Вам также может понравиться
- CohotДокумент14 страницCohotMadyline VictoryaОценок пока нет
- AP MR GlossaryДокумент5 страницAP MR GlossaryReynaldi HadiwijayaОценок пока нет
- Adosex 1Документ52 страницыAdosex 1Madyline VictoryaОценок пока нет
- Secrets to Long Life Revealed in Blue ZonesДокумент10 страницSecrets to Long Life Revealed in Blue ZonesMadyline VictoryaОценок пока нет
- Jadwal Piket Perawat Rawat IanapДокумент18 страницJadwal Piket Perawat Rawat IanapMadyline Victorya100% (1)
- SpiritualityДокумент82 страницыSpiritualityMadyline VictoryaОценок пока нет
- KKR - 8 Mei 2014Документ2 страницыKKR - 8 Mei 2014Madyline VictoryaОценок пока нет
- 455657Документ2 страницы455657Madyline VictoryaОценок пока нет
- Age Ageing-2013 - I1-I57Документ57 страницAge Ageing-2013 - I1-I57Madyline VictoryaОценок пока нет
- Gizi SeimbangДокумент54 страницыGizi SeimbangMarliana PohanОценок пока нет
- Paincontrol PDFДокумент52 страницыPaincontrol PDFMadyline VictoryaОценок пока нет
- Standards of Good Practice For Spinal Interventional ProceduresДокумент20 страницStandards of Good Practice For Spinal Interventional ProceduresMadyline VictoryaОценок пока нет
- SOFA Score Describes Organ DysfunctionДокумент4 страницыSOFA Score Describes Organ DysfunctionMadyline VictoryaОценок пока нет
- 2006 8215Документ86 страниц2006 8215Madyline VictoryaОценок пока нет
- Journal ReadingДокумент23 страницыJournal ReadingMadyline VictoryaОценок пока нет
- NelsonДокумент1 страницаNelsonMadyline VictoryaОценок пока нет
- Referat RadiologiДокумент6 страницReferat RadiologiMadyline VictoryaОценок пока нет
- Anestesi and FESSДокумент6 страницAnestesi and FESSMadyline VictoryaОценок пока нет
- Basic Life SupportДокумент12 страницBasic Life SupportMadyline VictoryaОценок пока нет
- EmpyemaДокумент27 страницEmpyemaMadyline VictoryaОценок пока нет
- Secrets to Long Life Revealed in Blue ZonesДокумент10 страницSecrets to Long Life Revealed in Blue ZonesMadyline VictoryaОценок пока нет
- Ectopic PregnancyДокумент16 страницEctopic PregnancyMadyline VictoryaОценок пока нет
- Standards of Good Practice For Spinal Interventional ProceduresДокумент20 страницStandards of Good Practice For Spinal Interventional ProceduresMadyline VictoryaОценок пока нет
- Obstetric Abdominal ExaminationДокумент32 страницыObstetric Abdominal ExaminationMadyline VictoryaОценок пока нет
- Hasil Kontrol LisaДокумент2 страницыHasil Kontrol LisaMadyline VictoryaОценок пока нет
- Pub Prof EpiduralAnalgesia2010Документ14 страницPub Prof EpiduralAnalgesia2010Madyline VictoryaОценок пока нет
- Socialism CapitalismДокумент268 страницSocialism CapitalismRobert PattonОценок пока нет
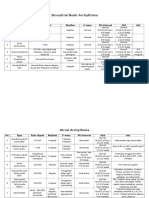
- Sinoatrial Node Arrhythmia: No Type Rate (BPM) Rhythm P Wave PR Interval ORS KetДокумент3 страницыSinoatrial Node Arrhythmia: No Type Rate (BPM) Rhythm P Wave PR Interval ORS KetMadyline VictoryaОценок пока нет
- Cardiology Research EvaluationДокумент6 страницCardiology Research EvaluationMadyline VictoryaОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- The Relationship Between Nurses Work HoursДокумент31 страницаThe Relationship Between Nurses Work HoursZaty ChaiyOkkОценок пока нет
- Majority of ailments in India more acute than chronic due to poor sanitationДокумент49 страницMajority of ailments in India more acute than chronic due to poor sanitationChristina HarmonОценок пока нет
- 藥理表格Документ26 страниц藥理表格林盈孜Оценок пока нет
- Formularium Obat RSДокумент2 страницыFormularium Obat RSMyzard AriefОценок пока нет
- Laporan Triwulan 2Документ87 страницLaporan Triwulan 2Nanda HotmanОценок пока нет
- Bipolar Brochure English FINAL 150109 PDFДокумент9 страницBipolar Brochure English FINAL 150109 PDFIka M. HendrajayaОценок пока нет
- SedativeДокумент35 страницSedativeking_goldОценок пока нет
- 1 Exercise ERD 1Документ2 страницы1 Exercise ERD 1Yashil Yudhisthir BhurtunОценок пока нет
- Top 10 Pharmaceutical Companies in IndiaДокумент2 страницыTop 10 Pharmaceutical Companies in Indiamerchantblue9Оценок пока нет
- Sleep: Sleep Can Be Defined As A Normal State of Altered Consciousness DuringДокумент17 страницSleep: Sleep Can Be Defined As A Normal State of Altered Consciousness DuringappuvayalaОценок пока нет
- Nettle Rash Symptoms, Causes, TreatmentДокумент2 страницыNettle Rash Symptoms, Causes, TreatmentArdave Laurente100% (1)
- Eth and Ice: TweakДокумент24 страницыEth and Ice: TweakJustin Ellingsen0% (1)
- AmsterdamLiquidXno1 vendor profile and product listДокумент11 страницAmsterdamLiquidXno1 vendor profile and product listArrush AhujaОценок пока нет
- SimvastatinДокумент1 страницаSimvastatinLyka Mae Imbat - PacnisОценок пока нет
- Disjoined 1S1EДокумент12 страницDisjoined 1S1EArthur CarvalhoОценок пока нет
- Usfda-Generic Drug User Fee Act - A Complete ReviewДокумент15 страницUsfda-Generic Drug User Fee Act - A Complete ReviewijsidonlineinfoОценок пока нет
- Observation Report - Hemodialysis - Kit P. RoaquinДокумент15 страницObservation Report - Hemodialysis - Kit P. Roaquineljhayar_18Оценок пока нет
- Medical Assistant Study Guide PDFДокумент116 страницMedical Assistant Study Guide PDFFelishaBassettОценок пока нет
- Causes, Symptoms and Treatments of VaginitisДокумент16 страницCauses, Symptoms and Treatments of VaginitisMae Christelle Hamoy100% (2)
- How To Switch Insulin Products - Pharm LetterДокумент6 страницHow To Switch Insulin Products - Pharm LetterAraceli LeonОценок пока нет
- Drug StudyДокумент8 страницDrug StudyRizzi DeveraОценок пока нет
- Amlodipine Side EffectsДокумент6 страницAmlodipine Side Effects1976gt500Оценок пока нет
- Epic TutДокумент15 страницEpic TutTorgbui Gorni Treve IV100% (2)
- LamotrigineДокумент109 страницLamotriginemunzirОценок пока нет
- Aseptic TechniquesДокумент6 страницAseptic TechniquesAinun MokhtarОценок пока нет
- Medcorps Patient FormДокумент7 страницMedcorps Patient Formapi-3609449100% (1)
- HRPB Drug Formulary 2018Документ244 страницыHRPB Drug Formulary 2018tiuwangОценок пока нет
- Manu ManualДокумент2 страницыManu ManualJatrice Bianca Dela PazОценок пока нет
- Exploratory Essay-2Документ8 страницExploratory Essay-2api-242478717Оценок пока нет
- Data Obat EthicalДокумент6 страницData Obat EthicalHarrys FadillahОценок пока нет