Вам также может понравиться
- Physical ExaminationДокумент55 страницPhysical Examinationdakshpanchal26369Оценок пока нет
- A&P 302 - Respiratory NotesДокумент31 страницаA&P 302 - Respiratory NotesBethanyОценок пока нет
- ANPH-M2-CU8. The HeartДокумент20 страницANPH-M2-CU8. The HeartMary Grace MapulaОценок пока нет
- Chapter 15 - Cardiovascular SystemДокумент89 страницChapter 15 - Cardiovascular SystemOliver Namyalo100% (1)
- Introduction To Cell PhysiologyДокумент149 страницIntroduction To Cell PhysiologyAlysaОценок пока нет
- Cardiovascular SystemДокумент58 страницCardiovascular Systemsultan khabeebОценок пока нет
- CH 11 Heart NotesДокумент2 страницыCH 11 Heart Notesummnicole0% (1)
- Physiology notes on cardiac muscle and the heart's conductive systemДокумент37 страницPhysiology notes on cardiac muscle and the heart's conductive systemDany SamuelОценок пока нет
- Asthma Triggers, Symptoms, Diagnosis & Treatment GuideДокумент10 страницAsthma Triggers, Symptoms, Diagnosis & Treatment GuideRem AlfelorОценок пока нет
- Skeletal Muscle Contraction MechanismДокумент10 страницSkeletal Muscle Contraction MechanismLiljana StojkovicОценок пока нет
- Head To Toe Checklist (Masroni)Документ13 страницHead To Toe Checklist (Masroni)hillary elsaОценок пока нет
- RBC Physiology and Blood TypingДокумент3 страницыRBC Physiology and Blood TypingGabrielle SerranoОценок пока нет
- Bleeding Disorders 1 - DR - Kamal MokbelДокумент13 страницBleeding Disorders 1 - DR - Kamal MokbelRawan E. SaeedОценок пока нет
- Anatomy and Physiology MnemonicsДокумент7 страницAnatomy and Physiology MnemonicsLalajimОценок пока нет
- Properties of Cardiac Muscle and Conducting SystemsДокумент38 страницProperties of Cardiac Muscle and Conducting Systemsnirilib100% (4)
- Expanded 3P Study Guide YasminaIrinaДокумент79 страницExpanded 3P Study Guide YasminaIrinaikОценок пока нет
- Hemodynamics: DR Axelle Saverettiar Mbbs Physiology Department SSR Medical CollegeДокумент31 страницаHemodynamics: DR Axelle Saverettiar Mbbs Physiology Department SSR Medical CollegeÑäd ÉèmОценок пока нет
- Mediastinum and Its ContentsДокумент11 страницMediastinum and Its ContentsPap YeeОценок пока нет
- The Cardiac Cycle: Chapter 19Документ62 страницыThe Cardiac Cycle: Chapter 19BishwambherОценок пока нет
- Lec - 1H - Special Senses System ReviewerДокумент18 страницLec - 1H - Special Senses System ReviewerProfessor GhoulОценок пока нет
- Abdominal Trauma: Fatin Amirah KamaruddinДокумент29 страницAbdominal Trauma: Fatin Amirah Kamaruddinvirz23Оценок пока нет
- Clinical Examination of CVSДокумент33 страницыClinical Examination of CVSmahnoorОценок пока нет
- 4 Apr - Bleeding DisordersДокумент50 страниц4 Apr - Bleeding DisordersAhmed SarfarazОценок пока нет
- 3-Major Veins of The BodyДокумент26 страниц3-Major Veins of The BodyTJPlayz100% (1)
- Pulmonary Diseases - Dental ManagementДокумент45 страницPulmonary Diseases - Dental Managementfilyouth4life100% (3)
- Heart Muscles, Valves & Blood Vessels (I)Документ31 страницаHeart Muscles, Valves & Blood Vessels (I)Hussain GauharОценок пока нет
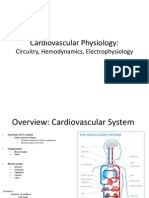
- Cardiovascular Physiology:: Circuitry, Hemodynamics, ElectrophysiologyДокумент27 страницCardiovascular Physiology:: Circuitry, Hemodynamics, Electrophysiologyrsmoney3Оценок пока нет
- Cardiovascular Physiology 4 - Gomez MD PDFДокумент65 страницCardiovascular Physiology 4 - Gomez MD PDFMelissa SalayogОценок пока нет
- LSM3212 - Lecture 2-4 BloodДокумент59 страницLSM3212 - Lecture 2-4 BloodAbraham KangОценок пока нет
- 2 - Renal PhysiologyДокумент8 страниц2 - Renal PhysiologyKunware TropaОценок пока нет
- HEENT Cheat SheetДокумент22 страницыHEENT Cheat SheetKatrina FeriОценок пока нет
- Urinary SystemДокумент9 страницUrinary SystemCUESCANO, CRISTEL G. BSMT 2-AОценок пока нет
- Cardiac Exam Guide: Inspection, Palpation, AuscultationДокумент23 страницыCardiac Exam Guide: Inspection, Palpation, AuscultationAreza Eka PermanaОценок пока нет
- Shock: Rose Ann J. Raquiza-Perante Post Graduate InternДокумент53 страницыShock: Rose Ann J. Raquiza-Perante Post Graduate InternRose Ann RaquizaОценок пока нет
- Y2 Met Lecture Revision NotesДокумент69 страницY2 Met Lecture Revision NotesHelen VlotomasОценок пока нет
- Cardiac Physical Exam Guide by Prof. TorresДокумент29 страницCardiac Physical Exam Guide by Prof. TorresrubyОценок пока нет
- Lab Physiology Second Year PracticalДокумент21 страницаLab Physiology Second Year PracticalNona NonicaaОценок пока нет
- Classification of MurmursДокумент2 страницыClassification of MurmursNazneen SiddiquiОценок пока нет
- Physiology of Heart in DetailДокумент101 страницаPhysiology of Heart in Detailakanksha sharmaОценок пока нет
- Heart Muscle: The Heart As A Pump and FunctionДокумент4 страницыHeart Muscle: The Heart As A Pump and Functionmcwnotes100% (1)
- Neuroscience I - Neurologic History Taking and Examination (POBLETE)Документ9 страницNeuroscience I - Neurologic History Taking and Examination (POBLETE)Johanna Hamnia PobleteОценок пока нет
- RBC Formation, Anemia, WBC FunctionДокумент28 страницRBC Formation, Anemia, WBC FunctionlifecostОценок пока нет
- Diagn Approach of Abdominal PainДокумент53 страницыDiagn Approach of Abdominal PainNuriОценок пока нет
- CSF Protection & Flow of the BrainДокумент25 страницCSF Protection & Flow of the BrainchintyamontangОценок пока нет
- Lecture 3. Bleeding Disorders Part 1Документ31 страницаLecture 3. Bleeding Disorders Part 1Kekelwa Mutumwenu Snr100% (1)
- Propagation of Nerve ImpulseДокумент42 страницыPropagation of Nerve ImpulseRe UpОценок пока нет
- Cardio AuscultationДокумент19 страницCardio AuscultationshadabОценок пока нет
- REVISED Head InjuryДокумент4 страницыREVISED Head InjuryJanselle H Arma0% (1)
- Anes Preoperative-AssessmentДокумент6 страницAnes Preoperative-AssessmentChristine Mendoza100% (1)
- Cardiac InvestigationsДокумент17 страницCardiac InvestigationsTARIQ100% (1)
- PencernaanДокумент39 страницPencernaanVina Zavira NizarОценок пока нет
- MED (Neuro) - NeuroanatomyДокумент6 страницMED (Neuro) - NeuroanatomyFlora XuОценок пока нет
- 24 Cerebral Blood FlowДокумент31 страница24 Cerebral Blood FlowZuhaib Ahmed100% (1)
- Nervous System and Special Senses OverviewДокумент90 страницNervous System and Special Senses Overviewjayc lopezОценок пока нет
- Amphibian Graphs?Документ9 страницAmphibian Graphs?Anshumaan PatraОценок пока нет
- Causes Obstruction Causes CSF To Build Up in The Brain. If The Cause Is Congenital, Symptoms Such As AnДокумент22 страницыCauses Obstruction Causes CSF To Build Up in The Brain. If The Cause Is Congenital, Symptoms Such As Anmhelandie100% (1)
- OSCE Chart Cough (KK)Документ4 страницыOSCE Chart Cough (KK)api-26938624Оценок пока нет
- Endo 3 Notes PDFДокумент9 страницEndo 3 Notes PDFDilОценок пока нет
- Problem-based Approach to Gastroenterology and HepatologyОт EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisОценок пока нет
- Sexual Harassment Act FMCH April 2017Документ29 страницSexual Harassment Act FMCH April 2017Dranreb Berylle MasangkayОценок пока нет
- SCREEM (Divina) resources pathology planДокумент2 страницыSCREEM (Divina) resources pathology planDranreb Berylle MasangkayОценок пока нет
- Pathology 4.05 Liver Pathology - Dr. YanezДокумент22 страницыPathology 4.05 Liver Pathology - Dr. YanezDranreb Berylle MasangkayОценок пока нет
- Community-Acquired Pneumonia - CPG 2016Документ26 страницCommunity-Acquired Pneumonia - CPG 2016Jamie SebastianОценок пока нет
- Pathology 5.05b Vagina and Vulva - DR - Dy (Final Edit)Документ11 страницPathology 5.05b Vagina and Vulva - DR - Dy (Final Edit)Dranreb Berylle MasangkayОценок пока нет
- What Is The Diagnosis? 2. Give The Basis For Your Diagnosis and Criteria For Your Diagnosis? SymptomsДокумент1 страницаWhat Is The Diagnosis? 2. Give The Basis For Your Diagnosis and Criteria For Your Diagnosis? SymptomsDranreb Berylle MasangkayОценок пока нет
- C N L Part 1 - Diseases and Chest Pain TablesДокумент3 страницыC N L Part 1 - Diseases and Chest Pain TablesDranreb Berylle MasangkayОценок пока нет
- Pathology 5.05a CervixДокумент6 страницPathology 5.05a CervixDranreb Berylle MasangkayОценок пока нет
- Non-Pharmacological Treatment Lifestyle ModificationsДокумент6 страницNon-Pharmacological Treatment Lifestyle ModificationsDranreb Berylle MasangkayОценок пока нет
- Pathology 4.05 Liver Pathology - Dr. YanezДокумент22 страницыPathology 4.05 Liver Pathology - Dr. YanezDranreb Berylle MasangkayОценок пока нет
- Sexually Transmitted Diseases de VeraДокумент50 страницSexually Transmitted Diseases de VeraDranreb Berylle MasangkayОценок пока нет
- C N L Part 1 - Diseases and Chest Pain TablesДокумент3 страницыC N L Part 1 - Diseases and Chest Pain TablesDranreb Berylle MasangkayОценок пока нет
- Stroke PDFДокумент106 страницStroke PDFDranreb Berylle MasangkayОценок пока нет
- Community Survey ToolДокумент10 страницCommunity Survey ToolDranreb Berylle MasangkayОценок пока нет
- RepairДокумент48 страницRepairDranreb Berylle MasangkayОценок пока нет
- Family Structure, Characteristics and DynamicsДокумент6 страницFamily Structure, Characteristics and DynamicsErilyn Leigh ManaloОценок пока нет
- Malabsorptive DiarrheaДокумент3 страницыMalabsorptive DiarrheaDranreb Berylle MasangkayОценок пока нет
- EYE PATHOLOGIES REVEALEDДокумент11 страницEYE PATHOLOGIES REVEALEDDranreb Berylle MasangkayОценок пока нет
- CSTДокумент36 страницCSTDranreb Berylle MasangkayОценок пока нет
- Family Structure, Characteristics and DynamicsДокумент6 страницFamily Structure, Characteristics and DynamicsErilyn Leigh ManaloОценок пока нет
- Family Structure, Characteristics and DynamicsДокумент6 страницFamily Structure, Characteristics and DynamicsErilyn Leigh ManaloОценок пока нет
- 1malabsorption SyndromeДокумент6 страниц1malabsorption SyndromeDranreb Berylle MasangkayОценок пока нет
- Malabsorption: Exocrine Pancreatic InsufficiencyДокумент6 страницMalabsorption: Exocrine Pancreatic InsufficiencyDranreb Berylle MasangkayОценок пока нет
- CSTДокумент36 страницCSTDranreb Berylle MasangkayОценок пока нет
- CSTДокумент36 страницCSTDranreb Berylle MasangkayОценок пока нет
- Malabsorptive DiarrheaДокумент3 страницыMalabsorptive DiarrheaDranreb Berylle MasangkayОценок пока нет
- Community Assessment Tools: A Companion Piece To Communities in ActionДокумент12 страницCommunity Assessment Tools: A Companion Piece To Communities in ActionDranreb Berylle MasangkayОценок пока нет
- Diarrhea (Autosaved)Документ3 страницыDiarrhea (Autosaved)Dranreb Berylle MasangkayОценок пока нет
- Inflammatory Bowel DiseaseДокумент19 страницInflammatory Bowel DiseaseDranreb Berylle MasangkayОценок пока нет
- Infinium OMNI Express Patient Monitor ManualДокумент41 страницаInfinium OMNI Express Patient Monitor ManualCarl AzzopardiОценок пока нет
- English M8102-9441AДокумент40 страницEnglish M8102-9441ABong Kek ChiewОценок пока нет
- Tibetan Medicine: The Three ElementsДокумент28 страницTibetan Medicine: The Three ElementshonetzugiОценок пока нет
- BPBIO750 Catalogue EngДокумент2 страницыBPBIO750 Catalogue EngLouis LОценок пока нет
- Physical Assessment Findings for Nursing StudentДокумент19 страницPhysical Assessment Findings for Nursing StudentJanОценок пока нет
- Notes On Physical Examination of AbdomenДокумент6 страницNotes On Physical Examination of AbdomenMarwa Al-AzzawiОценок пока нет
- Unit 10-Basic Nursing SkillsДокумент104 страницыUnit 10-Basic Nursing Skillsshenric16Оценок пока нет
- A Spectrum of Doppler Waveforms in The Carotid and Vertebral ArteriesДокумент17 страницA Spectrum of Doppler Waveforms in The Carotid and Vertebral ArteriesDewintha Airene NoviantiОценок пока нет
- Skills Lab QuestionДокумент3 страницыSkills Lab QuestionRIBO, DELОценок пока нет
- Outcomes Upper Intermediate Vocabulary BuilderДокумент76 страницOutcomes Upper Intermediate Vocabulary Buildermavr7680% (5)
- Definition of Physical EducationДокумент8 страницDefinition of Physical EducationAkhilesh Jain100% (2)
- System Exam SummaryДокумент4 страницыSystem Exam Summaryespo176Оценок пока нет
- June Nle 2009 SRG Final CoachingДокумент31 страницаJune Nle 2009 SRG Final CoachingChoki Momoki100% (1)
- Health Assessment Lecture: - Review About THE Respiratory SystemДокумент8 страницHealth Assessment Lecture: - Review About THE Respiratory SystemHОценок пока нет
- Case Presentation: Patient Chart - Mary JohnsonДокумент12 страницCase Presentation: Patient Chart - Mary Johnsonivoneeh_16100% (1)
- MEDICAL PHYSICAL DIAGNOSISДокумент4 страницыMEDICAL PHYSICAL DIAGNOSISMonique BorresОценок пока нет
- Danger Signs of LaborДокумент13 страницDanger Signs of LaborBenj Villanueva50% (2)
- Patient'S Peripheral Arterial Disease Risk FactorsДокумент2 страницыPatient'S Peripheral Arterial Disease Risk FactorsKrystel BatinoОценок пока нет
- Monitoring Vital SignsДокумент23 страницыMonitoring Vital SignsDefina 17Оценок пока нет
- CVA Case StudyДокумент4 страницыCVA Case Studynbk08Оценок пока нет
- Fundamentals of Cardiology For The USMLE and General Medics PDFДокумент287 страницFundamentals of Cardiology For The USMLE and General Medics PDFCharles Vindo100% (2)
- Nellcor N-65 Pulse Oximeter - Service ManualДокумент118 страницNellcor N-65 Pulse Oximeter - Service ManualDaniel Hernan Rengifo GiraldoОценок пока нет
- CNA Abbreviations & VocabularyДокумент8 страницCNA Abbreviations & VocabularyLie Adi Darmawan100% (2)
- Mobil-O-Graph PWA Brochure PDFДокумент1 страницаMobil-O-Graph PWA Brochure PDFhyde93Оценок пока нет
- Associations of Arterial Stiffness With Some Cardiovascular Complications in The HypertensivesДокумент12 страницAssociations of Arterial Stiffness With Some Cardiovascular Complications in The HypertensivesLê HoangОценок пока нет
- Table Respiration RateДокумент1 страницаTable Respiration Ratereal_septiady_madrid3532Оценок пока нет
- Assessing The Thorax and LungsДокумент4 страницыAssessing The Thorax and LungsLorenz Jude Cańete100% (2)
- Skills - Masuring Apical - Radial PulseДокумент1 страницаSkills - Masuring Apical - Radial PulseJoanna Mae Movido CarolinoОценок пока нет
- What Is Patient Monitoring Equipment PDFДокумент2 страницыWhat Is Patient Monitoring Equipment PDFAMEY PILANKARОценок пока нет
- Classic Pulse Diagnosis PDFДокумент21 страницаClassic Pulse Diagnosis PDFDani TenaОценок пока нет