Вам также может понравиться
- Prostate International: Cindy Garcia, Peter Chin, Prem Rashid, Henry H. WooДокумент5 страницProstate International: Cindy Garcia, Peter Chin, Prem Rashid, Henry H. WooAkhmad MustafaОценок пока нет
- Percutaneous Nephrostomy: Last Updated: January 3, 2003Документ5 страницPercutaneous Nephrostomy: Last Updated: January 3, 2003Alicia EncinasОценок пока нет
- Transurethral Resection of The ProstateДокумент48 страницTransurethral Resection of The Prostateralf_dolanОценок пока нет
- Benign Prostatic Hyperplasia (BPH) : Jeselo Ouano GormeДокумент60 страницBenign Prostatic Hyperplasia (BPH) : Jeselo Ouano GormeMaddox EdeyajОценок пока нет
- Transurethral Resection of ProstateДокумент10 страницTransurethral Resection of ProstateMa. Ydela MeradoresОценок пока нет
- 2020ICU - Icu 62 569Документ8 страниц2020ICU - Icu 62 569andryzell1987Оценок пока нет
- TURPДокумент25 страницTURPShreevidya GurunageshОценок пока нет
- Ocua Urologytoday VolumeiДокумент8 страницOcua Urologytoday Volumeiapi-249405525Оценок пока нет
- 0616 SCuДокумент18 страниц0616 SCuYolanda Dwi OktaviyaniОценок пока нет
- ProstactomyДокумент18 страницProstactomyBharat BhushanОценок пока нет
- 191 206 PDFДокумент16 страниц191 206 PDFVelix ZeroFifeОценок пока нет
- Post Aua ReconstructivaДокумент14 страницPost Aua ReconstructivaIndhira Sierra SanchezОценок пока нет
- Turp Transurethral Resection of The Prostate: Anatomic and Physiologic OverviewДокумент4 страницыTurp Transurethral Resection of The Prostate: Anatomic and Physiologic OverviewJylme Keziah Manzano DoronioОценок пока нет
- Articol ExtensoДокумент5 страницArticol ExtensoDavid CalinОценок пока нет
- Management of AROUДокумент6 страницManagement of AROUAung Ko HtetОценок пока нет
- PCNL and PyelolithotomyДокумент60 страницPCNL and PyelolithotomyDoctors PodcastОценок пока нет
- Management of Feline Ureteral Obstructions: An Interventionalist's ApproachДокумент6 страницManagement of Feline Ureteral Obstructions: An Interventionalist's ApproachvetgaОценок пока нет
- AO - Trans Obturator Technique Versus Suburethral Tape PDFДокумент15 страницAO - Trans Obturator Technique Versus Suburethral Tape PDFGustavo flores quispeОценок пока нет
- Robotic-Assisted Laparoscopic Radical Cystectomy With Extracorporeal Urinary Diversion: Initial ExperienceДокумент11 страницRobotic-Assisted Laparoscopic Radical Cystectomy With Extracorporeal Urinary Diversion: Initial ExperiencesandyrraoОценок пока нет
- CystorrhaphyДокумент7 страницCystorrhaphyKit LaraОценок пока нет
- Theimpactofprostatesizemedianlobeandpriorbenignprostatichyperplasiainterventiononrobot Assistedlaparoscopicprostatectomy TechniqueandoutcomesДокумент9 страницTheimpactofprostatesizemedianlobeandpriorbenignprostatichyperplasiainterventiononrobot Assistedlaparoscopicprostatectomy TechniqueandoutcomesGordana PuzovicОценок пока нет
- Class Presentation ON BPH: Presented By: Ruchika Kaushal M.Sc. Nursing 1 YearДокумент31 страницаClass Presentation ON BPH: Presented By: Ruchika Kaushal M.Sc. Nursing 1 YearRuchika KaushalОценок пока нет
- Advances in Urinary Tract EndosДокумент23 страницыAdvances in Urinary Tract EndosJosé Moreira Lima NetoОценок пока нет
- Benign Prostatic Hyperplasia (BPH) : By, Ms. Ekta. S. Patel, I Yr M.SC NursingДокумент71 страницаBenign Prostatic Hyperplasia (BPH) : By, Ms. Ekta. S. Patel, I Yr M.SC NursingannisanabilaasОценок пока нет
- Interventional Radiology 1Документ66 страницInterventional Radiology 1sibrahim16Оценок пока нет
- FP & NC Kidney SurgeryДокумент48 страницFP & NC Kidney SurgeryancoursОценок пока нет
- An Update On Transurethral Surgery For Benign Prostatic ObstructionДокумент4 страницыAn Update On Transurethral Surgery For Benign Prostatic ObstructionprashanthОценок пока нет
- Jurnal Urologi 234Документ8 страницJurnal Urologi 234Muhammad Rezi RamdanniОценок пока нет
- Advantages and Disadvantages of SurgeryДокумент10 страницAdvantages and Disadvantages of Surgeryawal_w_ajmal_nazraОценок пока нет
- Ureteral Stent For Ureteral Stricture: James F. Borin and Elspeth M. McdougallДокумент13 страницUreteral Stent For Ureteral Stricture: James F. Borin and Elspeth M. McdougallOoОценок пока нет
- Rectus Sheath Vs TAP BlocksДокумент6 страницRectus Sheath Vs TAP BlocksMikeMacKinnon100% (1)
- Jurnal 1 PDFДокумент5 страницJurnal 1 PDFsabila_chaОценок пока нет
- 9 Anaesthesia For ProstatectomyДокумент7 страниц9 Anaesthesia For ProstatectomySilvie DinОценок пока нет
- Instrumentations: Presented byДокумент27 страницInstrumentations: Presented byOmar AhmedОценок пока нет
- The Effects of Bladder Training On Bladder Functions After Transurethral Resection of ProstateДокумент21 страницаThe Effects of Bladder Training On Bladder Functions After Transurethral Resection of Prostatetrisna workОценок пока нет
- Inspection/Examination of The Ureter Biopsy: What Is The Evidence Base For This Information?Документ7 страницInspection/Examination of The Ureter Biopsy: What Is The Evidence Base For This Information?MarcelitaTaliaDuwiriОценок пока нет
- Benign Prostatic Hyperplasia BPH Transurethral Resection of The Prostate TurpДокумент8 страницBenign Prostatic Hyperplasia BPH Transurethral Resection of The Prostate TurpayamОценок пока нет
- Benign Prostatic HyperplasiaДокумент4 страницыBenign Prostatic HyperplasiaAdelle Fortunato100% (2)
- Lasers: Outpatient Transurethral Cystolithotripsy of Large Bladder Stones by Holmium LaserДокумент4 страницыLasers: Outpatient Transurethral Cystolithotripsy of Large Bladder Stones by Holmium LaserSteve aokiОценок пока нет
- KJR 18 299Документ10 страницKJR 18 299Willian HolandaОценок пока нет
- Postoperative Complication of Colorectal SurgeryДокумент29 страницPostoperative Complication of Colorectal SurgeryPeter ChenОценок пока нет
- Benign Prostatic Hypertrophy: Pathophysiology and EtiologyДокумент4 страницыBenign Prostatic Hypertrophy: Pathophysiology and EtiologyErnestomalamionОценок пока нет
- Benignprostatehyperplasia 190707164908Документ50 страницBenignprostatehyperplasia 190707164908jinsi georgeОценок пока нет
- BPH-Diagnosis and TreatmentДокумент7 страницBPH-Diagnosis and TreatmentMedissa MothОценок пока нет
- University College London Hospitals: Ureteroscopy/UreterorenosДокумент20 страницUniversity College London Hospitals: Ureteroscopy/UreterorenosrakaОценок пока нет
- Surgical Bed Side ProceduressДокумент62 страницыSurgical Bed Side Proceduressdrhiwaomer100% (1)
- Endoscopic Diagnosis and Treatment in Prostate Pathology: Handbook of EndourologyОт EverandEndoscopic Diagnosis and Treatment in Prostate Pathology: Handbook of EndourologyPetrisor Aurelian GeavleteОценок пока нет
- BPH 6Документ9 страницBPH 6nong danceОценок пока нет
- Striktur UrethraДокумент7 страницStriktur UrethraEl-yes Yonirazer El-BanjaryОценок пока нет
- Refrat: Wahyu Aji SetiabudiДокумент66 страницRefrat: Wahyu Aji SetiabudiariezaОценок пока нет
- Final EditДокумент43 страницыFinal EditMary Rose LinatocОценок пока нет
- Combined Laparoscopic Pyelolithotomy and Endoscopic Pyelolithotripsy For Staghorn Calculi: Long-Term Follow-Up Results From A Case SeriesДокумент6 страницCombined Laparoscopic Pyelolithotomy and Endoscopic Pyelolithotripsy For Staghorn Calculi: Long-Term Follow-Up Results From A Case SeriesantonОценок пока нет
- Uro Catheter JournalДокумент8 страницUro Catheter JournalKokong Duda kereОценок пока нет
- Nephro-Urology Monthly Nephro-Urology Monthly Nephro-Urology MonthlyДокумент3 страницыNephro-Urology Monthly Nephro-Urology Monthly Nephro-Urology MonthlyTheQueensafa90Оценок пока нет
- Prostate CancerДокумент6 страницProstate CancerfheisanzОценок пока нет
- BPH DefinitionДокумент5 страницBPH DefinitionMadhu Sudhan PandeyaОценок пока нет
- Karami 022 029Документ8 страницKarami 022 029TheQueensafa90Оценок пока нет
- 575-Article Text-1208-1-10-20100307Документ5 страниц575-Article Text-1208-1-10-20100307Richard HartantoОценок пока нет
- ErcpДокумент22 страницыErcpPutu YoanaОценок пока нет
- Acute Gastroenteritis (AGE) PDFДокумент37 страницAcute Gastroenteritis (AGE) PDFAries Chandra AnandithaОценок пока нет
- 8275 29195 1 PBДокумент8 страниц8275 29195 1 PBVijayakanth VijayakumarОценок пока нет
- Research Article: Awareness of StyeДокумент3 страницыResearch Article: Awareness of StyeUp TayyuОценок пока нет
- GastroFINALGuideline12 21 2011Документ20 страницGastroFINALGuideline12 21 2011Jam Knows RightОценок пока нет
- Bismillah - Osce PrintДокумент11 страницBismillah - Osce PrintMaya LarasОценок пока нет
- 8275 29195 1 PBДокумент8 страниц8275 29195 1 PBVijayakanth VijayakumarОценок пока нет
- Fulltext Ajpt v3 Id1072Документ5 страницFulltext Ajpt v3 Id1072Maya LarasОценок пока нет
- CLMДокумент4 страницыCLMMaya LarasОценок пока нет
- Daftar PustakaДокумент2 страницыDaftar PustakaMaya LarasОценок пока нет
- ProstateEnlargement 508 PDFДокумент20 страницProstateEnlargement 508 PDFMaya LarasОценок пока нет
- Bullous CLMДокумент2 страницыBullous CLMMaya LarasОценок пока нет
- 9 Anaesthesia For ProstatectomyДокумент7 страниц9 Anaesthesia For ProstatectomySilvie DinОценок пока нет
- Daftar PustakaДокумент2 страницыDaftar PustakaMaya LarasОценок пока нет
- 05 - 203perkembangan Terkini Diagnosis Dan Penatalaksanaan Imflammatory Bowel Disease PDFДокумент6 страниц05 - 203perkembangan Terkini Diagnosis Dan Penatalaksanaan Imflammatory Bowel Disease PDFrisda aulia putriОценок пока нет
- Rekuren T. KorporisДокумент4 страницыRekuren T. KorporisMaya LarasОценок пока нет
- Art:10.1007/s13555 016 0158 XДокумент5 страницArt:10.1007/s13555 016 0158 XMaya LarasОценок пока нет
- Art:10.1007/s13555 016 0158 XДокумент5 страницArt:10.1007/s13555 016 0158 XMaya LarasОценок пока нет
- 194 27 141 99Документ53 страницы194 27 141 99Fahri Dwi PermanaОценок пока нет
- CLMДокумент4 страницыCLMMaya LarasОценок пока нет
- Diet of Acne PDFДокумент15 страницDiet of Acne PDFMaya LarasОценок пока нет
- Review Patogenesis Treatment PDFДокумент6 страницReview Patogenesis Treatment PDFMaya LarasОценок пока нет
- FaecesДокумент18 страницFaecesMaya LarasОценок пока нет
- Comparison Between Fluconazole and Terbinafine in The Treatment ofДокумент6 страницComparison Between Fluconazole and Terbinafine in The Treatment ofPutry SampelanОценок пока нет
- Bullous CLMДокумент2 страницыBullous CLMMaya LarasОценок пока нет
- World's Largest Science, Technology & Medicine Open Access Book PublisherДокумент18 страницWorld's Largest Science, Technology & Medicine Open Access Book PublisherMaya LarasОценок пока нет
- 9 Anaesthesia For ProstatectomyДокумент7 страниц9 Anaesthesia For ProstatectomySilvie DinОценок пока нет
- Acute Gastroenteritis (AGE) PDFДокумент37 страницAcute Gastroenteritis (AGE) PDFAries Chandra AnandithaОценок пока нет
- C 2860 Aacbff 1Документ9 страницC 2860 Aacbff 1Muhammad FaizОценок пока нет
- Guide To Assessment and Management of Acute Gastroenteritis in Primary CareДокумент2 страницыGuide To Assessment and Management of Acute Gastroenteritis in Primary CareMaya LarasОценок пока нет
- Scientific Signs of Qur'an & SunnahДокумент26 страницScientific Signs of Qur'an & SunnahISLAMICULTURE100% (11)
- Sesi 3-Promoting B'feeding During PregnancyДокумент64 страницыSesi 3-Promoting B'feeding During PregnancyMazlina MaidinОценок пока нет
- Textile GlossaryДокумент143 страницыTextile GlossaryRanjana RajanОценок пока нет
- Anterior Single Implant Supported Restoration in Esthetic ZoneДокумент71 страницаAnterior Single Implant Supported Restoration in Esthetic ZoneAmar BimavarapuОценок пока нет
- AdvancedTrainingTechniquesforOxenTechGuide PDFДокумент23 страницыAdvancedTrainingTechniquesforOxenTechGuide PDFh1970hu100% (1)
- West Nile FeverДокумент24 страницыWest Nile Feveraliabh2006Оценок пока нет
- Citrasate: Product ManualДокумент30 страницCitrasate: Product ManualfidabimeeОценок пока нет
- Jurnal Dian Syahna Nazella Reviisi-1Документ10 страницJurnal Dian Syahna Nazella Reviisi-1Darwin AllОценок пока нет
- Riddle of DeathДокумент2 страницыRiddle of DeathReka182Оценок пока нет
- Shelter Quality Protocol 2014Документ50 страницShelter Quality Protocol 2014Tomislav Mikuš100% (1)
- Drugs Acting On Digestive System of AnimalsДокумент11 страницDrugs Acting On Digestive System of AnimalsSunil100% (3)
- Level+5+wordlist+12+3+12 RRДокумент148 страницLevel+5+wordlist+12+3+12 RRELISA GALINDO GUERRAОценок пока нет
- Anatomy and Physiology of BloodДокумент10 страницAnatomy and Physiology of Bloodaoi_rachelle100% (1)
- Electrolyte ImbalancesДокумент4 страницыElectrolyte Imbalancessccctutor100% (2)
- Jurnal EnglishДокумент2 страницыJurnal EnglishMuhd Afan AFuanОценок пока нет
- Dr. Nur Farhanah - SPEED TetanusДокумент24 страницыDr. Nur Farhanah - SPEED TetanusJonathan IngramОценок пока нет
- BibliographyДокумент2 страницыBibliographyapi-197414643Оценок пока нет
- SMNR - 4... Wound HealingДокумент62 страницыSMNR - 4... Wound HealingDrAmar GillОценок пока нет
- CWU Gynae Missed MiscarriageДокумент8 страницCWU Gynae Missed MiscarriageFaris Mohd NasirОценок пока нет
- GuppyДокумент2 страницыGuppymartynunez12345Оценок пока нет
- Biology ProjectДокумент27 страницBiology Projectravifact0% (2)
- General AnatomyДокумент25 страницGeneral AnatomyAltamae IbayОценок пока нет
- Air Sac Mites in ChickensДокумент6 страницAir Sac Mites in ChickensShah NawazОценок пока нет
- HPNДокумент26 страницHPNI-Focus PhotosОценок пока нет
- Gene Linkage and PolyploidyДокумент48 страницGene Linkage and Polyploidyjoey delgadoОценок пока нет
- NEMATODESДокумент4 страницыNEMATODESAbby VillamuchoОценок пока нет
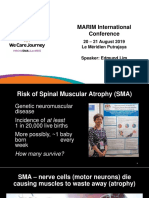
- WeCareJourney Edmund LimДокумент12 страницWeCareJourney Edmund LimPrabhuОценок пока нет
- Repair Reline & Rebase 1Документ51 страницаRepair Reline & Rebase 1huma100% (3)
- Dengue Update - As of Aug. 9, 2019Документ10 страницDengue Update - As of Aug. 9, 2019CHICKYОценок пока нет
- Cestoda and TrematodaДокумент42 страницыCestoda and Trematodadeneke100% (1)