Вам также может понравиться
- The Social Work and Human Services Treatment Planner, with DSM 5 UpdatesОт EverandThe Social Work and Human Services Treatment Planner, with DSM 5 UpdatesОценок пока нет
- Drug and Alcohol Psychosocial Interventions Professional Practice GuidelinesДокумент94 страницыDrug and Alcohol Psychosocial Interventions Professional Practice GuidelinesAlex PiecesОценок пока нет
- NSW Mental Health Policy on AggressionДокумент65 страницNSW Mental Health Policy on AggressionindahОценок пока нет
- PD2012 035Документ65 страницPD2012 035mohfirmanhamdaniОценок пока нет
- PD2012 069Документ21 страницаPD2012 069fhreankОценок пока нет
- NSW Health Records Policy SummaryДокумент21 страницаNSW Health Records Policy SummaryhopeloltestscribdОценок пока нет
- PD2005 187Документ8 страницPD2005 187api-3770073Оценок пока нет
- Pi Is 0196064418301148Документ5 страницPi Is 0196064418301148Anonymous 0WHX7nОценок пока нет
- GL2017 019Документ57 страницGL2017 019Muhammad NaufalОценок пока нет
- Clinical Placement NSWДокумент37 страницClinical Placement NSWrenata miateliОценок пока нет
- Early Pregnancy ComplciationsДокумент43 страницыEarly Pregnancy ComplciationsbbyesОценок пока нет
- PD2019_020Документ11 страницPD2019_020hatem newishyОценок пока нет
- Closed Head Injury in AdultsДокумент175 страницClosed Head Injury in AdultsElfiraОценок пока нет
- PD2014 028Документ30 страницPD2014 028Inne Milagros FransienDimpudusОценок пока нет
- Child Protetcion in CounselingДокумент263 страницыChild Protetcion in CounselingMadonna AngОценок пока нет
- Policy Directive: Children and Infants - Acute Management of CroupДокумент30 страницPolicy Directive: Children and Infants - Acute Management of CroupbedeskahericosОценок пока нет
- PD2017 013 PDFДокумент36 страницPD2017 013 PDFChico Hermanu BrillianОценок пока нет
- Mental Health Commissioner Monitoring and Advocacy Report 2018Документ106 страницMental Health Commissioner Monitoring and Advocacy Report 2018Stuff Newsroom100% (1)
- Policy Directive: Workplace Health and Safety: Policy and Better Practice Guide - NSW HealthДокумент43 страницыPolicy Directive: Workplace Health and Safety: Policy and Better Practice Guide - NSW HealthYwagar YwagarОценок пока нет
- Consultant PsychiatristДокумент13 страницConsultant PsychiatristDaniel LuuОценок пока нет
- UPS2Документ19 страницUPS2Carlos Miguel Mendoza LlamocaОценок пока нет
- Guide To Informed Decision-Making in Health CareДокумент80 страницGuide To Informed Decision-Making in Health CareClauОценок пока нет
- Personality Disorder - No Loger A Diagnosis of ExclusionДокумент54 страницыPersonality Disorder - No Loger A Diagnosis of ExclusionsanhourieОценок пока нет
- National Guidelines On Workplace Mental WellnessДокумент60 страницNational Guidelines On Workplace Mental WellnessCliff OngakiОценок пока нет
- Welcome To The Final Edition of The National Mental Health Development Unit (NMHDU) News BriefingДокумент14 страницWelcome To The Final Edition of The National Mental Health Development Unit (NMHDU) News Briefingtony_jameson-allenОценок пока нет
- Policy Directive: Visiting Practitioners and Staff Specialists Delineation of Clinical Privileges For Policy For ImpДокумент39 страницPolicy Directive: Visiting Practitioners and Staff Specialists Delineation of Clinical Privileges For Policy For ImpreyОценок пока нет
- GL2013 006Документ37 страницGL2013 006Marcelo UGОценок пока нет
- Job Spec HSE Area Lead of Service User Family CarerДокумент7 страницJob Spec HSE Area Lead of Service User Family CarerGateway ProjectОценок пока нет
- NSW Health Pd2023 002 PDFДокумент18 страницNSW Health Pd2023 002 PDFMeОценок пока нет
- The Nhs Talking Therapies Manual v6Документ156 страницThe Nhs Talking Therapies Manual v6DevyanshОценок пока нет
- PD2005 627Документ12 страницPD2005 627api-3770073Оценок пока нет
- Proposal Project. Group 1Документ22 страницыProposal Project. Group 1Pham Thi Que (K17 DN)Оценок пока нет
- Guia DDДокумент44 страницыGuia DDAntónio MartinsОценок пока нет
- The Role of Community Mental Health Teams in Delivering Community Mental Health ServicesДокумент23 страницыThe Role of Community Mental Health Teams in Delivering Community Mental Health ServicesNur LestaryОценок пока нет
- PD2014 025Документ13 страницPD2014 025brookie8868Оценок пока нет
- CMHC Implement Guideline 2013 Psych Services MalasiaДокумент47 страницCMHC Implement Guideline 2013 Psych Services MalasiaVanessa Herrera LopezОценок пока нет
- Gad-7 Questionnaire SpanishДокумент86 страницGad-7 Questionnaire Spanishrowanpurdy100% (1)
- Department of Health - National Mental Health Program - 2011-10-21Документ7 страницDepartment of Health - National Mental Health Program - 2011-10-21daryl ann dep-asОценок пока нет
- SciptДокумент8 страницSciptnurulamirahhamzahОценок пока нет
- Telepsychiatry Operational Guidelines 2020Документ58 страницTelepsychiatry Operational Guidelines 2020SHIVANGI KUMARIОценок пока нет
- Shared Decision Making Summary Guide v1Документ14 страницShared Decision Making Summary Guide v1Katja DunsmuirОценок пока нет
- National Mental Health Programme (NMHP) OverviewДокумент19 страницNational Mental Health Programme (NMHP) OverviewPratibha LoarОценок пока нет
- Munity Psychiatry - COPДокумент16 страницMunity Psychiatry - COPCarlos Luque GОценок пока нет
- Performance Measures For Mental Healthcare in Singapore: CommentaryДокумент6 страницPerformance Measures For Mental Healthcare in Singapore: Commentarypaijosuseno2242Оценок пока нет
- Patient/Primary Medical Home Foundation For Transformation: @paul - PCMHДокумент36 страницPatient/Primary Medical Home Foundation For Transformation: @paul - PCMHabdullahОценок пока нет
- Managementul Depresiei in Medicina PrimaraДокумент46 страницManagementul Depresiei in Medicina PrimaraSendruc OvidiuОценок пока нет
- NSW Health (1) - Infection Control PolicyДокумент56 страницNSW Health (1) - Infection Control Policyhanumana_dasaОценок пока нет
- PD2017 019Документ31 страницаPD2017 019mert05Оценок пока нет
- PD2005 568Документ21 страницаPD2005 568api-3770073100% (1)
- Annual Business ReportДокумент57 страницAnnual Business ReportCristina GirniceanuОценок пока нет
- Psychiatry Operational PolicyДокумент124 страницыPsychiatry Operational PolicyFarah Nasyitah100% (2)
- HSE guidance on supervision for health professionalsДокумент18 страницHSE guidance on supervision for health professionalsLexОценок пока нет
- Recruitment Pack - NLCG-123Документ13 страницRecruitment Pack - NLCG-123M LubisОценок пока нет
- Best Practice Guidelines Physiotherapy EIPIC 2Документ66 страницBest Practice Guidelines Physiotherapy EIPIC 2Ankur ShahОценок пока нет
- Inseparable Federal ActionsДокумент21 страницаInseparable Federal ActionsAralee HenighanОценок пока нет
- Medical Equipment Management and Maintenance PolicyДокумент28 страницMedical Equipment Management and Maintenance Policytaioba2010Оценок пока нет
- Doh Mtra PDFДокумент8 страницDoh Mtra PDFElaine DabuОценок пока нет
- A Recovery Vision For RehabilitationДокумент68 страницA Recovery Vision For RehabilitationGlencharlesworthОценок пока нет
- Protocol Dental TriageДокумент3 страницыProtocol Dental TriageastroirmaОценок пока нет
- Guidelines For Triage of Obstetric PatientsДокумент16 страницGuidelines For Triage of Obstetric Patientsastroirma0% (2)
- Manchester Triage System PDFДокумент112 страницManchester Triage System PDFastroirma100% (1)
- Aust Triage ScaleДокумент3 страницыAust Triage ScalemutiaОценок пока нет
- EYE EDUCATION FOR EMERGENCY CLINICIANS: Triage and Ocular HistoryДокумент33 страницыEYE EDUCATION FOR EMERGENCY CLINICIANS: Triage and Ocular HistoryastroirmaОценок пока нет
- 57.121 DenomProc BLANKДокумент2 страницы57.121 DenomProc BLANKastroirmaОценок пока нет
- Dental TriageДокумент62 страницыDental TriageastroirmaОценок пока нет
- Effect of A Triage Course On Quality of Rating Triage Codes in A Group of University Nursing Students: A Before-After Observational StudyДокумент6 страницEffect of A Triage Course On Quality of Rating Triage Codes in A Group of University Nursing Students: A Before-After Observational StudySriatiОценок пока нет
- FG 1Документ13 страницFG 1astroirmaОценок пока нет
- Ref 2Документ9 страницRef 2astroirmaОценок пока нет
- ASIA ClassificationДокумент2 страницыASIA ClassificationCarlos Avilés GutierrezОценок пока нет
- Sirriraj ScoreДокумент1 страницаSirriraj ScoreastroirmaОценок пока нет
- Aydemir and BedirДокумент5 страницAydemir and BedirastroirmaОценок пока нет
- GuidlinesДокумент10 страницGuidlinesbubuvulpeaОценок пока нет
- Endotracheal Tube ETT Insertion IntubationДокумент3 страницыEndotracheal Tube ETT Insertion IntubationmochkurniawanОценок пока нет
- Books About GroupsДокумент25 страницBooks About GroupsgerawenceОценок пока нет
- Pharmacodynamics and Therapeutic Applications of Iboga and IbogaineДокумент25 страницPharmacodynamics and Therapeutic Applications of Iboga and IbogainejesterstableОценок пока нет
- Ethical Issues at The End of LifeДокумент24 страницыEthical Issues at The End of Lifeorderstuff36160100% (1)
- DPT Doctor of Physiotherapy Program at Abu Zafar InstituteДокумент44 страницыDPT Doctor of Physiotherapy Program at Abu Zafar InstituteAbdul basit KaleemОценок пока нет
- Implant OcclusionДокумент52 страницыImplant OcclusionElango25489100% (3)
- Molluscum Contagiosum Andrew N PitzpatrickДокумент5 страницMolluscum Contagiosum Andrew N PitzpatrickHel DaОценок пока нет
- The Crashing Ventilated Patient Algorthm (Jairo I. Santanilla, ACEP, 2011)Документ1 страницаThe Crashing Ventilated Patient Algorthm (Jairo I. Santanilla, ACEP, 2011)PkernОценок пока нет
- Revised Kanda NCPДокумент3 страницыRevised Kanda NCPhaxa yzaОценок пока нет
- A-2012 Knee (Copy-1)Документ73 страницыA-2012 Knee (Copy-1)Yuri KemalОценок пока нет
- ReikiДокумент2 страницыReikiaiccclaОценок пока нет
- Parkland Formula For Burns Calculated DecisionsДокумент2 страницыParkland Formula For Burns Calculated DecisionsJulia Ines ObregonОценок пока нет
- EnglishДокумент56 страницEnglishPankaj SharmaОценок пока нет
- Clinical Manual - Part 2 - Drug Infusion Guidelines Revised - July 2015 - V7.11Документ58 страницClinical Manual - Part 2 - Drug Infusion Guidelines Revised - July 2015 - V7.11Jayaprakash KuppusamyОценок пока нет
- Self-motivation quiz tipsДокумент1 страницаSelf-motivation quiz tipsRose D GuzmanОценок пока нет
- Sustained Release Dosage FormsДокумент9 страницSustained Release Dosage FormsJasdeep KaurОценок пока нет
- What Are Extrapyramidal SymptomsДокумент2 страницыWhat Are Extrapyramidal SymptomscristieristiieОценок пока нет
- Preterm Labor ManagementДокумент50 страницPreterm Labor ManagementDr-Firas Nayf Al-ThawabiaОценок пока нет
- Mindfulness Group Lesson PlansДокумент3 страницыMindfulness Group Lesson Plansapi-469144202Оценок пока нет
- Nurse Practitioner VS Physical TherapistsДокумент5 страницNurse Practitioner VS Physical Therapistspdet1Оценок пока нет
- Dialog EFN2 Sudarmi 30140114040Документ2 страницыDialog EFN2 Sudarmi 30140114040sudarmiОценок пока нет
- Epidemiology & Social Costs of Haemophilia in India: Review ArticleДокумент13 страницEpidemiology & Social Costs of Haemophilia in India: Review ArticleDharmendra B MistryОценок пока нет
- ProposalДокумент45 страницProposalJP firmОценок пока нет
- NCP - Acute Pain Stomach CancerДокумент2 страницыNCP - Acute Pain Stomach CancerJohn Michael TaylanОценок пока нет
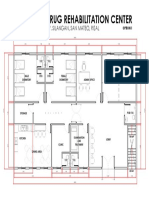
- Proposed Drug Rehabilitation Center: Monterey Sudb., Brgy. Silangan, San Mateo, RizalДокумент1 страницаProposed Drug Rehabilitation Center: Monterey Sudb., Brgy. Silangan, San Mateo, RizalJonathan MazonОценок пока нет
- USUHS Anesthesia Pharmacology NotesetДокумент247 страницUSUHS Anesthesia Pharmacology NotesetSean Bancroft100% (3)
- Transitioning Anticoagulants 2016Документ4 страницыTransitioning Anticoagulants 2016S_XangaiОценок пока нет
- Community Building ProcessДокумент17 страницCommunity Building ProcessKarolina HutagalungОценок пока нет
- Risk Management in PVДокумент40 страницRisk Management in PVSutirtho Mukherji100% (1)