Вам также может понравиться
- Zhao Mingyao: BMC - Zzu. 2006-2-12Документ32 страницыZhao Mingyao: BMC - Zzu. 2006-2-12api-19916399Оценок пока нет
- Kuliah Mineral 2015-2016Документ20 страницKuliah Mineral 2015-2016molenОценок пока нет
- Calcium, Magnesium, and Potassium Homeostasis: OutlineДокумент10 страницCalcium, Magnesium, and Potassium Homeostasis: OutlineMigs MedinaОценок пока нет
- Keseimbangan Elektrolit Dan Asam Basa: Dr. Satriawan Abadi, SP - Pd-KicДокумент79 страницKeseimbangan Elektrolit Dan Asam Basa: Dr. Satriawan Abadi, SP - Pd-KicdrroytambunanОценок пока нет
- 2 - Renal Secretion & AbsorptionДокумент14 страниц2 - Renal Secretion & AbsorptionHamzehОценок пока нет
- Dr. Hendrata - CLINICAL POTASSIUM IMBALANCE (Slide PERNEFRI Jakarta (24-27 Nop 2011)Документ45 страницDr. Hendrata - CLINICAL POTASSIUM IMBALANCE (Slide PERNEFRI Jakarta (24-27 Nop 2011)Patricia WenОценок пока нет
- Potassium HomeostasisДокумент47 страницPotassium HomeostasisMayuresh ChaudhariОценок пока нет
- Fluid and Electrolyte Imbalances Part 1Документ34 страницыFluid and Electrolyte Imbalances Part 1Gabrielle Frances FernandezОценок пока нет
- Keseimbangan Elektrolit Dan Asam Basa: Dr. Satriawan Abadi, SP - Pd-KicДокумент79 страницKeseimbangan Elektrolit Dan Asam Basa: Dr. Satriawan Abadi, SP - Pd-KicSteven KatuukОценок пока нет
- Keseimbangan Elektrolit Dan Asam Basa: Dr. Satriawan Abadi, SP - Pd-KicДокумент79 страницKeseimbangan Elektrolit Dan Asam Basa: Dr. Satriawan Abadi, SP - Pd-KicInterna FKUNHASОценок пока нет
- 30 GuytonДокумент7 страниц30 GuytonBianca Louise Chan LimОценок пока нет
- Maintenance FluidДокумент27 страницMaintenance FluidganeshyaeОценок пока нет
- Sodium, Potassium and The AnaesthetistДокумент14 страницSodium, Potassium and The AnaesthetistBayu Budi SukocoОценок пока нет
- Electrolytes: Dedykusuma@ugm - Ac.idДокумент20 страницElectrolytes: Dedykusuma@ugm - Ac.idRama DhistaОценок пока нет
- Emergencies in Nephrology:: ObjectivesДокумент9 страницEmergencies in Nephrology:: ObjectivesAndy F MonroeОценок пока нет
- Potassium BalanceДокумент13 страницPotassium BalancePhysiology by Dr Raghuveer100% (1)
- 19 HyperkalemiaДокумент36 страниц19 HyperkalemiaJoel Topf100% (3)
- 16-K-Ca ImbalanceДокумент11 страниц16-K-Ca Imbalanceمصطفى محمد جواد كاظمОценок пока нет
- Potassium Homeostasis & DisordersДокумент20 страницPotassium Homeostasis & DisordersHassan SalamehОценок пока нет
- Renal Glucose and Acid Base BalanceДокумент18 страницRenal Glucose and Acid Base BalanceAgasi MkОценок пока нет
- Metabolic AlkalosisДокумент54 страницыMetabolic AlkalosispriyankagalhotraОценок пока нет
- Lecture 22 - Fluid & Electrolyte Balance2 - 21 Oct 2006Документ28 страницLecture 22 - Fluid & Electrolyte Balance2 - 21 Oct 2006api-3703352Оценок пока нет
- Disorder of Potassium MetabolismДокумент28 страницDisorder of Potassium MetabolismSaif AliОценок пока нет
- K Disorders CCN PDFДокумент14 страницK Disorders CCN PDFLuis CuestaОценок пока нет
- Hypokalemia: A Practical Approach To Diagnosis and TreatmentДокумент17 страницHypokalemia: A Practical Approach To Diagnosis and TreatmentIntan NoaОценок пока нет
- Electrolytes PDFДокумент5 страницElectrolytes PDFFrances FranciscoОценок пока нет
- Serum Potassium: DR Sana Iqbal JanjuaДокумент18 страницSerum Potassium: DR Sana Iqbal JanjuahadibabaОценок пока нет
- Chapter 30 PhysiologyДокумент6 страницChapter 30 PhysiologyBianca Louise Chan LimОценок пока нет
- Imbalance of PotassiumДокумент16 страницImbalance of Potassiumapi-19916399Оценок пока нет
- Introducton Renal Physiolgy: Physiology Department Medical School, University of Methodist IndonesiaДокумент47 страницIntroducton Renal Physiolgy: Physiology Department Medical School, University of Methodist IndonesiaHachi Nini Shop II100% (1)
- DKA Anesthesia Management. DR M MagdyДокумент9 страницDKA Anesthesia Management. DR M MagdyHany ElbarougyОценок пока нет
- Potassium Disorders: Syeda Shaheera ZaidiДокумент60 страницPotassium Disorders: Syeda Shaheera ZaidiMohammad AliОценок пока нет
- Plasma K Is Around 4mmol, So Relatively That's Low. Na Is 140mmolДокумент24 страницыPlasma K Is Around 4mmol, So Relatively That's Low. Na Is 140mmoljavibruinОценок пока нет
- HyperkalemiaДокумент30 страницHyperkalemiaAyanna100% (3)
- Dangerous Rhythms Tachycardia: Potassium Electrolyte HypokalemiaДокумент7 страницDangerous Rhythms Tachycardia: Potassium Electrolyte HypokalemiagorodoeОценок пока нет
- B5W4 Renal Regulation of Potassium Homeostasis STUDENTДокумент29 страницB5W4 Renal Regulation of Potassium Homeostasis STUDENTInhoОценок пока нет
- Aldosterone Regulation of Sodium: Atrial Natriuretic Peptide ANPДокумент4 страницыAldosterone Regulation of Sodium: Atrial Natriuretic Peptide ANPHanoof GhaziОценок пока нет
- GI PhysiologyДокумент117 страницGI Physiologykhorrami4Оценок пока нет
- Physiology 8-5-2013Документ4 страницыPhysiology 8-5-2013AmanyОценок пока нет
- 17 Introduction To PotassiumДокумент18 страниц17 Introduction To PotassiumJoel TopfОценок пока нет
- Tubular Secretion by The Renal Tubules: Prof./ Ibrahim Mohamady IbrahimДокумент20 страницTubular Secretion by The Renal Tubules: Prof./ Ibrahim Mohamady IbrahimOsama MohamedОценок пока нет
- Hypokalemia 2Документ32 страницыHypokalemia 2aqilasafikaОценок пока нет
- 4 ElectrolyteДокумент30 страниц4 ElectrolytePesan IslamОценок пока нет
- Mineral, PH, Immunological Markers Plus CaseДокумент55 страницMineral, PH, Immunological Markers Plus CaseVio MincuОценок пока нет
- Fluids & Electrolytes Acid/Bas Balance: DR Wael SadaqahДокумент72 страницыFluids & Electrolytes Acid/Bas Balance: DR Wael Sadaqahdr wael sadaqaОценок пока нет
- HyponatremiaДокумент1 страницаHyponatremiaLouay KilaОценок пока нет
- Regulation of Water & Electrolytes Balance: By: Husnil KadriДокумент41 страницаRegulation of Water & Electrolytes Balance: By: Husnil KadrimarsyaОценок пока нет
- Seminar RДокумент93 страницыSeminar Rmubarak abdulkadirОценок пока нет
- Gangguan Keseimbangan Cairan Dan ElektrolitДокумент45 страницGangguan Keseimbangan Cairan Dan Elektrolitmulyo utomoОценок пока нет
- Electrolytes - HypokalamiaДокумент21 страницаElectrolytes - HypokalamiamympomОценок пока нет
- 467 2010 Article 1699Документ8 страниц467 2010 Article 1699anindia wardhaniОценок пока нет
- DCT and Collecting DuctДокумент29 страницDCT and Collecting DuctayeshaОценок пока нет
- Renal Tubular Acidosis: Moderator:Dr Nitin Joshi Presented By: Dr. Parth Nathwani MGM Medical College, MumbaiДокумент71 страницаRenal Tubular Acidosis: Moderator:Dr Nitin Joshi Presented By: Dr. Parth Nathwani MGM Medical College, MumbaiariОценок пока нет
- Renal Physiology ReviewДокумент7 страницRenal Physiology ReviewHOD AnesthesiaОценок пока нет
- Hyperkalemia: Michael Levin, D.O. Medical Resident PGY II P.C.O.MДокумент22 страницыHyperkalemia: Michael Levin, D.O. Medical Resident PGY II P.C.O.MsuviacesoОценок пока нет
- Physiology 1 Fluid ElectrolyteДокумент38 страницPhysiology 1 Fluid ElectrolyteHaziq KamardinОценок пока нет
- Tubular ReabsorptionДокумент42 страницыTubular Reabsorptionmina mounirОценок пока нет
- Disorders of Potassium BalanceДокумент41 страницаDisorders of Potassium BalanceUmesh BabuОценок пока нет
- TWIS, Fluid and Electrolytes-4Документ45 страницTWIS, Fluid and Electrolytes-4Madison FОценок пока нет
- Osce Stations For Medical Final 1Документ40 страницOsce Stations For Medical Final 1Freedom SunОценок пока нет
- Uterine Compression Sutures For Postpartum Hemorrhage - An OverviewДокумент8 страницUterine Compression Sutures For Postpartum Hemorrhage - An OverviewJoezelleОценок пока нет
- OphthalmologyДокумент92 страницыOphthalmologyMd Israt KhanОценок пока нет
- OB 1 - 1.02 Physiology of Menstruation and Decidua PDFДокумент11 страницOB 1 - 1.02 Physiology of Menstruation and Decidua PDFMDreamerОценок пока нет
- Staphylococcus: Organism Biology Tests Clinical Manifestations Virulence and Antigenic Factors Treatment Gram (+)Документ22 страницыStaphylococcus: Organism Biology Tests Clinical Manifestations Virulence and Antigenic Factors Treatment Gram (+)JoezelleОценок пока нет
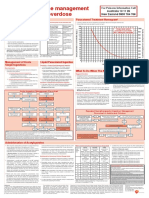
- Paracetamol OD Poster 2016 VersionДокумент1 страницаParacetamol OD Poster 2016 Versionmuhamed bwamkuuОценок пока нет
- Staphylococcus: Organism Biology Tests Clinical Manifestations Virulence and Antigenic Factors Treatment Gram (+)Документ22 страницыStaphylococcus: Organism Biology Tests Clinical Manifestations Virulence and Antigenic Factors Treatment Gram (+)JoezelleОценок пока нет
- 2011 - Sspe PDFДокумент230 страниц2011 - Sspe PDFJean Michael Castillo100% (1)
- Parasitology MicrosДокумент17 страницParasitology MicrosJoezelleОценок пока нет
- Electrocardiography: I. Leads A. Limb LeadsДокумент11 страницElectrocardiography: I. Leads A. Limb LeadsJoezelle0% (1)
- CohortДокумент3 страницыCohortJoezelleОценок пока нет
- 2.01b Gluteal Region Posterior Lower ExtremitiesДокумент64 страницы2.01b Gluteal Region Posterior Lower ExtremitiesJoezelleОценок пока нет
- Case K Sports Physiology - Exercise Associated HyponatremiaДокумент6 страницCase K Sports Physiology - Exercise Associated HyponatremiaJoezelleОценок пока нет
- Case K Sports Physiology - Exercise Associated HyponatremiaДокумент6 страницCase K Sports Physiology - Exercise Associated HyponatremiaJoezelleОценок пока нет
- Ward 1: Group 4: Paras, Payad, Pedrosa, Pinlac, Roldan, SalungaДокумент30 страницWard 1: Group 4: Paras, Payad, Pedrosa, Pinlac, Roldan, SalungaJoezelleОценок пока нет
- Posterior Ciliary Artery Circulation in Health and DiseaseДокумент9 страницPosterior Ciliary Artery Circulation in Health and DiseaseJoezelleОценок пока нет
- Cartas Contra La HumanidadДокумент31 страницаCartas Contra La Humanidadjohn_200000080% (5)
- Owth - Maturity: Words Selected by PaulДокумент3 страницыOwth - Maturity: Words Selected by PaulJoezelleОценок пока нет
- PHT 2Документ49 страницPHT 2Juliet Cayao SajolОценок пока нет
- Descriptive MammalsДокумент11 страницDescriptive MammalsS Nurul HalimahОценок пока нет
- Cranial Base ScottДокумент30 страницCranial Base ScottShirley AliagaОценок пока нет
- BIOLOGY (0610) s03 QP 3 Model Answer FinalДокумент15 страницBIOLOGY (0610) s03 QP 3 Model Answer FinalDON-thegreat100% (8)
- Zika VirusДокумент25 страницZika VirusSumit Sharma PoudelОценок пока нет
- Spoof TextДокумент9 страницSpoof TextHeather LeeОценок пока нет
- Chapter 19 Microbial Diseases of The Skin and WoundsДокумент8 страницChapter 19 Microbial Diseases of The Skin and WoundsGRACE MAR CABAHUG100% (1)
- 200 - First ResponseДокумент218 страниц200 - First Responsemoqmer100% (1)
- Open-Cap Acrylic SplintДокумент3 страницыOpen-Cap Acrylic SplintFeras Al-ZbounОценок пока нет
- Leadfinger GoblinДокумент1 страницаLeadfinger GoblinBrianОценок пока нет
- AGGIE Board ReviwerДокумент43 страницыAGGIE Board ReviwerQuinnee Vallejos100% (2)
- SD - Cauda Equina InglesДокумент20 страницSD - Cauda Equina InglesRodriguezОценок пока нет
- Goat Housing and Fencing PDFДокумент43 страницыGoat Housing and Fencing PDFmary anthoneth bayle100% (1)
- Chapter 38 Animal DevelopmentДокумент77 страницChapter 38 Animal Developmentmaria banunaekОценок пока нет
- Trial IGCSE (P1) 2022 - 2023Документ16 страницTrial IGCSE (P1) 2022 - 2023Andrew PooleОценок пока нет
- Enfermedades EmergentesДокумент216 страницEnfermedades EmergentesCaaarolОценок пока нет
- Data Review Meeting Template 2018 Final 1Документ19 страницData Review Meeting Template 2018 Final 1AdraОценок пока нет
- CHEESE - Dairy Processing Handbook PDFДокумент30 страницCHEESE - Dairy Processing Handbook PDFVVОценок пока нет
- GCSE AQA Biology Unit 3Документ10 страницGCSE AQA Biology Unit 3Fasih AhmadОценок пока нет
- Keperawatan Medikal Bedah Ii Skenario 2Документ19 страницKeperawatan Medikal Bedah Ii Skenario 2Nastiti DamayantiОценок пока нет
- MSC ZoologyДокумент26 страницMSC ZoologyRaji Deol BandeshaОценок пока нет
- Anatomy and Physiology PDFДокумент51 страницаAnatomy and Physiology PDFalexenneth canilaОценок пока нет
- Microsoft Word Document جديدДокумент3 страницыMicrosoft Word Document جديدHisham EssamОценок пока нет
- Gambar Usg TestisДокумент28 страницGambar Usg TestisIrfan YHОценок пока нет
- Maternal QuestionsДокумент7 страницMaternal Questionsjhae_darilayОценок пока нет
- NBDE Dental Boards Oral Surgery-27Документ27 страницNBDE Dental Boards Oral Surgery-27amitdineshp100% (11)
- Bubbles HeДокумент39 страницBubbles HePerrilyn PereyОценок пока нет
- Rabies SeminarДокумент73 страницыRabies SeminarQazi Muhammad IqbalОценок пока нет
- BODY TISSUES Reviewer 3Документ3 страницыBODY TISSUES Reviewer 3Jaira EmmarinaОценок пока нет
- Ba Duan JinДокумент58 страницBa Duan JinpositivamenteОценок пока нет
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)От EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Рейтинг: 3 из 5 звезд3/5 (1)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDОт EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDРейтинг: 5 из 5 звезд5/5 (2)
- The Age of Magical Overthinking: Notes on Modern IrrationalityОт EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityРейтинг: 4 из 5 звезд4/5 (29)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionОт EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionРейтинг: 4 из 5 звезд4/5 (404)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОт EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОценок пока нет
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedОт EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedРейтинг: 5 из 5 звезд5/5 (81)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeОт EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeРейтинг: 2 из 5 звезд2/5 (1)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessОт EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessРейтинг: 4.5 из 5 звезд4.5/5 (328)
- The Obesity Code: Unlocking the Secrets of Weight LossОт EverandThe Obesity Code: Unlocking the Secrets of Weight LossРейтинг: 4 из 5 звезд4/5 (6)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaОт EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisОт EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisРейтинг: 4.5 из 5 звезд4.5/5 (42)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsОт EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsРейтинг: 3.5 из 5 звезд3.5/5 (3)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsОт EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsРейтинг: 5 из 5 звезд5/5 (1)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeОт EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeРейтинг: 4.5 из 5 звезд4.5/5 (253)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.От EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Рейтинг: 4.5 из 5 звезд4.5/5 (110)
- Why We Die: The New Science of Aging and the Quest for ImmortalityОт EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityРейтинг: 4 из 5 звезд4/5 (5)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisОт EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisРейтинг: 4 из 5 звезд4/5 (1)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryОт EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryРейтинг: 4 из 5 звезд4/5 (45)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsОт EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsРейтинг: 4.5 из 5 звезд4.5/5 (170)
- Summary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedОт EverandSummary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedРейтинг: 4 из 5 звезд4/5 (61)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesОт EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesРейтинг: 4.5 из 5 звезд4.5/5 (1412)
- How to ADHD: The Ultimate Guide and Strategies for Productivity and Well-BeingОт EverandHow to ADHD: The Ultimate Guide and Strategies for Productivity and Well-BeingРейтинг: 1 из 5 звезд1/5 (1)
- The Marshmallow Test: Mastering Self-ControlОт EverandThe Marshmallow Test: Mastering Self-ControlРейтинг: 4.5 из 5 звезд4.5/5 (59)