Вам также может понравиться
- 29 Anti-Viral Drugs PDFДокумент43 страницы29 Anti-Viral Drugs PDFabhishek talokarОценок пока нет
- Anti Viral and Antiretroviral Drugs: Presented byДокумент36 страницAnti Viral and Antiretroviral Drugs: Presented byshree devОценок пока нет
- AntifungalДокумент41 страницаAntifungalDeribe BekeleОценок пока нет
- Digitalis ToxicityДокумент55 страницDigitalis ToxicityBahaa Shaaban100% (1)
- Drugs Used in TuberculosisДокумент27 страницDrugs Used in Tuberculosisapi-3705123Оценок пока нет
- Clostridium BotulinumДокумент18 страницClostridium BotulinumPolinaОценок пока нет
- STDДокумент2 страницыSTDapocruОценок пока нет
- Uses of Inhaler DevicesДокумент39 страницUses of Inhaler Devicesluis_chubeeОценок пока нет
- Anti Protozoal AgentsДокумент19 страницAnti Protozoal AgentsNithish SОценок пока нет
- Oncology Nursing Oncology What Is Cancer? International IncidenceДокумент10 страницOncology Nursing Oncology What Is Cancer? International IncidenceNeweeJoonYowОценок пока нет
- Therapeutic Classification of DrugsДокумент35 страницTherapeutic Classification of DrugsJomarie Villalobos BuñoОценок пока нет
- Alcohol and Drug QuizДокумент6 страницAlcohol and Drug Quizapi-285898641Оценок пока нет
- In The Name of Allah, The Most Beneficent and MercifulДокумент35 страницIn The Name of Allah, The Most Beneficent and MercifulAhmedMenshawyОценок пока нет
- Pharma - SkinДокумент8 страницPharma - Skinreference books100% (1)
- NANDA DX NI, NOДокумент165 страницNANDA DX NI, NOKerry Brown100% (1)
- Introduction in Medical Microbiology June 2020 Online ClassДокумент9 страницIntroduction in Medical Microbiology June 2020 Online Classjames rukenyaОценок пока нет
- Review Questions On Antiviral and AntibioticДокумент63 страницыReview Questions On Antiviral and AntibioticusedforfunplocОценок пока нет
- Antifungal Drugs 3Документ54 страницыAntifungal Drugs 3Mikee MeladОценок пока нет
- Leukocytes White Blood CellsДокумент64 страницыLeukocytes White Blood CellsNevin BhunjunОценок пока нет
- Ncm107 Summarization of MCNДокумент40 страницNcm107 Summarization of MCNArlyn Faith AlvarezОценок пока нет
- Lecture 1, Introduction To Pharmacology (Script)Документ10 страницLecture 1, Introduction To Pharmacology (Script)JustDen09Оценок пока нет
- Drugs Affecting The Ear and Eye 2021Документ88 страницDrugs Affecting The Ear and Eye 2021renz bartolomeОценок пока нет
- Micro paraДокумент7 страницMicro paraAj MillanОценок пока нет
- Antiinflammatory Drugs: Toya AriawanДокумент27 страницAntiinflammatory Drugs: Toya Ariawanlast100% (1)
- Hygiene NotesДокумент60 страницHygiene NotesDuchess Juliane Jose MirambelОценок пока нет
- Infection Control QuestionsДокумент2 страницыInfection Control QuestionsNhor BasmalaОценок пока нет
- AlzheimersДокумент5 страницAlzheimersRonald Cszar Fabian VillanoОценок пока нет
- Pharmacology - Section 23 - Antibiotics 2Документ5 страницPharmacology - Section 23 - Antibiotics 2Pathalee ThalpavilaОценок пока нет
- Microbiology Pre Test 1Документ6 страницMicrobiology Pre Test 1thediaber100% (1)
- Medication Administration PDFДокумент47 страницMedication Administration PDFac caneОценок пока нет
- Intravenous TherapyДокумент10 страницIntravenous TherapyS. AmberОценок пока нет
- Riaz Gul AHN Unit 1Документ106 страницRiaz Gul AHN Unit 1Riaz Gul RindОценок пока нет
- Gastrointestinal DrugsДокумент2 страницыGastrointestinal DrugsJannah Mikhaela Alibay VillarinОценок пока нет
- Antifungal Drugs During PregnancyДокумент9 страницAntifungal Drugs During Pregnancy600WPMPOОценок пока нет
- XTRA Final PunchДокумент314 страницXTRA Final Punchsk100% (1)
- 001 Introduction To PharmacologyДокумент29 страниц001 Introduction To Pharmacologynancy alsharuОценок пока нет
- Drugs Acting On The Immune SystemДокумент33 страницыDrugs Acting On The Immune SystemAnonymous iG0DCOf100% (1)
- VaginitisДокумент16 страницVaginitisMae Christelle Hamoy100% (2)
- Acute Pesticide PoisoningДокумент46 страницAcute Pesticide PoisoningGiaToula54Оценок пока нет
- Funda DXДокумент8 страницFunda DXdhodejun lizhaldeОценок пока нет
- Antiviral DrugsДокумент6 страницAntiviral DrugsLori MoscaliucОценок пока нет
- Mathematical Fundamental in PharmacokineticДокумент21 страницаMathematical Fundamental in PharmacokineticErna PratiwiОценок пока нет
- Lectures1,2,3, 4 PDFДокумент127 страницLectures1,2,3, 4 PDFYasmin AbozeidОценок пока нет
- Duty Ob ExamДокумент3 страницыDuty Ob ExamKATHERINE GRACE JOSEОценок пока нет
- Medical Dan Surgical AsepsisДокумент49 страницMedical Dan Surgical AsepsisTahtawi 'Afid' Rifai RidhoОценок пока нет
- Chapter 11Документ23 страницыChapter 11Hannah BuquironОценок пока нет
- Prepared By: Mr. Val L. Ramilo RNДокумент65 страницPrepared By: Mr. Val L. Ramilo RNMilk CoОценок пока нет
- About 70% of All Sensory Information Reaches The Brain Through The EyesДокумент127 страницAbout 70% of All Sensory Information Reaches The Brain Through The Eyesjoan olanteОценок пока нет
- Health, Stress, and CopingДокумент43 страницыHealth, Stress, and CopingKar Gayee100% (1)
- Vaccination or ImmunizationДокумент4 страницыVaccination or ImmunizationPrincessОценок пока нет
- Oral Antibiotic Therapy For Acne Vulgaris PDFДокумент8 страницOral Antibiotic Therapy For Acne Vulgaris PDFEka Sulistyowati PОценок пока нет
- AUTOIMMUNEДокумент75 страницAUTOIMMUNEEva Boje-JugadorОценок пока нет
- InjectionsДокумент18 страницInjectionsNotInterestedОценок пока нет
- AntihistaminesДокумент66 страницAntihistaminesAfif Bastian100% (1)
- Unit#1principle of PharmacologyДокумент58 страницUnit#1principle of PharmacologySaima VictorОценок пока нет
- Epidemiology and Public HealthДокумент21 страницаEpidemiology and Public HealthFatima SumabatОценок пока нет
- PoisoningДокумент3 страницыPoisoningGenevie GabrielОценок пока нет
- Introduction To PharmacologyДокумент38 страницIntroduction To PharmacologyManglarapu Surya100% (1)
- Antiviral ChemotherapyДокумент59 страницAntiviral ChemotherapyDiriba feyisaОценок пока нет
- Antihsv-Vzv AgentsДокумент35 страницAntihsv-Vzv AgentsAulia Rahma NoviastutiОценок пока нет
- Vitamins Notes PDFДокумент3 страницыVitamins Notes PDFmiguel cuevas100% (1)
- Surgical Pathology Trans No 7. The LIVER DR ROXAS by MCD Recoverd 1Документ14 страницSurgical Pathology Trans No 7. The LIVER DR ROXAS by MCD Recoverd 1miguel cuevasОценок пока нет
- Pathology Final Practical ExaminationДокумент40 страницPathology Final Practical Examinationmiguel cuevasОценок пока нет
- Sex Determination and DifferentiationДокумент3 страницыSex Determination and Differentiationmiguel cuevasОценок пока нет
- Cytogenetics Disorders PDFДокумент7 страницCytogenetics Disorders PDFmiguel cuevasОценок пока нет
- Minerals SummaryДокумент2 страницыMinerals Summarymiguel cuevasОценок пока нет
- Male PhysiologyДокумент2 страницыMale Physiologymiguel cuevasОценок пока нет
- Histo Pracs - Respi and Brain PDFДокумент17 страницHisto Pracs - Respi and Brain PDFmiguel cuevasОценок пока нет
- (New) Drugs Used For Gastrointestinal DiseasesДокумент59 страниц(New) Drugs Used For Gastrointestinal Diseasesmiguel cuevasОценок пока нет
- Infectious Diseases - BacteriaДокумент9 страницInfectious Diseases - Bacteriamiguel cuevas100% (1)
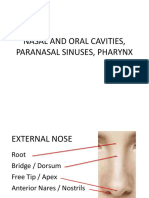
- Nasal and Oral Cavities, Paranasal Sinuses, PharynxДокумент112 страницNasal and Oral Cavities, Paranasal Sinuses, Pharynxmiguel cuevasОценок пока нет
- Diseases of The Peripheral Nervous SystemДокумент8 страницDiseases of The Peripheral Nervous Systemmiguel cuevasОценок пока нет
- First Aid: FM 4-25.11 NTRP 4-02.1 AFMAN 44-163 (I)Документ224 страницыFirst Aid: FM 4-25.11 NTRP 4-02.1 AFMAN 44-163 (I)Giuseppe TrovatoОценок пока нет
- Hypolipedemic AgentsДокумент9 страницHypolipedemic Agentsmiguel cuevasОценок пока нет
- RBC - Patho BДокумент129 страницRBC - Patho Bmiguel cuevasОценок пока нет
- 1 Patho5 - Kidney I 2015bДокумент10 страниц1 Patho5 - Kidney I 2015bmiguel cuevasОценок пока нет
- Anesthesia - Dr. FirmalinoДокумент14 страницAnesthesia - Dr. Firmalinomiguel cuevasОценок пока нет
- 1.18 MycobacteriumДокумент6 страниц1.18 Mycobacteriummiguel cuevasОценок пока нет
- Glycogenolysis and GlycogenesisДокумент11 страницGlycogenolysis and Glycogenesismiguel cuevas100% (2)
- Female PathologyДокумент16 страницFemale Pathologymiguel cuevasОценок пока нет
- CHF and Diuretics Trans Limpin MissionДокумент12 страницCHF and Diuretics Trans Limpin Missionmiguel cuevasОценок пока нет
- Breast PathologyДокумент27 страницBreast Pathologymiguel cuevasОценок пока нет
- Anti-Psychotic NewestДокумент118 страницAnti-Psychotic Newestmiguel cuevasОценок пока нет
- He Ma To PoiesisДокумент98 страницHe Ma To Poiesismiguel cuevasОценок пока нет
- Cell Cycle, Apoptosis, and CancerДокумент13 страницCell Cycle, Apoptosis, and Cancermiguel cuevas100% (1)
- Microbiology Lecture 8 & 9 - Systemic & Opportunistic Mycoses (Raroromiki Trans)Документ3 страницыMicrobiology Lecture 8 & 9 - Systemic & Opportunistic Mycoses (Raroromiki Trans)miguel cuevasОценок пока нет
- SynapseДокумент45 страницSynapsemiguel cuevasОценок пока нет
- Second Messengers-OLFU-MD 2017Документ66 страницSecond Messengers-OLFU-MD 2017Melissa SalayogОценок пока нет
- Lecture On Subcutaneous MycosesДокумент75 страницLecture On Subcutaneous Mycosesmiguel cuevasОценок пока нет
- Sachin Kumar CV Updated On 01-05-2014Документ5 страницSachin Kumar CV Updated On 01-05-2014Sachin Kumar PrajapatiОценок пока нет
- Spo Pengoplosan ObatДокумент9 страницSpo Pengoplosan Obatdj_ury21Оценок пока нет
- Topic 3Документ13 страницTopic 3JESSMINE SABELLANOОценок пока нет
- Test Bank For Lehnes Pharmacology For Nursing Care Burchum 9th EditionДокумент11 страницTest Bank For Lehnes Pharmacology For Nursing Care Burchum 9th EditionHenry Horowitz100% (29)
- PVCR AssessmentДокумент19 страницPVCR AssessmentNikitha SreeОценок пока нет
- Pharma 2nd LEДокумент3 страницыPharma 2nd LEkimberly abianОценок пока нет
- Pharma - Prescription Writing PDFДокумент3 страницыPharma - Prescription Writing PDFVon Javier Gamatero100% (1)
- Instant Clinical PharmacologyДокумент112 страницInstant Clinical Pharmacologycelecosib100% (3)
- Pricelist Sadana 28april2021Документ6 страницPricelist Sadana 28april2021Rama RakanataОценок пока нет
- Hard Gelatin CapsulesДокумент13 страницHard Gelatin CapsulesMohamed AlhamdaniОценок пока нет
- Pharmacy CPDProvider v2Документ9 страницPharmacy CPDProvider v2PRC BoardОценок пока нет
- Daftar Obat Bedah Dan AnestesiДокумент12 страницDaftar Obat Bedah Dan AnestesiGanien Unggul Ardiyanto SoewiryoОценок пока нет
- Sample CPJE: Finasteride 1 MG Tablets #30 1 Tab P.O. Daily For Benign Prostatic HyperplasiaДокумент12 страницSample CPJE: Finasteride 1 MG Tablets #30 1 Tab P.O. Daily For Benign Prostatic HyperplasiaHerne Balberde78% (9)
- New Drug Delivery Systems: A Global OpportunityДокумент24 страницыNew Drug Delivery Systems: A Global OpportunityRugun Clara SamosirОценок пока нет
- Cotizacion Farmacia 17.08.2022Документ48 страницCotizacion Farmacia 17.08.2022Alicia OrtizОценок пока нет
- (Tergecef) DR - Estoque: FluidsДокумент2 страницы(Tergecef) DR - Estoque: FluidsSean SialanaОценок пока нет
- 3.3 Medicine LabelДокумент6 страниц3.3 Medicine LabelStefmi Dhila WandaОценок пока нет
- Routes of Drug AdministrationДокумент36 страницRoutes of Drug Administrationapule geraldhumbleОценок пока нет
- Obat Yang Bekerja Pada SarafДокумент31 страницаObat Yang Bekerja Pada SarafzaroziОценок пока нет
- Laporan Obat HarianДокумент8 страницLaporan Obat HarianNi Dar100% (1)
- Compliance CircularДокумент1 страницаCompliance CircularsadafОценок пока нет
- FB U Manual Medication Order 1.5.1 1st Review 080217Документ55 страницFB U Manual Medication Order 1.5.1 1st Review 080217raj_pegasusОценок пока нет
- Tranexamic Acid Drug StudyДокумент3 страницыTranexamic Acid Drug Studyswitchlers anneОценок пока нет
- Remdesivir Distributor ListДокумент15 страницRemdesivir Distributor Listbasit.000Оценок пока нет
- BCS Losartan PDFДокумент8 страницBCS Losartan PDFHesti HariantiОценок пока нет
- Obat Non E-Cat (Maret-April) NewДокумент61 страницаObat Non E-Cat (Maret-April) NewfiannysjahjadiОценок пока нет
- Data All Item Per21112020Документ106 страницData All Item Per21112020Henry BudiawanОценок пока нет
- Gastro Recommendation DCGI SecДокумент3 страницыGastro Recommendation DCGI SecDipan KadiaОценок пока нет
- PharmabizДокумент1 страницаPharmabizbushraОценок пока нет
- Pharmacovigilance - Sem VIIIДокумент4 страницыPharmacovigilance - Sem VIIIkuttiappan anithaОценок пока нет