities. The registered nurses
romuscular disease that could impair weaning based on whether or not they were in one of role was to assess patients on admission to
(myasthenia gravis, amyotrophic lateral scle- the ICUs where the Mobility Team was as- determine entry criteria, to evaluate patients
rosis, Guillian-Barre), acute stroke, body mass signed. Protocol patients received mobility for readiness to interact with the Mobility
index (BMI) 45, hip fracture, unstable cervi- therapy until transferred to a regular hospital Team and to facilitate safety. In the Protocol
cal spine or pathologic fracture, mechanical bed. All patients were managed using proto- group, physical therapy was initiated by the
ventilation 48 hrs before transfer from an cols for sepsis resuscitation, intravenous insu- protocols automatic physicians order;
outside facility, current hospitalization or lin for glycemic control, sedation with daily whereas, in the Usual Care group, physical
transferring hospital stay 72 hrs, cardiopul- interruption, and liberation from mechanical therapy was initiated based on a physicians
monary resuscitation at admission, do not re- ventilation (710). The Mobility Teams repre- patient-specific order.
suscitate at admission, hospitalization within sentation was that across the seven ICUs to The protocol contained four levels of activ-
30 days before admission, cancer therapy which a medicine service patient could be ad- ity therapy (Fig. 1). When patients were un-
within last 6 months, readmission to ICU mitted, there was a 1:1 coverage of Mobility conscious, only PROM therapy was adminis-
within current hospitalization. The reason Team coverage of Protocol beds to Usual tered three times a day to all upper and lower
represented in the listing of immunocompro- Care beds. extremity joints by the Mobility Team nursing
mised as an exclusion was because of the po- All patients were MICU service patients; assistant (level I of the protocol) (Fig. 1). At a
tential difficulty in assessing muscle strength there were no surgical or trauma admissions minimum, five repetitions of PROM were pro-
in patients on long-term corticosteroids. to the project. The MICU service is not geo- vided for each joint. For the upper extremities
It was determined a priori that only pa- graphically limited to just one unit in our PROM included finger flexion and extension;
tients who survived to a hospital discharge hospital but has patients every day in each of wrist flexion, extension, and ulnar and radial
would be included in the outcome analyses the seven units. Patients are assigned beds on deviation; elbow flexion, extension, supina-
based on results of prestudy data that found a first come, first serve basis. The ICU beds tion, and pronation; shoulder flexion, abduc-
few patients who died in the ICU achieved stay 95% occupied. Each of the seven units tion, and internal and external rotation.
sufficient wakefulness to be considered for accepted medical and surgical patients. Each Shoulder extension was deferred due to posi-
physical therapy before their death. Thus, out- of the ICUs had 11 beds except one unit that tioning in bed. Lower extremity PROM in-
come data were compared for patients in the had nine beds. The medical patients were cluded toe flexion and extension; ankle dorsi-
Usual Care group with patients in the Protocol managed with the same general care protocols flexion, plantarflexion, inversion, and
group who survived to hospital discharge. A and physician staff (MICU attendings, fellows eversion; knee flexion and extension; and hip
sample size of 135 survivors per group pro- and house staff) no matter which of the seven flexion, abduction, adduction, internal and ex-
vided 80% power to detect a difference in the ICUs they were assigned. All of the ICUs had a ternal rotation. Hip extension was generally
percent of patients receiving physical therapy 1:2 nurse-to-patient ratio, and one respiratory deferred due to positioning in bed.
of at least 20% between groups, using a two therapist per unit, 24 hrs per day. Nursing At level II of the protocol, physical therapy
sided test and a 5% significance level. staff, protocols, and respiratory therapists was initiated. The patients ability to interact
Protocol Development. As part of a quality were similar across the study time. Also, the with the physical therapist was determined by
improvement initiative to improve patient same set of medical service physicians would the responses to the following commands:
outcome, a mobility protocol was designed to care for all of the patients on the medical Open (close) your eyes, Look at me, Open
initiate and deliver daily mobility therapy to service, concurrently, whether they were on your mouth and put out your tongue, Nod
MICU patients. The protocol was developed the protocol arm or usual care arm, no matter your head, and Raise your eyebrows when I
with involvement of nursing, physical therapy, to which unit the patient was admitted. have counted up to 5 (2). The patient had to
and intensivists. All care delivered under this Demographic information, mortality, base- respond correctly to three of the five com-
protocol was already governed by the hospi- line assessments, on-project management in- mands to be considered sufficiently alert to
tals Nursing and Physical Therapy Depart- formation, physical therapy administration, participate in physical therapy. Patients were
ments policies and procedures, i.e., no new and hospital outcomes were collected. Base- progressed to active-assistive and active range
Crit Care Med 2008 Vol. 36, No. 8 2239
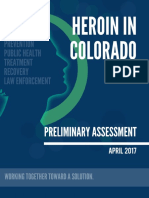
Figure 2. An orally intubated level intravenous
patient, exercising while standing.
deviations for continuous measures and
counts and percentages for categorical mea-
Figure 1. Passive range of motion therapy (PROM) started on day 1 of Protocol (level I). As patients
sures. All statistical tests were two-sided and
demonstrated consciousness and increased strength (see circles with arrows above), they were moved
significance was determined at the .05 proba-
to the next higher level. Physical therapy (PT) would be first attempted at level II. The Protocols
bility level. Days to first out of bed, ventilator
intervention ceased as a patient was transferred to a floor bed and then the patient within both
days, and ICU and hospital LOS data were log
Protocol and Usual Care groups would receive usual care mobility therapy (MT) as dictated by the
floor physician teams. ICU, intensive care unit; OOB, out of bed.
transformed for statistical analysis. Baseline
data were analyzed reflective of all patients
enrolled in the project (Usual Care group, n
165 vs. Protocol group, n 165). Basic com-
of motion exercise as they were alert and able pressure 65 mm Hg), administration of a
parisons between groups were done with a
to advance their participation, and were ad- new pressor agent, new documented myocar-
Students t-test for continuous variables or
vanced through levels II through IV of the dial infarction by electrocardiogram and en-
chi-square for categorical variables. Project
protocol. Advancement to the next level was zyme changes, dysrhythmia requiring the ad-
outcomes on the outcome population, partic-
based on limb strength during one effort (3/5 dition of a new antiarrhythmic agent, an
ipants who survived to hospital discharge, are
Medical Research Council strength in biceps increase in the positive end-expiratory pres-
for IIIII advance, and 3/5 in quadriceps for sure on the ventilator or a change to assist reported as means (95% confidence intervals).
IIIIV advance). Five repetitions per exercise control mode once in a weaning mode. If mo- Tests of univariate association with the project
were typical goals. Weights were not used as bility was withheld the patients were re- outcomes were done by using simple linear
part of the protocol. As patients progressed, evaluated the next day. If stable, the mobility regression. Univariate predictor variables with
the activity increasingly focused on functional protocol was reinitiated. There was no abso- p .1 were included in the multiple linear
activities such as transfer to edge of bed; safe lute limit in regard to FIO2 and positive end- regression analysis as possible confounders. A
transfers to and from bed, chair, or commode; expiratory pressure to withhold Mobility. stepwise selection procedure was used to iden-
seated balance activities; pregait standing ac- Mobility was not initiated if the patient tify significant variables (p .05) associated
tivities (forward and lateral weight shifting, were deemed to be experiencing frequent de- with the project outcomes.
marching in place); and ambulation (Fig. 2). saturations. Baseline BMI, APACHE II, and vasopressor
The protocols intervention ended when a Usual Care. Nursing practice for the Usual usage (yes/no) were included in the multiple
patient was transferred to a regular bed. Pa- Care group included administration of PROM linear regression as confounders. The differ-
tients in both arms would then receive usual as delivered daily by the bedside nurse; uncon- ence between the Usual Care and Protocol
care. Patient transfer from the MICU to either scious patients were repositioned every 2 hrs. groups in project outcomes was adjusted for
the Intermediate Care Unit or floor nursing The administration of both PROM and Physi- these confounders. The adjusted means are
units was determined by the MICU physician cal Therapy to ventilated, ICU patients is per- the least square means from the linear regres-
team. At the time of assignment to a floor bed, mitted and governed by Nursing and Physical sion models. Both unadjusted and adjusted
MICU patients were transferred to a separate Therapy department policies. means (95% confidence intervals) are reported
physician service that worked primarily with Outcomes. The primary outcome was the for study outcomes.
floor patients (the General Medicine Physician proportion of patients surviving to hospital The effect of ICU unit was assessed by add-
service, Family Practice or Neurology). discharge who received ICU physical therapy. ing ICU unit to the multivariable models as a
The following criteria were used to limit or Secondary outcomes included days until first fixed effect and an interaction term for ICU
withhold mobility interventions including a out of bed, ventilator days, ICU LOS, and hos- and group (protocol/control). Both the ICU
decline in hemodynamic or ventilatory status, pital LOS among survivors. unit term and the interaction term were non-
definitions of hemodynamic or ventilatory de- Statistical Analyses. All statistical analyses significant. The effect of the protocol on LOS
cline were hypoxia with frequent desatura- were performed with SAS version 9. Descrip- outcomes was not different between the ICU
tions below 88%, hypotension (mean arterial tive statistics included means and standard units.
2240 Crit Care Med 2008 Vol. 36, No. 8
RESULTS Table 1. Enrollment population baseline parameters
Patients were enrolled in the study for Usual Care Protocol
Parameter (n 165) (n 165) p
24 consecutive months within 2004 to
2006. There were a total of 3032 patients Diagnoses (no. and %) .915
admitted to the MICU service, of which Acute lung injury: out-patient pneumonia 33 (20.1%) 32 (19.8%)
1605 were not intubated. Of the 1427 Acute lung injury: severe sepsis (nonpneumonia) 23 (14.0%) 26 (16.0%)
intubated admissions, 330 met study cri- Acute lung injury: aspiration pneumonia 32 (19.5%) 27 (16.7%)
teria and were assigned either to the Acute lung injury: pancreatitis 2 (1.2%) 4 (2.5%)
Acute lung injury: other 10 (6.1%) 6 (3.7%)
Usual Care (n 165) or the Protocol Coma 20 (12.2%) 25 (15.4%)
group (n 165) based on block ICU Post-op 4 (2.4%) 7 (4.3%)
allocation. Of the 1097 excluded, the ex- Congestive heart failure 10 (6.1%) 12 (7.4%)
clusions were (some patients had more Cardiac arresta 6 (3.7%) 3 (1.9%)
Acute on chronic lung dz: asthma 4 (2.4%) 4 (2.5%)
than one exclusion) hospital stay 72 hrs Acute on chronic lung dz: chronic obstructive pulmonary 18 (11.0%) 14 (8.6%)
before intubation, 543; nonambulatory, disease
168; cancer therapy, 153; stroke, 120; im- Acute on chronic lung dz: nonasthma/non-chronic obstructive 2 (1.2%) 2 (1.2%)
munocompromised, 59; cardiopulmonary pulmonary disease
resuscitation at admission, 51; cognitive Age in yrs (mean SD ) 55.4 16.8 54.0 16.8 .782
impairment, 46; BMI 45, 42; cervical Gender-male (no. and %) 88 (53.3%) 93 (56.4%) .581
Body mass index (mean SD ) 27.7 7.1 29.0 6.8 .376
spine or hip fracture, 20; DNR at admis- Acute Physiology and Chronic Health Evaluation II 21.6 8.0 23.5 8.8 .092
sion, 2. Activity of daily living 96.5 9.8 95.3 12.6 .243
Baseline Characteristics. Demo- Charlson index 3.16 2.23 2.87 2.31 .249
graphic characteristics, diagnosis infor- Patients on vasopressors (no. and %) 60 (36.4%) 53 (32.1%) .815
Patients with previous home O2 (no. and %) 9 (5.5%) 13 (7.9%) .378
mation, and baseline characteristics are Patients with previous chronic renal failure (no. and %) 9 (5.5%) 9 (5.5%) 1.00
reported in Table 1 for all patients en-
rolled in the project. There were no dif- dz, disease.
ferences in baseline characteristics for a
Patients with cardiac arrest were patients transferred from an outside hospital and entered before
the Usual Care and Protocol groups. subsequent records from the transferring hospital were obtained. These patients were entered without
There were no differences in the pro- knowledge of their exclusion.
portions of patients in both groups re-
ceiving intravenous insulin and intrave- Table 2. Postenrollment variables
nous neuromuscular blocking agents for
1 or more days during their ICU stay. Usual Care Protocol
(n 165) (n 165) p
There was no statistical difference be-
tween the Usual Care and Protocol Patients with arterial catheters (no. and %) 78 (47.3%) 69 (41.8%) .320
groups for the proportion of patients who Number of arterial catheters per patient (mean SD ) 1.3 0.6 1.4 0.7 .557
received intravenous or oral corticoste- Patients with central VAD (no. and %) 100 (60.6%) 91 (55.2%) .316
roids on day 1 of their ICU stay (22.4% of Number of VADs per patient (mean SD ) 2.1 1.6 2.1 1.4 .919
Patients reintubated (no. and %) 28 (17.0%) 28 (17.0%) 1.00
patients vs. 21.8% of patients, respec-
Patients receiving intravenous insulin in ICU (no. and %) 83 (50.3%) 82 (49.7%) .912
tively, p .8955). A simple linear regres- Patients receiving neuromuscular blocking agent 23 (13.9%) 31 (18.8%) .234
sion was done to assess the relationship 1 d (no and %)
between corticosteroid administration Patients receiving steroids in first 24 hrs (no. and %) 37 (22.4%) 36 (21.8%) .895
and study outcomes. No significant rela- Patients with VAP (no. and %) 13 (7.9%) 5 (3.0%) .087
Patients with pulmonary embolism by computed tomography 3 (1.8%) 4 (2.4%) .702
tionships were found (p .05). The pro-
angiogram (no. and %)
portion of patients diagnosed with venti- Patients with deep vein thrombosis by lower 3 (1.8%) 9 (5.4%) .078
lator-associated pneumonia, pulmonary extremity Doppler (no. and %)
emboli, or deep vein thromboses was not Intravenous sedation days per patient (mean SD ) 5.15 6.23 5.54 9.10 .945
statistically different for the Usual Care Discharge location n 135 n 145
groups compared with Protocol group. Long term acute care (no. and %) 10 (7.4%) 10 (6.9%) .868
Process Measures, On-Project Man- Skilled nursing facility (no. and %) 15 (11.1%) 12 (8.3%) .422
Rehabilitation hospital (no. and %) 12 (8.9%) 16 (11.0%) .550
agement, and Safety Characteristics. No Home (no. and %) 98 (72.6%) 107 (73.8%) .821
deaths, near-deaths or cardiopulmonary
resuscitation occurred during physical VAD, vascular access device; VAP, ventilator-associated pneumonia; ICU, intensive care unit.
therapy in either group. There were no
adverse events such as accidental removal
of a device during physical therapy and sure and 0.9% of sessions were not Mortality. In-hospital mortality oc-
no differences in the numbers of arterial initiated because of either too high or too curred in 30 of 165 Usual Care patients
catheters, venous devices or reintuba- low a heart rate. The most frequent rea- (18.2%) and 20 of 165 (12.1%) of Proto-
tions between the two groups (Table 2). son for ending a mobility session was col patients (p 0.125). Of those patients
Of all combined passive and active ses- patient fatigue occurring without a sig- with an in-hospital death, only five had
sions, only 1.4% were not initiated be- nificant change in the patients vital received a physical therapy session (Usual
cause of either a high or low blood pres- signs. Care, n 2; Protocol, n 3).
Crit Care Med 2008 Vol. 36, No. 8 2241
Table 3. Outcomes (survivors) ting, safely increased the proportion of
acute respiratory failure patients who re-
Usual Care Protocol
ceived physical therapy without adverse
(n 135) (n 145) p
events. Our report is similar to previous
Days to first out of bed 13.7 (11.715.7) 8.5 (6.610.5) .001 studies that show ICU mobility is feasible
Days to first out of bed (adjusteda) 11.3 (9.613.4) 5.0 (4.35.9) .001 and safe (14, 15) and extends these pre-
Ventilator days 9.0 (7.510.4) 7.9 (6.49.3) .298 vious reports by documenting that early
Ventilator days (adjusteda) 10.2 (8.711.7) 8.8 (7.410.3) .163 ICU mobility was associated with statisti-
ICU LOS days 8.1 (7.09.3) 7.6 (6.38.8) .084
ICU LOS days (adjusteda) 6.9 (5.98.0) 5.5 (4.76.3) .025
cally significant shortened days in bed,
Hospital LOS days 17.2 (14.220.2) 14.9 (12.617.1) .048 and reduced ICU and hospital LOS for
Hospital LOS days (adjusteda) 14.5 (12.716.7) 11.2 (9.712.8) .006 hospital survivors, without increasing
cost. If this project is replicated, such
Data are presented as means (confidence intervals). data may be important in justifying bud-
Adjusteda, adjusted for body mass index, Acute Physiology and Chronic Health Evaluation II, and getary support for early physical therapy
vasopressors.
in ICU patients.
ICU, intensive care unit; LOS, length of stay.
Although cost was not statistically dif-
ferent between groups, the absolute dif-
Outcomes. In the Usual Care group, There was a significant difference be- ference in cost appears to be less for the
64 of 135 (47.4%) underwent at least one tween the Usual Care and Protocol groups Protocol group, including the cost of the
physical therapy session at any time dur- in both ICU and hospital LOS measures. Mobility Team, likely because of LOS-
ing their hospital stay compared with 116 The adjusted ICU LOS for the Usual Care related cost reductions. Confirmation of
of 145 patients (80.0%) of the Protocol group was 6.9 days vs. the Protocol group these data could be useful to justify the
group (p .001). Of the 64 Usual Care 5.5 days, p .027. The hospital LOS (ad- initiation of such a program to hospital
patients who received physical therapy, justed) was 14.5 days for the Usual Care administrators. Although the relation-
eight (12.5%) patients had physical ther- group (n 135) and 11.2 days for the ship between costs and the Mobility in-
apy initiated during ICU treatment com- Protocol group (n 145) (p .006) (see tervention is an association and not cau-
pared with 106 of 116 Protocol patients Table 3 for unadjusted values of ICU and sation, it may be that early mobility
(91.4%) (p .001). Within the subset of hospital LOS). interventions are cost saving.
patients who received at least one physi- There were no statistical differences in Although the mechanisms of our Pro-
cal therapy session during their hospital discharge locations between groups (spe- tocols reduced ICU and hospital LOS in
stay, Usual Care patients had fewer ses- cifically there was no higher percentage survivors are unclear, several factors may
sions compared with Protocol patients, of Protocol patients who were transferred have influenced the outcome. Protocol-
4.1 sessions per patient vs. 5.5 sessions to Long Term Acute Care hospitals on ization of this care may have served as a
per patient, (p .037). Within the anal- mechanical ventilation vs. the Usual Care significant factor. Previous ICU studies
ysis population, study outcomes are re- group) (Table 2). Time to hospital dis- have shown that protocolized delivery of
ported as unadjusted and adjusted means charge in days for both groups is repre- care by nursing and respiratory therapy
(95% confidence interval). After adjust- sented in Table 3. staff increased the percentage of patients
ing for BMI, APACHE II, and vasopressor Hospital Costs. The total direct inpa- for whom care may be delivered, such as
usage, Usual Care patients were first out tient costs for the Protocol group inclu- daily awakening and weaning (7, 8). An-
of bed in 11.3 days whereas Protocol pa- sive of the Mobility Team salaries were other factor may be that an independent,
tients were first out of bed in 5.0 days $6,805,082 and for the Usual Care group, multidisciplinary team (nursing assis-
(p .001) (Table 3). The proportion of $7,309,871. The average cost per patient tants, nurse and physical therapist) deliv-
Protocol patients who were able to ad- was $44,302 for the Usual Care group and ered the protocol compared with usual
vance to specific levels of the protocol is $41,142 for the Protocol group, p care which relied on a physical therapist
as follows: level I 44 (26.7%), level II 0.262. The cost of the Mobility Team sal- working with the various bedside caregiv-
12 (7.3%), level III 18 (10.9%), level ary and benefits for the study duration ers when available. Additionally, within
IV 91 (55.1%). The average number of (24 months) was $251,258. Usual Care, initiation of physical therapy
days at each level is as follows: level I: was dependent on receipt of the MICU
mean (SD) 7.1 (10.5); level II: mean DISCUSSION teams order; whereas, Mobility com-
(SD) 2.3 (2.0); level III: mean (SD) 2.2 menced for the Protocol group when the
(1.3); level IV: mean (SD) 3.9 (3.5). Although physical deconditioning of patient first met criteria as assessed by
There was no significant difference in ICU patients, possibly most pronounced the Mobility Teams nurse. The Mobility
mean number of ventilator days between in acute respiratory distress syndrome (1, team may have reduced the frequency of
the two groups. Ventilator days (adjusted) 13) has previously been described, there missed opportunities for physical therapy
comparing the Usual Care (n 135) and is a paucity of data describing outcomes sessions as they were freed from other
Protocol (n 145) groups were 10.2 vs. of early mobility therapy. We found that patient care responsibilities. This effect
8.8 days, respectively, p 0.163. In the implementation of an early mobility pro- may be due to more uniform skill level,
Usual Care group, 16 of 165 (9.7%) pa- tocol by a Mobility Team resulted in more the high priority the Mobility Team
tients were readmitted to the ICU physical therapy sessions and impor- placed on physical therapy, or it may
whereas 14 of 165 (8.5%) in the Protocol tantly, was associated with shorter LOS highlight pervasive time constraints for
group were readmitted (p 0.702) for hospital survivors. This study shows the routine bedside caregivers resulting
within the same hospital stay. that a mobility protocol, in the ICU set- in limited time to provide physical ther-
2242 Crit Care Med 2008 Vol. 36, No. 8
apy. That there is limited time a bedside proportion of patients with a higher prob- Emphysema Treatment Trial. Chest 2005;
practitioner might be able to spend on ability of overall survivorship than the 128:3799 3809
mobilization and still achieve other care general medical ICU population. Whether 5. Belardinelli R, Georgiou D, Cianci G, et al:
similar results could be reproduced in Randomized, controlled trial of long-term
goals may have been a factor. A recent
moderate exercise training in chronic heart
nursing survey found that time for direct medical ICU populations with more se-
failure: Effects on functional capacity, quality
patient care declined 6% in a 3-yr period vere diseases, or inclusion after 72 hrs, of life, and clinical outcome. Circulation
from 1999 to 2001 (16). Time required remains unknown. Furthermore, whether 1999; 99:11731182
for charting and care documentation was an early physical therapy program could 6. Norrenberg M, Vincent JL: A profile of Euro-
given the most frequent reason for the be applied to surgical ICU patients (with pean intensive care unit physiotherapists.
decline in direct patient care. postoperative pain and associated analge- European Society of Intensive Care Medi-
Mobility therapy was available more sic requirements) also remains unknown. cine. Intensive Care Med 2000; 26:988 994
frequently in the Protocol group than in The study was not blinded and there- 7. Ely EW, Baker AM, Dunagan DP, et al: Effect
the Usual Care group (7 days compared fore a potential bias is associated with the on the duration of mechanical ventilation of
physicians, nurses, physical therapists, identifying patients capable of breathing
with 5 days a week) which may have con-
spontaneously. N Engl J Med 1996; 335:
tributed to a shorter hospital stay in these and respiratory therapists who cared for
1864 1869
patients. Future targeted dose and dura- patients in both arms of the study. De-
8. Kress JP, Pohlman AS, OConnor MF, et al:
tion studies of the exercise delivered by spite these limitations, this project was Daily interruption of sedative infusions in
an ICU Mobility Team may clarify mech- associated with decreased ICU and hospi- critically ill patients undergoing mechanical
anisms, as major advances in the under- tal LOS in survivors. This is the first ventilation. N Engl J Med 2000; 342:
standing of the physical therapy dose- study to show that early physical therapy 14711477
response relationship in the ambulatory compared with a group receiving Usual 9. Rivers E, Nguyen B, Havstad S, et al: Early
setting have been recently shown (17, Care (with relatively little ICU-based goal-directed therapy in the treatment of se-
18). These types of investigations in the physical therapy) was associated with im- vere sepsis and septic shock. N Engl J Med
portant outcomes in the ICU. Future 2001; 345:1368 1377
ICU may provide further benefit by defin-
studies with in-hospital functional mea- 10. Van den Berghe G, Wouters P, Weekers F, et
ing the upper or lower limitations of ben-
al: Intensive insulin therapy in critically ill
efit of early physical therapy. Finally, fu- surements may provide clarification as to
patients. N Engl J Med 2001; 345:1359 1367
ture ICU investigations may need to the effect of physical therapy on sedation 11. Knaus WA, Draper EA, Wagner DP, et al:
consider the timing of mobility therapy assessments and more importantly on APACHE II: A severity of disease classifica-
as an independent outcome variable how early mobilization may have affected tion system. Crit Care Med 1985; 13:
when assessing survivors ICU-free days long-term functional outcomes. These 818 829
or hospital-free days. results were obtained in the Protocol 12. Horan TC, Gaynes RP: Surveillance of noso-
ICU nursing unit assignment rather group that was compared with a Usual comial infections. In: Hospital Epidemiology
than randomization was used to allocate Care group which received relatively little and Infection Control. Mayhall CG (Ed.).
ICU-based physical therapy. This Usual Philadelphia, Lippincott Williams & Wilkins,
patients to receive the mobility protocol.
Care group may not be representative of 2004, pp 1659 1702
However, patients were enrolled within
13. Schweickert WD, Hall J: ICU-acquired weak-
48 hrs of intubation, there was no drop- the baseline level of physical therapy ad-
ness. Chest 2007; 131:15411549
out or crossover of patients between ministered in other hospitals ICUs.
14. Stiller K, Phillips AC, Lambert P: The safety
groups (i.e., every patient enrolled in the of mobilisation and its effect on haemody-
study is accounted for in the baseline CONCLUSIONS namic and respiratory status of intensive
parameters), and there were no differ- care patients. Physiother Theory Practice
We conclude that mobility therapy de-
ences in the patients baseline character- 2004; 20:175185
livered early in the course of acute respira- 15. Bailey PR, Thomsen GEM, Spuhler VJR, et al:
istics of home oxygen dependence or
tory failure patients receiving mechanical Early activity is feasible and safe in respira-
chronic renal failure. Further, both
ventilation is feasible, safe, did not increase tory failure patients. Critical Care Med 2007;
groups received care directed by a single
cost, and was associated with decreased ICU 35:139 145
physician group, the MICU physicians
and hospital LOS in survivors. 16. Lacey LM, Shaver K: Reductions in the
and sedation, sepsis management, glu- amount of time spent in direct patient care
cose control and ventilator weaning were by staff nurses in North Carolina. North
all controlled by protocol. REFERENCES
Carolina Center for Nursing 2002; Available
A limitation is that the mobility pro- 1. Herridge MS, Cheung AM, Tansey CM, et al: at: http://www.nursenc.org/research/chgs_
tocol was limited in its delivery to within One-year outcomes in survivors of the acute time_alloctn. Accessed September 3, 2007
the ICU setting. It is to be determined if respiratory distress syndrome. N Engl J Med 17. Church TS, Earnest CP, Skinner JS, et al:
similar or more robust results may be 2003; 348:683 693 Effects of different doses of physical activity
achieved if the active intervention were 2. DeJonghe B, Sharshar T, Lefaucheur JP, et on cardiorespiratory fitness among seden-
al: Paresis acquired in the intensive care tary, overweight or obese postmenopausal
carried out through the portion of the
unit: A prospective multicenter study. JAMA women with elevated blood pressure: A ran-
hospital stay when the patients were in
2002; 288:2859 2867 domized controlled trial. JAMA 2007; 297:
the regular floor settings and if patients 3. Morris PE. Moving our critically ill patients: 20812091
with more numerous comorbidities were Mobility barriers and benefits. Crit Care Clin 18. Lee IM: Dose-response relation between
examined. These results were associated 2007; 23:120 physical activity and fitness: Even a little is
with an ICU population specifically re- 4. Ries AL, Make BJ, Lee SM, et al: The effects of good; more is better. JAMA 2007; 297:
stricted by exclusion criteria to select a pulmonary rehabilitation in the National 21372139
Crit Care Med 2008 Vol. 36, No. 8 2243
Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Herpes Opportunity Disclosure Handout 2Документ1 страницаHerpes Opportunity Disclosure Handout 2Thong Huynh100% (1)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Epidemiology - CHEAT SHEETДокумент4 страницыEpidemiology - CHEAT SHEETEthica100% (15)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Microbiology For OptometristsДокумент7 страницMicrobiology For OptometristsMohamed Shantier100% (2)
- PATHOPHYSIOLOGY-PTB - FinalДокумент1 страницаPATHOPHYSIOLOGY-PTB - FinaliamMye100% (1)
- M. Preterm and Postterm - NewДокумент93 страницыM. Preterm and Postterm - NewRinaОценок пока нет
- Chole CystitisДокумент4 страницыChole CystitisMasithaОценок пока нет
- Causes of Blindness and Visual ImpairmentДокумент3 страницыCauses of Blindness and Visual ImpairmentMuhammad Amri KautsarОценок пока нет
- Classification of Primary Headaches: Views & ReviewsДокумент9 страницClassification of Primary Headaches: Views & ReviewsHabib G. Moutran BarrosoОценок пока нет
- AIIMS Question PaperДокумент6 страницAIIMS Question Papersharu4291100% (1)
- MalariaДокумент8 страницMalariasomebody_maОценок пока нет
- Poultry DiseaseДокумент8 страницPoultry DiseaseJoão Silva0% (1)
- Otitis ExternaДокумент14 страницOtitis ExternaRizkaGayoОценок пока нет
- My Safe SpaceДокумент2 страницыMy Safe SpaceGabriel DiuyanОценок пока нет
- Lakshmi V Paed KIMSB 2013Документ155 страницLakshmi V Paed KIMSB 2013Kari RichardsonОценок пока нет
- StrongyloidiasisДокумент5 страницStrongyloidiasisMufidah OthmanОценок пока нет
- Dermatology in Mideaval IndiiaДокумент20 страницDermatology in Mideaval IndiiaMuhamed Ashraf CОценок пока нет
- Epidemiological SurveillanceДокумент22 страницыEpidemiological SurveillanceSyafiq HusniОценок пока нет
- Daftar PustakaДокумент5 страницDaftar PustakaGeraldo Primaman CoffeeОценок пока нет
- What Is DracunculiasisДокумент1 страницаWhat Is DracunculiasisSiti SyahirahОценок пока нет
- Planning A Surveillance SystemДокумент28 страницPlanning A Surveillance SystemRatu TaqiyaОценок пока нет
- Heroin in ColoradoДокумент62 страницыHeroin in ColoradoMichael_Lee_RobertsОценок пока нет
- Microbiology ReviewerДокумент3 страницыMicrobiology ReviewerWendy Escalante100% (6)
- Humasis Malaria Antigen Test: High Sensitive Differential Diagnosis of Malaria InfectionДокумент10 страницHumasis Malaria Antigen Test: High Sensitive Differential Diagnosis of Malaria InfectionSantiagoAFОценок пока нет
- Made By: DR Aditya RanjanДокумент32 страницыMade By: DR Aditya RanjanArjun SainiОценок пока нет
- Test Bank Chapter 23: Nursing Assessment: Integumentary SystemДокумент6 страницTest Bank Chapter 23: Nursing Assessment: Integumentary SystemBriseidaSolisОценок пока нет
- HACCPtestДокумент13 страницHACCPtestDianne Faye ManabatОценок пока нет
- Guidelines For The Use of Fresh-Frozen Plasma, CryoprecipitateДокумент18 страницGuidelines For The Use of Fresh-Frozen Plasma, CryoprecipitatemelaniefarahdillaОценок пока нет
- Vox SanguinisДокумент179 страницVox SanguinistristanmunarОценок пока нет
- History of Present IllnessДокумент2 страницыHistory of Present IllnessReylan GarciaОценок пока нет
- 14th Century - Black DeathДокумент16 страниц14th Century - Black DeathJean-pierre NegreОценок пока нет