Вам также может понравиться
- 1.prayudi FNL BDG Clinical Science DiagnoДокумент34 страницы1.prayudi FNL BDG Clinical Science DiagnoBoy Henri PasaribuОценок пока нет
- CV MikhailДокумент2 страницыCV MikhailMikhail NurhariОценок пока нет
- Sumihar Sijabat RSKTM H+2Документ2 страницыSumihar Sijabat RSKTM H+2Johannes TambunanОценок пока нет
- Populasi Parson LandscapeДокумент68 страницPopulasi Parson LandscapefaizrahmaanОценок пока нет
- 04 Data CRS Surveillance April 2023 (Data As of 08 Mei 2023)Документ16 страниц04 Data CRS Surveillance April 2023 (Data As of 08 Mei 2023)Yanti maruapeyОценок пока нет
- Anisa Aulia R CVДокумент1 страницаAnisa Aulia R CVSalsa AzrielОценок пока нет
- Undangan 1Документ2 страницыUndangan 1zaki hetamiОценок пока нет
- ERAS DR - TESAR SP - AnДокумент26 страницERAS DR - TESAR SP - AnAhmad Rifai R AОценок пока нет
- Prescription 229 MMMДокумент1 страницаPrescription 229 MMMSourav BiswasОценок пока нет
- List of Antigen Rapid Test Services - by Lion Air GroupДокумент4 страницыList of Antigen Rapid Test Services - by Lion Air Groupbocah tileОценок пока нет
- CV Tedy Jaswady 2Документ3 страницыCV Tedy Jaswady 2dedebojokursiОценок пока нет
- Clinical RotationДокумент2 страницыClinical RotationmyannbeguasОценок пока нет
- Surat Undangan Peserta Workshop Program HIV - H.5 Kab - Bone 08 Juni 2023Документ4 страницыSurat Undangan Peserta Workshop Program HIV - H.5 Kab - Bone 08 Juni 2023Surya MidwiferyОценок пока нет
- Karyawan Rsu Aliyah UpdateДокумент4 страницыKaryawan Rsu Aliyah UpdateAlza Ccr100% (1)
- Company Profile ESA Global Consulting - RSДокумент9 страницCompany Profile ESA Global Consulting - RSWiliam HansОценок пока нет
- Application For Employment Form-SignedДокумент4 страницыApplication For Employment Form-SignedDyki AnwarОценок пока нет
- CV DR Sabrina AnggrainiДокумент8 страницCV DR Sabrina Anggrainialiy_drОценок пока нет
- 1.3.3.a AJUAN PELATIHAN MP 2023Документ1 страница1.3.3.a AJUAN PELATIHAN MP 2023Wulan 160781Оценок пока нет
- To Jjtu 1STДокумент14 страницTo Jjtu 1STsrilalitha avinashОценок пока нет
- SKD 2021Документ15 страницSKD 2021NovidaYusnitaNasutionОценок пока нет
- Caraga Chapter: D.O. Plaza Memorial Provincial HospitalДокумент1 страницаCaraga Chapter: D.O. Plaza Memorial Provincial Hospitaljanel nayreОценок пока нет
- Pengkajian Gawat DaruratДокумент4 страницыPengkajian Gawat DaruratDekde Septian AdyОценок пока нет
- Umi (Univ. Muslim Indonesia)Документ16 страницUmi (Univ. Muslim Indonesia)Muslimin PutraОценок пока нет
- Jeena Jayan - CV Orig-2Документ5 страницJeena Jayan - CV Orig-2Raghavendran RamachandranОценок пока нет
- DeccvДокумент4 страницыDeccvapi-595636120Оценок пока нет
- Surat Tugas Khitan Massal SenduroДокумент2 страницыSurat Tugas Khitan Massal SenduroDjaka SambungОценок пока нет
- 2nd Annaouncement MCCRC 17 - 19 Mei SOLO 2024Документ4 страницы2nd Annaouncement MCCRC 17 - 19 Mei SOLO 2024dmandatari7327Оценок пока нет
- CV DR - Ade Adrain Sitompul (Indonesia) 2020Документ6 страницCV DR - Ade Adrain Sitompul (Indonesia) 2020AdraОценок пока нет
- Curriculum Vitae: Personal DataДокумент3 страницыCurriculum Vitae: Personal DataDelly MarsellinaОценок пока нет
- Struktur Organisasi Upt Puskesmas DTP Curugbitung Kabupaten Lebak TAHUN 2015Документ1 страницаStruktur Organisasi Upt Puskesmas DTP Curugbitung Kabupaten Lebak TAHUN 2015KochengОценок пока нет
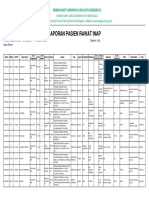
- Laporan Pasien Rawat InapДокумент15 страницLaporan Pasien Rawat InapsyadikiniОценок пока нет
- Report 8Документ4 страницыReport 8Rizkyastari OnnyОценок пока нет
- Apply Ade Adrain SitompulДокумент6 страницApply Ade Adrain Sitompulade adrain sitompulОценок пока нет
- SK Program Lampiran PKM Sukaraja 2014Документ6 страницSK Program Lampiran PKM Sukaraja 2014Puskesmas SukarajaОценок пока нет
- Fira Yunita PT Sabar GandaДокумент2 страницыFira Yunita PT Sabar GandaFira YunitaОценок пока нет
- CV Dian Pebriyanti SRGДокумент4 страницыCV Dian Pebriyanti SRGdian pebriyanti siregarОценок пока нет
- Dr. Chepi Priansyah Tegema: Personal DetailsДокумент2 страницыDr. Chepi Priansyah Tegema: Personal DetailsChepi PriansyahОценок пока нет
- Penugasan 1 KB 3Документ10 страницPenugasan 1 KB 3Cynthya Rinda ImaniarОценок пока нет
- Yora, DPJP DR SPOДокумент2 страницыYora, DPJP DR SPOPutri Nahrisa NstОценок пока нет
- Curriculum Vitae: Personal DataДокумент3 страницыCurriculum Vitae: Personal Databams_warsitoОценок пока нет
- Telemedicine Roster For July2022Документ7 страницTelemedicine Roster For July2022Nobojit DasОценок пока нет
- Surat Permohanan Stady Banding 2018Документ1 страницаSurat Permohanan Stady Banding 2018Fyphi MaharaniОценок пока нет
- Profile: Dr. I Made Dwi Tirtana, S.KedДокумент1 страницаProfile: Dr. I Made Dwi Tirtana, S.KedDwitirtana100% (1)
- CV - Pengayoman Medical CentreДокумент3 страницыCV - Pengayoman Medical CentreTommy KuncoroОценок пока нет
- Praktek DR Juwanto SP PD Pekanbaru - Google Search PDFДокумент1 страницаPraktek DR Juwanto SP PD Pekanbaru - Google Search PDFayu nanizaОценок пока нет
- Uptd Puskesmas Lohbener: Pemerintah Kabupaten Indramayu Dinas KesehatanДокумент2 страницыUptd Puskesmas Lohbener: Pemerintah Kabupaten Indramayu Dinas KesehatanwiwinОценок пока нет
- Curriculum Vitae: Date of Birth Gender Male Citizenship Religion Single AddressДокумент3 страницыCurriculum Vitae: Date of Birth Gender Male Citizenship Religion Single AddressareszqyОценок пока нет
- SKBS Dinda 2023 - CompressedДокумент1 страницаSKBS Dinda 2023 - CompressedAsmanОценок пока нет
- LAMARAN Rs Persada HospitalДокумент2 страницыLAMARAN Rs Persada HospitalMariya Tiyya MdfОценок пока нет
- Anisa Aulia R CVДокумент1 страницаAnisa Aulia R CVSalsa AzrielОценок пока нет
- Prescription - 540660 - 12 11 2020 - Dr. Bikash Majumder - Apollo 247Документ2 страницыPrescription - 540660 - 12 11 2020 - Dr. Bikash Majumder - Apollo 247soumitra choudhuryОценок пока нет
- NO Nama1 Jabatan1 Alamat1 Nama2 Jabatan2 Alamat2 Nama3 Jabatan3 Alamat3 Nama4 Jabatan4 Alamat4 Nama5 Jabatan5 Alamt5 Nama6Документ11 страницNO Nama1 Jabatan1 Alamat1 Nama2 Jabatan2 Alamat2 Nama3 Jabatan3 Alamat3 Nama4 Jabatan4 Alamat4 Nama5 Jabatan5 Alamt5 Nama6Irmayanti AR IrmayantiОценок пока нет
- 3.1.1.3 Pedoman Manual MutuДокумент46 страниц3.1.1.3 Pedoman Manual MutuKoperasi Pertanian Gema AgungОценок пока нет
- Letter of Acceptance (Loa) Jurnal Pasca Sarjana Institut Ilmu Kesehatan Strada IndonesiaДокумент1 страницаLetter of Acceptance (Loa) Jurnal Pasca Sarjana Institut Ilmu Kesehatan Strada IndonesiasumaiyahОценок пока нет
- Beta Health Full List of Hospitals and Medical CentresДокумент70 страницBeta Health Full List of Hospitals and Medical CentresAdedimeji FredОценок пока нет
- Lamaran Juli NurseДокумент18 страницLamaran Juli NurseRifai SinagaОценок пока нет
- Jadwal Soft Uat Simrs Kerinci: NO Modul Key User Estimasi Jadwal RABU, JULY 2018Документ2 страницыJadwal Soft Uat Simrs Kerinci: NO Modul Key User Estimasi Jadwal RABU, JULY 2018hendraОценок пока нет
- Rencana Operasi Elektif Ibs Rsud R Syamsudin SH SukabumiДокумент2 страницыRencana Operasi Elektif Ibs Rsud R Syamsudin SH SukabumibellinasarsaОценок пока нет
- Naovel Diana Fauziyah: Clinical Practice Position AppliedДокумент1 страницаNaovel Diana Fauziyah: Clinical Practice Position AppliednaovelОценок пока нет
- Cefepime: Ellie Marie F. Royales - PH-3AДокумент10 страницCefepime: Ellie Marie F. Royales - PH-3AEllie Marie RoyalesОценок пока нет
- مدونة كل العرب الطبية Davidson - Mcq - 22 - edition PDFДокумент232 страницыمدونة كل العرب الطبية Davidson - Mcq - 22 - edition PDFنورهانعزالدين100% (1)
- Antioxidant and Anticandidal Activity of Juniperus Communis L.Документ7 страницAntioxidant and Anticandidal Activity of Juniperus Communis L.ESSENCE - International Journal for Environmental Rehabilitation and ConservaionОценок пока нет
- Antibiotics: Lecture 6: Antibiotics For Anaerobic InfectionsДокумент12 страницAntibiotics: Lecture 6: Antibiotics For Anaerobic InfectionsMuath AlqarniОценок пока нет
- Introduction of MicrobiologyДокумент52 страницыIntroduction of MicrobiologyTri Wahyudi Iman DantaraОценок пока нет
- ScriptДокумент3 страницыScriptPonpimol Odee BongkeawОценок пока нет
- Antibiotic Classification: Generic Name Brand Names Common UsesДокумент5 страницAntibiotic Classification: Generic Name Brand Names Common Usesade_lubu100% (1)
- Pedia Recommended DosageДокумент5 страницPedia Recommended DosageNerak LuОценок пока нет
- Pelvic Inflammatory DiseaseДокумент9 страницPelvic Inflammatory DiseaseSohanInduwaraGamage100% (2)
- MEDICAMENTEДокумент13 страницMEDICAMENTELily Ozunu100% (1)
- MCB 308 Pharmaceutical Microbiology PDFДокумент23 страницыMCB 308 Pharmaceutical Microbiology PDFIlori OluwafemiОценок пока нет
- Ce Fur OximeДокумент4 страницыCe Fur Oximekanij fatima koliОценок пока нет
- IVcompatibility Ppn1221 WMДокумент8 страницIVcompatibility Ppn1221 WMwasim yousafОценок пока нет
- Formulation of Chloramphenicol in Situ Ophthalmic Gels Using Different Matrix CombinationsДокумент7 страницFormulation of Chloramphenicol in Situ Ophthalmic Gels Using Different Matrix CombinationsbrianОценок пока нет
- Antibiotic Susceptibility Patterns of Methicillin Resistant Staphyl - PDF NIHДокумент5 страницAntibiotic Susceptibility Patterns of Methicillin Resistant Staphyl - PDF NIHzia ul RahmanОценок пока нет
- Guava Review PDFДокумент17 страницGuava Review PDFPony ParadiseОценок пока нет
- UntitledДокумент24 страницыUntitledRicardo silvestreОценок пока нет
- Bacterial Meningitis HandoutДокумент7 страницBacterial Meningitis Handoutapi-648714317Оценок пока нет
- Doctors Order Form D4Документ1 страницаDoctors Order Form D4Marielle ChuaОценок пока нет
- TanninДокумент9 страницTannindedypurnamaОценок пока нет
- Reflective EssayДокумент1 страницаReflective Essayapi-357131209Оценок пока нет
- Otitis Media AkutДокумент28 страницOtitis Media AkutMuhammad IqbalОценок пока нет
- Antioxidant, Antibacterial and Antifungal Activity of Impatiens Sulcata Wallich in Roxb. ExtractsДокумент7 страницAntioxidant, Antibacterial and Antifungal Activity of Impatiens Sulcata Wallich in Roxb. ExtractsSSR-IIJLS JournalОценок пока нет
- Wound Management Formulary NHS PeterboroughДокумент77 страницWound Management Formulary NHS PeterboroughBrian HarrisОценок пока нет
- Pharmaceuticals Products ListДокумент51 страницаPharmaceuticals Products Listsks65Оценок пока нет
- EUCAST 2012 Disk MIC Breakpoint TableДокумент73 страницыEUCAST 2012 Disk MIC Breakpoint TableSayantan BanerjeeОценок пока нет
- 2013 CLSIFDA Table UpdateДокумент5 страниц2013 CLSIFDA Table UpdateNadir A IbrahimОценок пока нет
- Antibacterial Activity of The Extracts of Marine Red and Brown AlgaeДокумент6 страницAntibacterial Activity of The Extracts of Marine Red and Brown AlgaeelmisariОценок пока нет
- Ideal Qualities of An Antimicrobial AgentДокумент11 страницIdeal Qualities of An Antimicrobial AgentNissi PielagoОценок пока нет
- Evaluation of Antibacterial & Antioxidant Activities of The Leaf Essential Oil & Leaf Extracts of Citrus AurantifoliaДокумент9 страницEvaluation of Antibacterial & Antioxidant Activities of The Leaf Essential Oil & Leaf Extracts of Citrus AurantifoliaFirman TirmaОценок пока нет