Вам также может понравиться
- Nursing Care Plan Priorities: Risk For InjuryДокумент6 страницNursing Care Plan Priorities: Risk For InjuryPauling FrezОценок пока нет
- Nursing Care Plan For "HEMODIALYSIS"Документ5 страницNursing Care Plan For "HEMODIALYSIS"jhonroks100% (6)
- Course in The Ward: DialysisДокумент4 страницыCourse in The Ward: DialysisRayjundie EstradaОценок пока нет
- Doctors Order LoveДокумент4 страницыDoctors Order LoveAubrey Unique EvangelistaОценок пока нет
- NCP Icu-CcuДокумент6 страницNCP Icu-CcuJohn CenasОценок пока нет
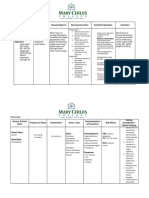
- Nursing Care Plan Date Assessed: December 11, 2017 Nursing Diagnosis Nursing Objective Nursing Intervention Scientific Explanation EvaluationДокумент2 страницыNursing Care Plan Date Assessed: December 11, 2017 Nursing Diagnosis Nursing Objective Nursing Intervention Scientific Explanation EvaluationCelyn Nicole Fernandez RollanОценок пока нет
- Case: Liver Cirrhosis Assessment:: Nursing InferenceДокумент7 страницCase: Liver Cirrhosis Assessment:: Nursing InferenceLovelyn GanirОценок пока нет
- Nursing Care Plan: Cues Objectives Interventions Rationale EvaluationДокумент10 страницNursing Care Plan: Cues Objectives Interventions Rationale EvaluationChamelli RobinОценок пока нет
- Learning Feedback DiaryДокумент10 страницLearning Feedback DiaryLoids IgnacioОценок пока нет
- Hemodialysis NCPДокумент2 страницыHemodialysis NCPAfia Tawiah33% (3)
- Risk For Acute ConfusionДокумент2 страницыRisk For Acute ConfusionChar PereaОценок пока нет
- Nursing Care Plan For Breast Cancer NCP PDFДокумент2 страницыNursing Care Plan For Breast Cancer NCP PDFMaina BarmanОценок пока нет
- Nursing Care PlanДокумент12 страницNursing Care Plankeishaaa29100% (6)
- ARTHROCENTESISДокумент2 страницыARTHROCENTESISJairene Dave Martinez CambalonОценок пока нет
- CYSTOCLYSIS3Документ9 страницCYSTOCLYSIS3Alvin OccianoОценок пока нет
- NCP Acute Pain RT CancerДокумент3 страницыNCP Acute Pain RT CancerCharissa Magistrado De LeonОценок пока нет
- CystoclysisДокумент2 страницыCystoclysisRaymond BasiloniaОценок пока нет
- NCP Ineffective Breathing GunshotДокумент3 страницыNCP Ineffective Breathing GunshotMikko Enoc100% (1)
- Cefipime HCL (AXERA)Документ2 страницыCefipime HCL (AXERA)Kristine YoungОценок пока нет
- Pre-Operative (Incision & Drainage of Abscess)Документ6 страницPre-Operative (Incision & Drainage of Abscess)Eunice MañalacОценок пока нет
- Lung Cancer (Nursing Care)Документ5 страницLung Cancer (Nursing Care)heiyuОценок пока нет
- Hypertensive NephrosclerosisДокумент14 страницHypertensive Nephrosclerosisreysanne100% (1)
- Aminogen Drug StudyДокумент2 страницыAminogen Drug Studymilesmin100% (1)
- NCP HyperthermiaДокумент1 страницаNCP HyperthermiaLeo_Rabacca_3610100% (1)
- Nursing Diagnosis of Prostate CancerДокумент3 страницыNursing Diagnosis of Prostate CancerSyafiqAzizi100% (1)
- Care of The Client With Pulmonary Tuberculosis Utilizing Orem's TheoryДокумент13 страницCare of The Client With Pulmonary Tuberculosis Utilizing Orem's TheoryRazel Kinette AzotesОценок пока нет
- Total Abdominal Hysterectomy Bilateral Salpingo OophorectomyДокумент3 страницыTotal Abdominal Hysterectomy Bilateral Salpingo OophorectomyMitch Elle Infante100% (1)
- Nursing Care Planreadiness of Enhanced Therapeutic Management CompressДокумент2 страницыNursing Care Planreadiness of Enhanced Therapeutic Management CompressMarlo Dañez NorbeОценок пока нет
- Nanda NCP BasedДокумент14 страницNanda NCP Baseddeliejoyce100% (1)
- Student Nurses' Community: Nursing Care Plan AmputationДокумент3 страницыStudent Nurses' Community: Nursing Care Plan AmputationNur faizah bt azmiОценок пока нет
- Discharge Care PlanДокумент2 страницыDischarge Care PlanLaurinda Angelica Dimaiwat PrestadoОценок пока нет
- Nursing Care Plan ColostomyДокумент5 страницNursing Care Plan ColostomyCarissa Mae Tapec EstradaОценок пока нет
- Assessment Nursing Diagnosis Planning Implemantation Rationale EvaluationДокумент2 страницыAssessment Nursing Diagnosis Planning Implemantation Rationale EvaluationChloie Marie Rosalejos100% (1)
- NCP Ch31 p991-992Документ2 страницыNCP Ch31 p991-992Ala'a Abd Mansor100% (2)
- 1 Acute Pain NCPДокумент2 страницы1 Acute Pain NCPFilipinas BelzaОценок пока нет
- TB, Ineffectivbe Breathing PatternsДокумент1 страницаTB, Ineffectivbe Breathing PatternsnikkilyceeОценок пока нет
- MGH 8 - Ihd - NCPДокумент12 страницMGH 8 - Ihd - NCPSesinando Niez Quilao Jr.100% (1)
- Soapie, Assessment and NCP On PAINДокумент7 страницSoapie, Assessment and NCP On PAINAna100% (2)
- Skin Grafting Surgical NursingДокумент21 страницаSkin Grafting Surgical NursingHEMMA100% (1)
- NCP Acute PainДокумент3 страницыNCP Acute PainDyanne BОценок пока нет
- Nursing Care PlanДокумент20 страницNursing Care PlanZamranosОценок пока нет
- NCP Gastric CancerДокумент6 страницNCP Gastric Cancerhayascent hilarioОценок пока нет
- NCP - Acute PainДокумент1 страницаNCP - Acute PainjsthrОценок пока нет
- Journal EntriesДокумент4 страницыJournal Entriesapi-315619551Оценок пока нет
- NCP Lack of KnowledgeДокумент3 страницыNCP Lack of KnowledgeFaye BartianaОценок пока нет
- Impaired Gas ExchangeДокумент10 страницImpaired Gas ExchangeWardinatul ImanОценок пока нет
- Icu NCPДокумент4 страницыIcu NCPdrsabuegОценок пока нет
- NCP BPHДокумент8 страницNCP BPHjyaba0% (1)
- DM & DI ExamsДокумент11 страницDM & DI ExamsTomzki CornelioОценок пока нет
- Concept Map: End Stage Renal DiseaseДокумент4 страницыConcept Map: End Stage Renal DiseaseAziil LiizaОценок пока нет
- NCP Liver CirrhosisДокумент7 страницNCP Liver CirrhosisIris Jimenez-BuanОценок пока нет
- TAHBSO Concept MapДокумент1 страницаTAHBSO Concept MapSherika Mariz Moreno GuarinОценок пока нет
- Nursing Care Plan AДокумент6 страницNursing Care Plan ACrystal WyattОценок пока нет
- You Are Caring For A Patient With An NG Feeding TubeДокумент2 страницыYou Are Caring For A Patient With An NG Feeding TubeWen Silver100% (1)
- Hemodialysis: NURSING DIAGNOSIS: Injury, Risk For (Loss of Vascular Access) Risk Factors May IncludeДокумент10 страницHemodialysis: NURSING DIAGNOSIS: Injury, Risk For (Loss of Vascular Access) Risk Factors May IncludeChevelle Valenciano-GaanОценок пока нет
- Demonstration ON Haemodialysis: Submitted ToДокумент46 страницDemonstration ON Haemodialysis: Submitted ToAbirajanОценок пока нет
- HemodialysisДокумент4 страницыHemodialysisJon Adam Bermudez SamatraОценок пока нет
- Pingen, Kathleen Joy R. BSN 3AДокумент3 страницыPingen, Kathleen Joy R. BSN 3AKathleen Joy PingenОценок пока нет
- ProstatectomyДокумент9 страницProstatectomymardsz100% (1)
- DialysisДокумент19 страницDialysisSachin Singh100% (2)
- NYSBoatersGuide PDFДокумент68 страницNYSBoatersGuide PDFAshleyОценок пока нет
- Assessment of Dry Weight in Hemodialysis: An Overview: ReviewДокумент12 страницAssessment of Dry Weight in Hemodialysis: An Overview: ReviewAshleyОценок пока нет
- AsnДокумент76 страницAsnAshleyОценок пока нет
- CH 6 WorksheetДокумент4 страницыCH 6 WorksheetAshley100% (1)
- CNNДокумент21 страницаCNNAshleyОценок пока нет
- Time Management Template For NursesДокумент3 страницыTime Management Template For NursesAshleyОценок пока нет
- 110 Ekg.1.8.2014. Ifn - Icp PDFДокумент27 страниц110 Ekg.1.8.2014. Ifn - Icp PDFAshleyОценок пока нет
- Cramer's Calls For: 12/21/2012 C Al L Pric e Portfo LioДокумент12 страницCramer's Calls For: 12/21/2012 C Al L Pric e Portfo LioAshleyОценок пока нет
- Neurological ChecklistДокумент2 страницыNeurological ChecklistAshley100% (1)
- 301 EDM ManualДокумент178 страниц301 EDM ManualAshley100% (1)
- Chapter 8Документ4 страницыChapter 8AshleyОценок пока нет
- MCQS Question: Qualitative ResearchДокумент5 страницMCQS Question: Qualitative ResearchAshley33% (3)
- Ob Peds Women S Health NotesДокумент176 страницOb Peds Women S Health NotesMikylla Huertas93% (28)
- Fever When Immunocompromised: ObjectivesДокумент7 страницFever When Immunocompromised: ObjectivesAshleyОценок пока нет
- Pneumonic For PD: Past Medical HX M I I M A S H Social HX S H O R E SДокумент1 страницаPneumonic For PD: Past Medical HX M I I M A S H Social HX S H O R E SAshleyОценок пока нет
- IB - Biology 2009 Syllabus (Almost Complete Set of Notes)Документ117 страницIB - Biology 2009 Syllabus (Almost Complete Set of Notes)Cristen100% (24)
- A Few Concepts: ST THДокумент4 страницыA Few Concepts: ST THAshleyОценок пока нет
- Population Genetics: Genetic Variation Within A PopulationДокумент26 страницPopulation Genetics: Genetic Variation Within A PopulationAshleyОценок пока нет
- 5-Chi Square Analysis TutorialДокумент17 страниц5-Chi Square Analysis TutorialAshleyОценок пока нет
- Genetics: From Genes To GenomesДокумент58 страницGenetics: From Genes To GenomesAshleyОценок пока нет
- Chapt04 ImagesДокумент48 страницChapt04 ImagesAshleyОценок пока нет
- Linkage & Mapping in Eukaryotes: Linkage & Chi Square For LinkageДокумент16 страницLinkage & Mapping in Eukaryotes: Linkage & Chi Square For LinkageAshleyОценок пока нет
- Biocontrol in Disease SugarcaneДокумент11 страницBiocontrol in Disease SugarcaneAlbar ConejoОценок пока нет
- Training 11 Add 3 enДокумент44 страницыTraining 11 Add 3 enBela CruzОценок пока нет
- ResumeДокумент2 страницыResumeapi-281248740Оценок пока нет
- Human Factors and Safety Culture in Maritime Safety (Revised)Документ10 страницHuman Factors and Safety Culture in Maritime Safety (Revised)Al-aayan D. IsmaelОценок пока нет
- Definition of Physical EducationДокумент7 страницDefinition of Physical EducationRose Jane BangisОценок пока нет
- Radiation Protection Rules 1971Документ10 страницRadiation Protection Rules 1971KomalОценок пока нет
- ANGIOSARCOMA pdf3 PDFДокумент9 страницANGIOSARCOMA pdf3 PDFعبدالعزيز عماد محمودОценок пока нет
- IZONE Academic WordlistДокумент59 страницIZONE Academic WordlistTrung KiênОценок пока нет
- Prevalence of Burkholderia Mallei in Equids of Remount Depot, Sargodha, PakistanДокумент6 страницPrevalence of Burkholderia Mallei in Equids of Remount Depot, Sargodha, PakistanMuhammad Naeem IqbalОценок пока нет
- Understanding Desistance From Crime Laub and SampsonДокумент70 страницUnderstanding Desistance From Crime Laub and Sampsonchrisgoss1Оценок пока нет
- PIIS0261561422000668 Micronitrientes: RequerimientosДокумент70 страницPIIS0261561422000668 Micronitrientes: Requerimientossulemi castañonОценок пока нет
- 1.3.1 The Autopsy-1Документ4 страницы1.3.1 The Autopsy-1Alyssa robertsОценок пока нет
- Cebu Normal University: Submitted By: DIANA ROSE B. ZAMORASДокумент3 страницыCebu Normal University: Submitted By: DIANA ROSE B. ZAMORASDiana ZamorasОценок пока нет
- 1 s2.0 S2667368123000116 MainДокумент24 страницы1 s2.0 S2667368123000116 MainCelia MartinezОценок пока нет
- Lumbar Interbody Fusions 1St Edition Edition Sunil Manjila Full ChapterДокумент67 страницLumbar Interbody Fusions 1St Edition Edition Sunil Manjila Full Chapterlaurence.williams167100% (6)
- Tsoukaki 2012Документ8 страницTsoukaki 2012Marina JoelОценок пока нет
- Sex Should Be Taught in Schools: Shafira Anindya Maharani X IPS 1 /29Документ11 страницSex Should Be Taught in Schools: Shafira Anindya Maharani X IPS 1 /29Shafira Anindya MaharaniОценок пока нет
- RP 11 - Measuring Concentration of Glucose Using A Calibration CurveДокумент4 страницыRP 11 - Measuring Concentration of Glucose Using A Calibration CurveAlfred SangОценок пока нет
- CLC - Good Copy Capstone ProposalДокумент6 страницCLC - Good Copy Capstone Proposalapi-549337583Оценок пока нет
- NK 48InjuryCategoryPackagesДокумент4 страницыNK 48InjuryCategoryPackagesJD Health Services TirupatturОценок пока нет
- TES Harian: Bahasa InggrisДокумент3 страницыTES Harian: Bahasa InggrisAlfiya HasnaОценок пока нет
- Harga Prolanis (Data Dari Apotek Online)Документ74 страницыHarga Prolanis (Data Dari Apotek Online)Orin Tri WulanОценок пока нет
- PNF 8th EditionДокумент7 страницPNF 8th EditionDanisaWajeОценок пока нет
- Matter For PGDIPC Course PromotionДокумент1 страницаMatter For PGDIPC Course PromotionAnkur VasudevaОценок пока нет
- Lepage Job WRKSHP 10-26-11Документ2 страницыLepage Job WRKSHP 10-26-11Andi ParkinsonОценок пока нет
- MDSAP QMS ManualДокумент43 страницыMDSAP QMS ManualmamjaguarОценок пока нет
- Statement of PurposeДокумент5 страницStatement of PurposesagvekarpoojaОценок пока нет
- The Girl With Green Eyes by John EscottДокумент10 страницThe Girl With Green Eyes by John EscottAyman Charoui essamadiОценок пока нет
- Insomnia: Management of Underlying ProblemsДокумент6 страницInsomnia: Management of Underlying Problems7OrangesОценок пока нет
- A Study On Pandemic Related Challenges Faced in Rural Areas: Patel Preja ID No: 20BBA125Документ9 страницA Study On Pandemic Related Challenges Faced in Rural Areas: Patel Preja ID No: 20BBA125PREJA PATELОценок пока нет
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)От EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Рейтинг: 3 из 5 звезд3/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedОт EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedРейтинг: 4.5 из 5 звезд4.5/5 (82)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDОт EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDРейтинг: 5 из 5 звезд5/5 (3)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionОт EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionРейтинг: 4 из 5 звезд4/5 (404)
- The Age of Magical Overthinking: Notes on Modern IrrationalityОт EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityРейтинг: 4 из 5 звезд4/5 (32)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeОт EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeРейтинг: 2 из 5 звезд2/5 (1)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaОт EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОт EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОценок пока нет
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsОт EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsРейтинг: 4 из 5 звезд4/5 (4)
- How to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipОт EverandHow to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipРейтинг: 4.5 из 5 звезд4.5/5 (1135)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsОт EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsРейтинг: 5 из 5 звезд5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisОт EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisРейтинг: 4.5 из 5 звезд4.5/5 (42)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeОт EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeРейтинг: 4.5 из 5 звезд4.5/5 (254)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessОт EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessРейтинг: 4.5 из 5 звезд4.5/5 (328)
- The Obesity Code: Unlocking the Secrets of Weight LossОт EverandThe Obesity Code: Unlocking the Secrets of Weight LossРейтинг: 4 из 5 звезд4/5 (6)
- Why We Die: The New Science of Aging and the Quest for ImmortalityОт EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityРейтинг: 4.5 из 5 звезд4.5/5 (6)
- Deep Sleep Hypnosis: Guided Meditation For Sleep & HealingОт EverandDeep Sleep Hypnosis: Guided Meditation For Sleep & HealingРейтинг: 4.5 из 5 звезд4.5/5 (104)
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingОт EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingРейтинг: 4 из 5 звезд4/5 (1138)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.От EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Рейтинг: 4.5 из 5 звезд4.5/5 (110)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsОт EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsРейтинг: 4.5 из 5 звезд4.5/5 (170)