Вам также может понравиться
- Ranula Management: Suggested Modifications in The Micro-Marsupialization TechniqueДокумент3 страницыRanula Management: Suggested Modifications in The Micro-Marsupialization Techniquemehak malhotraОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Management Surgery of The Oral and Maxillofacial Patient With End-Stage Renal DiseaseДокумент6 страницManagement Surgery of The Oral and Maxillofacial Patient With End-Stage Renal Diseasemehak malhotraОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Letter To The Editor: Int. J. Oral Maxillofac. Surg. 2018 XXX: XXX-XXXДокумент2 страницыLetter To The Editor: Int. J. Oral Maxillofac. Surg. 2018 XXX: XXX-XXXmehak malhotraОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Surgical Options in Oroantral Fistula Management: A Narrative ReviewДокумент13 страницSurgical Options in Oroantral Fistula Management: A Narrative Reviewmehak malhotraОценок пока нет
- Meniscopexy For Internal Derangement of Temporomandibular JointДокумент5 страницMeniscopexy For Internal Derangement of Temporomandibular Jointmehak malhotraОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Comparative Evaluation of Various Miniplate Systems For The Repair of Mandibular Corpus FracturesДокумент5 страницComparative Evaluation of Various Miniplate Systems For The Repair of Mandibular Corpus Fracturesmehak malhotraОценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Controversiesin Dentoalveolarand Preprostheticsurgery: Deepak G. KrishnanДокумент8 страницControversiesin Dentoalveolarand Preprostheticsurgery: Deepak G. Krishnanmehak malhotraОценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- 10 1016@j Coms 2018 06 003 PDFДокумент10 страниц10 1016@j Coms 2018 06 003 PDFmehak malhotraОценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Commentary: Distraction Osteogenesis Versus Orthognathic SurgeryДокумент3 страницыCommentary: Distraction Osteogenesis Versus Orthognathic Surgerymehak malhotraОценок пока нет
- Guidelines For Single-Stage Correction of TMJ Ankylosis, Facial Asymmetry and OSA in AdultsДокумент9 страницGuidelines For Single-Stage Correction of TMJ Ankylosis, Facial Asymmetry and OSA in Adultsmehak malhotraОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Ranula Decompression Using Stitch and Stab Method: The Aluko TechniqueДокумент5 страницRanula Decompression Using Stitch and Stab Method: The Aluko Techniquemehak malhotraОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- New Protocol To Prevent TMJ Reankylosis and Potentially Life Threatening Complications in Triad PatientsДокумент6 страницNew Protocol To Prevent TMJ Reankylosis and Potentially Life Threatening Complications in Triad Patientsmehak malhotraОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Al Moraissi2016Документ32 страницыAl Moraissi2016mehak malhotraОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Pernambuco Index: Predictability of The Complexity of Surgery For Impacted Lower Third MolarsДокумент7 страницPernambuco Index: Predictability of The Complexity of Surgery For Impacted Lower Third Molarsmehak malhotraОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Maxillomandibular Advancement: The Canadian ExperienceДокумент6 страницMaxillomandibular Advancement: The Canadian Experiencemehak malhotraОценок пока нет
- Kumari 2017Документ34 страницыKumari 2017mehak malhotraОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- 10 1016@j Cxom 2018 11 006Документ10 страниц10 1016@j Cxom 2018 11 006mehak malhotraОценок пока нет
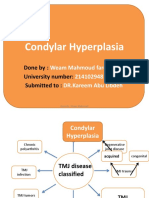
- Condylar Hyperplasia: Done By: University Number: Submitted ToДокумент69 страницCondylar Hyperplasia: Done By: University Number: Submitted Tomehak malhotraОценок пока нет
- What Is Suturing?: - The Primary Objective Is To Position andДокумент16 страницWhat Is Suturing?: - The Primary Objective Is To Position andmehak malhotraОценок пока нет
- Abdulmajeed Al Mogbel : Teaching Assistant, College of Dentistry, Qassim UniversityДокумент75 страницAbdulmajeed Al Mogbel : Teaching Assistant, College of Dentistry, Qassim Universitymehak malhotraОценок пока нет
- Pillai2016 PDFДокумент35 страницPillai2016 PDFmehak malhotraОценок пока нет
- The Use of The Buccal Fat Pad Flap For Oral Reconstruction: Review Open AccessДокумент9 страницThe Use of The Buccal Fat Pad Flap For Oral Reconstruction: Review Open Accessmehak malhotraОценок пока нет
- Maxillofacial Prosthetics Part-1 A Revie PDFДокумент10 страницMaxillofacial Prosthetics Part-1 A Revie PDFmehak malhotraОценок пока нет
- Injectableagentsversus Surgeryforrecurrent Temporomandibularjoint DislocationДокумент7 страницInjectableagentsversus Surgeryforrecurrent Temporomandibularjoint Dislocationmehak malhotraОценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Fibrinogen - A Practical and Cost Efficient BiomarДокумент6 страницFibrinogen - A Practical and Cost Efficient Biomarmehak malhotraОценок пока нет
- Malamed Local Anesthesia - 1Документ100 страницMalamed Local Anesthesia - 1Ines delacroix33% (3)
- Management of HIVHepatitis Patients in Oral and Maxillofacial SurgeryДокумент6 страницManagement of HIVHepatitis Patients in Oral and Maxillofacial Surgerymehak malhotraОценок пока нет
- Aramentarium For Minor Oral Surgical Procedure: Deepthi P.R. Intern Dept. of Oral SurgeryДокумент80 страницAramentarium For Minor Oral Surgical Procedure: Deepthi P.R. Intern Dept. of Oral Surgerymehak malhotraОценок пока нет
- Fortis AnalysisДокумент27 страницFortis Analysisrahul kОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Anatomy of A Case Write-Up DIДокумент2 страницыAnatomy of A Case Write-Up DIandrew powersОценок пока нет
- Pyoderma Gangrenosum A Review of Orthopedic Case ReportsДокумент4 страницыPyoderma Gangrenosum A Review of Orthopedic Case ReportsIga Nurwani RidwanОценок пока нет
- Risk and HazardДокумент22 страницыRisk and HazardRamirJanice Gulle MonjeОценок пока нет
- Life After Cancer: A Guide For Cancer SurvivorsДокумент88 страницLife After Cancer: A Guide For Cancer SurvivorsjeniferthuyОценок пока нет
- Evidence-Based Research:: "Spinal Cord Injury"Документ4 страницыEvidence-Based Research:: "Spinal Cord Injury"Jillian Danielle GalvezОценок пока нет
- Abcdefg1983 PDFДокумент769 страницAbcdefg1983 PDFmohОценок пока нет
- Newborn CompetencyДокумент3 страницыNewborn CompetencyJem Tellain100% (1)
- Investigation of An EpidemicДокумент26 страницInvestigation of An Epidemicnasnas18080Оценок пока нет
- Medical Surgical Nursing Module 12Документ45 страницMedical Surgical Nursing Module 12weissОценок пока нет
- Health Psychology: Bio Psychosocial Perspective: Ranya Al-Mandawi Dr. Tyrin Stevenson Psych 331Документ6 страницHealth Psychology: Bio Psychosocial Perspective: Ranya Al-Mandawi Dr. Tyrin Stevenson Psych 331Ranya NajiОценок пока нет
- Coping With Addiction: 6 Dysfunctional Family RolesДокумент4 страницыCoping With Addiction: 6 Dysfunctional Family RolesMy LaneОценок пока нет
- Geriatric NeuropsychДокумент480 страницGeriatric NeuropsychSergio García100% (2)
- CPG AID - Pocket Guide.v7 PDFДокумент31 страницаCPG AID - Pocket Guide.v7 PDFR ParkОценок пока нет
- Report AyendeДокумент13 страницReport AyendeAbubakar RabiuОценок пока нет
- 10 Tips For HospitalsДокумент2 страницы10 Tips For HospitalsVasu KodagantiОценок пока нет
- WHO Surgical Safety ChecklistДокумент1 страницаWHO Surgical Safety ChecklistArabelle GO100% (1)
- Surehands LMNДокумент1 страницаSurehands LMNapi-383151067Оценок пока нет
- Seminar Desiminasi NicuДокумент15 страницSeminar Desiminasi Niculina solihanОценок пока нет
- 504 Morocco Fact SheetsДокумент3 страницы504 Morocco Fact Sheetsopiakelvin2017Оценок пока нет
- Oleh: Kurnia Hernolingga 12-051 Preseptor: Dr. Dessy Wimelda, Sp. RadДокумент15 страницOleh: Kurnia Hernolingga 12-051 Preseptor: Dr. Dessy Wimelda, Sp. Radkurnia hernolinggaОценок пока нет
- Early OrthodonticsДокумент43 страницыEarly Orthodonticsdentistpro.org100% (1)
- Rabies 170502083951Документ17 страницRabies 170502083951dr shravaniОценок пока нет
- Tujuan Pembelajaran: Asking - Filling in Medical ReportДокумент8 страницTujuan Pembelajaran: Asking - Filling in Medical ReportNesi AgustiaОценок пока нет
- FSPR Masalunga1Документ34 страницыFSPR Masalunga1Janela CaballesОценок пока нет
- Drug Study On Labor and DeliveryДокумент4 страницыDrug Study On Labor and DeliveryJune Dumdumaya67% (3)
- Advanced Physiotherapeutic SyllabusДокумент1 страницаAdvanced Physiotherapeutic SyllabusAnup SharmaОценок пока нет
- Ms Question 1Документ33 страницыMs Question 1yra capiliОценок пока нет
- Current Perspectives On Pharmacist Home Visits: Do We Keep Reinventing The Wheel?Документ19 страницCurrent Perspectives On Pharmacist Home Visits: Do We Keep Reinventing The Wheel?200742 Elya AmaliaОценок пока нет
- The Wisdom of Plagues: Lessons from 25 Years of Covering PandemicsОт EverandThe Wisdom of Plagues: Lessons from 25 Years of Covering PandemicsРейтинг: 4.5 из 5 звезд4.5/5 (6)
- Uncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicОт EverandUncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicОценок пока нет
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisОт EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisРейтинг: 4 из 5 звезд4/5 (9)
- Profiles of the Vaccine-Injured: "A Lifetime Price to Pay"От EverandProfiles of the Vaccine-Injured: "A Lifetime Price to Pay"Рейтинг: 3.5 из 5 звезд3.5/5 (3)
- Do You Believe in Magic?: The Sense and Nonsense of Alternative MedicineОт EverandDo You Believe in Magic?: The Sense and Nonsense of Alternative MedicineОценок пока нет