Вам также может понравиться
- Rules and Directions for the Employment of Injections in Various DiseasesОт EverandRules and Directions for the Employment of Injections in Various DiseasesОценок пока нет
- Ascites, A Simple Guide To The Condition, Treatment And Related ConditionsОт EverandAscites, A Simple Guide To The Condition, Treatment And Related ConditionsОценок пока нет
- Benign Prostatic Hyperplasia. NCM 109Документ16 страницBenign Prostatic Hyperplasia. NCM 109Niña Jean Tormis AldabaОценок пока нет
- NCP BPHДокумент8 страницNCP BPHjyaba0% (1)
- Volume 1Документ2 страницыVolume 1roxybiscanteОценок пока нет
- NCP BPHДокумент1 страницаNCP BPHyasiraОценок пока нет
- Urinary EliminationДокумент6 страницUrinary EliminationryamonamourofficialОценок пока нет
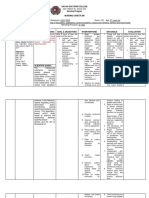
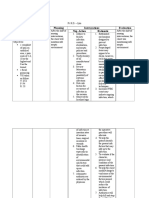
- Assessment Explanation Planning Interventions Rationale Evaluation Subjective: Short Term: Short TermДокумент5 страницAssessment Explanation Planning Interventions Rationale Evaluation Subjective: Short Term: Short TermGrape JuiceОценок пока нет
- NCP Urinary RetentionДокумент3 страницыNCP Urinary RetentionKingJayson Pacman06Оценок пока нет
- Dihydrotestosterone (DHT) - DHT Stimulates Cell Growth in The Tissue That Lines The Prostate GlandДокумент7 страницDihydrotestosterone (DHT) - DHT Stimulates Cell Growth in The Tissue That Lines The Prostate GlandPeter Kenneth LampitocОценок пока нет
- NCP Urine RetentionДокумент4 страницыNCP Urine RetentionKingJayson Pacman06Оценок пока нет
- Fluid Volume Excess NCPДокумент3 страницыFluid Volume Excess NCPAfia TawiahОценок пока нет
- NCP (BPH)Документ8 страницNCP (BPH)NataCo50% (2)
- NCP GRAND CASE PRE C Nursing ProblemsДокумент9 страницNCP GRAND CASE PRE C Nursing ProblemsAngie Mandeoya100% (1)
- Prado NCPДокумент4 страницыPrado NCPalleah pradoОценок пока нет
- Cholera N C P BY BHERU LALДокумент2 страницыCholera N C P BY BHERU LALBheru LalОценок пока нет
- Nursing Care Plan 1: Diagnosis Goal Nursing Interventions RationaleДокумент8 страницNursing Care Plan 1: Diagnosis Goal Nursing Interventions RationaleTrysna Ayu SukardiОценок пока нет
- Urinary Elimination: (Midterm)Документ14 страницUrinary Elimination: (Midterm)Mina RacadioОценок пока нет
- PERITONITISДокумент27 страницPERITONITISTiffany Adrias100% (1)
- Medical Surgical Nursing: Gracious Colleg of Nursing Abhanpur Raipur (C.G.)Документ9 страницMedical Surgical Nursing: Gracious Colleg of Nursing Abhanpur Raipur (C.G.)Topeshwar TpkОценок пока нет
- GI SYSTEM ANS 2nd DayДокумент6 страницGI SYSTEM ANS 2nd DayJohn AjishОценок пока нет
- Nursing Care PlanДокумент2 страницыNursing Care Planmjoie_baby6568470100% (6)
- Hepatitis A N C P BY BHERU LALДокумент2 страницыHepatitis A N C P BY BHERU LALBheru LalОценок пока нет
- Group-5 NCM-107 NCPДокумент4 страницыGroup-5 NCM-107 NCPbulok netflakes100% (1)
- Davao Doctors College Nursing Program Nursing Care PlanДокумент3 страницыDavao Doctors College Nursing Program Nursing Care PlanPRINCESS KOBAYASHIОценок пока нет
- Module 2 1Документ3 страницыModule 2 1Lacangan, Thea YvonneОценок пока нет
- Colle Ofn: Nursing Care PlanДокумент4 страницыColle Ofn: Nursing Care PlanDara Sophia EncarguezОценок пока нет
- Case Scenario: Prostate CancerДокумент5 страницCase Scenario: Prostate Cancer24 PAULINO ALDRIN MUJARОценок пока нет
- Nursing Care Plan: RationaleДокумент5 страницNursing Care Plan: Rationalerona-chanОценок пока нет
- Catheterization DemoДокумент3 страницыCatheterization DemoChris Daniel LeonorОценок пока нет
- NCP MeningitisДокумент2 страницыNCP MeningitisARISОценок пока нет
- Fluid Volume Deficit R/T Diarrhea & VomitingДокумент4 страницыFluid Volume Deficit R/T Diarrhea & Vomitingjisoo100% (3)
- Renal FunctionДокумент11 страницRenal FunctionJanely EstreraОценок пока нет
- Computation of Urine OutputДокумент4 страницыComputation of Urine OutputKassandra LabeОценок пока нет
- Impaired Urinary EliminationДокумент2 страницыImpaired Urinary EliminationRODERICK FELICIANO JR.Оценок пока нет
- NCP ProperДокумент9 страницNCP Properstephanie eduarteОценок пока нет
- Fluid Volume Excess (CRF)Документ4 страницыFluid Volume Excess (CRF)NursesLabs.com100% (1)
- ProstatectomyДокумент9 страницProstatectomymardsz100% (1)
- Cirrhosis of The LiverДокумент2 страницыCirrhosis of The LiverBheru LalОценок пока нет
- Acute GlomerulonephritisДокумент1 страницаAcute GlomerulonephritisAyrheen FornolesОценок пока нет
- Assignment in NCM 106 LectureДокумент6 страницAssignment in NCM 106 LectureJeanessa Delantar QuilisadioОценок пока нет
- NCPДокумент6 страницNCPJane CasiquinОценок пока нет
- Benign Prostatic HyperplasiaДокумент9 страницBenign Prostatic Hyperplasiamardsz100% (1)
- Assessment Diagnosis Planning Intervention-Rationale Evaluation Fluid Volume Excess Related ToДокумент3 страницыAssessment Diagnosis Planning Intervention-Rationale Evaluation Fluid Volume Excess Related ToJen BallesterosОценок пока нет
- Demo Bladder IrrigationДокумент4 страницыDemo Bladder IrrigationTopeshwar TpkОценок пока нет
- Justyne Rafaela A. Vidal BSN 3 Laryngeal Cancer Nursing Measure Procedure Reason For Doing The ProcedureДокумент2 страницыJustyne Rafaela A. Vidal BSN 3 Laryngeal Cancer Nursing Measure Procedure Reason For Doing The ProcedureAllyson AllysonОценок пока нет
- Impaired Urinary EliminationДокумент3 страницыImpaired Urinary EliminationDenise Republika100% (1)
- Assessment Nursing Diagnosis Planning (Desired or Expected Outcomes) Nursing Interventions Rationale EvaluationДокумент11 страницAssessment Nursing Diagnosis Planning (Desired or Expected Outcomes) Nursing Interventions Rationale EvaluationAsniah Hadjiadatu Abdullah100% (1)
- Name: A.V. Age: 12 Y/O Sex: M Diagnosis: Dengue Hemorrhagic Fever Assessment Diagnosis Planning Intervention EvaluationДокумент8 страницName: A.V. Age: 12 Y/O Sex: M Diagnosis: Dengue Hemorrhagic Fever Assessment Diagnosis Planning Intervention Evaluationglen glenОценок пока нет
- Bladder IrrigationДокумент3 страницыBladder IrrigationMyfanway Am-isОценок пока нет
- NCP - Impaired Urinary EliminationДокумент3 страницыNCP - Impaired Urinary EliminationFretzgine Lou ManuelОценок пока нет
- Bladder Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandBladder Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- Hematuria, (Blood in Urine) A Simple Guide to The Condition, Related Diseases And Use in Diagnosis of DiseasesОт EverandHematuria, (Blood in Urine) A Simple Guide to The Condition, Related Diseases And Use in Diagnosis of DiseasesРейтинг: 5 из 5 звезд5/5 (2)
- Ulcerative Colitis, A Simple Guide To The Condition, Treatment And Related ConditionsОт EverandUlcerative Colitis, A Simple Guide To The Condition, Treatment And Related ConditionsОценок пока нет
- Diverticulosis, A Simple Guide to the Condition, Treatment and Related DiseasesОт EverandDiverticulosis, A Simple Guide to the Condition, Treatment and Related DiseasesРейтинг: 1 из 5 звезд1/5 (1)
- Urinary Retention, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandUrinary Retention, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsРейтинг: 1 из 5 звезд1/5 (1)
- Dictionary of Veterinary Terms: Vet-Speak Deciphered for the Non VeterinarianОт EverandDictionary of Veterinary Terms: Vet-Speak Deciphered for the Non VeterinarianОценок пока нет
- I Practiced The Following During Childbirth. 4 3 2 1 F WV WM QDДокумент2 страницыI Practiced The Following During Childbirth. 4 3 2 1 F WV WM QDRhea Mae Valles - ReyesОценок пока нет
- SWOR AnalysisДокумент3 страницыSWOR AnalysisRhea Mae Valles - ReyesОценок пока нет
- Anaphy Patho BPHДокумент5 страницAnaphy Patho BPHRhea Mae Valles - ReyesОценок пока нет
- Assessment Diagnosis Planning Interventions Evaluation Nsg. Action RationaleДокумент2 страницыAssessment Diagnosis Planning Interventions Evaluation Nsg. Action RationaleRhea Mae Valles - ReyesОценок пока нет
- Semi CS BCДокумент17 страницSemi CS BCRhea Mae Valles - ReyesОценок пока нет
- Ds Pedia WardДокумент2 страницыDs Pedia WardRhea Mae Valles - ReyesОценок пока нет
- Ms. Valles Wound Care Center: Submitted By: Rhea Mae V. Valles Bsn-Iii Submitted To: Mr. Ismael LagrasonДокумент2 страницыMs. Valles Wound Care Center: Submitted By: Rhea Mae V. Valles Bsn-Iii Submitted To: Mr. Ismael LagrasonRhea Mae Valles - ReyesОценок пока нет
- Assessment Diagnosis Planning Interventions Evaluation Nsg. Action RationaleДокумент2 страницыAssessment Diagnosis Planning Interventions Evaluation Nsg. Action RationaleRhea Mae Valles - ReyesОценок пока нет
- Case Analysis For Acute GastroenteritisДокумент3 страницыCase Analysis For Acute GastroenteritisRhea Mae Valles - ReyesОценок пока нет
- Assessment Diagnosis Planning Interventions Evaluation Nsg. Action RationaleДокумент2 страницыAssessment Diagnosis Planning Interventions Evaluation Nsg. Action RationaleRhea Mae Valles - ReyesОценок пока нет
- LepДокумент6 страницLepRhea Mae Valles - ReyesОценок пока нет
- Report Cd1Документ6 страницReport Cd1Rhea Mae Valles - ReyesОценок пока нет
- Rheumatoid 1Документ18 страницRheumatoid 1Rhea Mae Valles - ReyesОценок пока нет
- Most Participative Most BehaveДокумент4 страницыMost Participative Most BehaveRhea Mae Valles - ReyesОценок пока нет
- NCP Pt. DE ASISДокумент3 страницыNCP Pt. DE ASISRhea Mae Valles - ReyesОценок пока нет
- Drug Study: Rhea Mae V. Valles Bsn-IiiДокумент1 страницаDrug Study: Rhea Mae V. Valles Bsn-IiiRhea Mae Valles - ReyesОценок пока нет
- Ds Pedia WardДокумент2 страницыDs Pedia WardRhea Mae Valles - ReyesОценок пока нет
- Occupational TherapyДокумент2 страницыOccupational TherapyRhea Mae Valles - ReyesОценок пока нет
- OAДокумент4 страницыOARhea Mae Valles - ReyesОценок пока нет
- NCP Pt. DE ASISДокумент3 страницыNCP Pt. DE ASISRhea Mae Valles - ReyesОценок пока нет
- Activity IntoleranceДокумент3 страницыActivity IntoleranceRhea Mae Valles - ReyesОценок пока нет
- Assessment Diagnosis Planning Intervention Evaluation Nsg. Action RationaleДокумент3 страницыAssessment Diagnosis Planning Intervention Evaluation Nsg. Action RationaleRhea Mae Valles - ReyesОценок пока нет
- Ineffective Airway ClearanceДокумент2 страницыIneffective Airway ClearanceRhea Mae Valles - ReyesОценок пока нет
- Assessment Diagnosis Planning Interventions Evaluation Nsg. Action RationaleДокумент3 страницыAssessment Diagnosis Planning Interventions Evaluation Nsg. Action RationaleRhea Mae Valles - ReyesОценок пока нет
- NCP Pt. DE ASISДокумент3 страницыNCP Pt. DE ASISRhea Mae Valles - ReyesОценок пока нет
- Drug Study: Rhea Mae V. Valles Bsn-IiiДокумент1 страницаDrug Study: Rhea Mae V. Valles Bsn-IiiRhea Mae Valles - ReyesОценок пока нет
- NCP Pt. DE ASISДокумент3 страницыNCP Pt. DE ASISRhea Mae Valles - ReyesОценок пока нет
- NCP Pt. GomezДокумент2 страницыNCP Pt. GomezRhea Mae Valles - ReyesОценок пока нет
- NCP Pt. DE ASISДокумент3 страницыNCP Pt. DE ASISRhea Mae Valles - ReyesОценок пока нет
- Nutritional Epidemiology: Reference: Nutrition Epidemiology by Walter WilletДокумент24 страницыNutritional Epidemiology: Reference: Nutrition Epidemiology by Walter WilletMarelign TilahunОценок пока нет
- DSL: Diabetes Mellitus: Endocrine & Metabolism ModuleДокумент45 страницDSL: Diabetes Mellitus: Endocrine & Metabolism ModuleTower AlangОценок пока нет
- CHN Epidemiology QUIZДокумент1 страницаCHN Epidemiology QUIZJammeОценок пока нет
- PONR - Comprehensive Nursing Health History and Physical ExaminationДокумент21 страницаPONR - Comprehensive Nursing Health History and Physical ExaminationDRJC100% (1)
- Sample Final Exam Questions-f14-KEYДокумент6 страницSample Final Exam Questions-f14-KEYAlias HedgeОценок пока нет
- Figo Staging Cancer CervicalДокумент7 страницFigo Staging Cancer CervicalihsansabridrОценок пока нет
- Patho AsthmaДокумент1 страницаPatho AsthmaAyel JimenezОценок пока нет
- Pathogenesis of Bacterial InfectionДокумент35 страницPathogenesis of Bacterial InfectionDiyantoro NyoОценок пока нет
- ShockДокумент124 страницыShockRahman Mukti AjiОценок пока нет
- Definitive Guide To Red Light Therapy PhotobiomodulationДокумент10 страницDefinitive Guide To Red Light Therapy PhotobiomodulationDavid Jenkins0% (2)
- Prevenção Secundária Avc Isquêmico - Guideline 2022Документ41 страницаPrevenção Secundária Avc Isquêmico - Guideline 2022Felipe Stoquetti de AbreuОценок пока нет
- Histological Features of Candidiasis: By:Mamdouh Dagsh Alshrifi ID:321103259Документ14 страницHistological Features of Candidiasis: By:Mamdouh Dagsh Alshrifi ID:321103259Mamdouh D AlrwailiОценок пока нет
- Nursing Care Plan: University of Tabuk Faculty of Applied Medical Science Department of NursingДокумент3 страницыNursing Care Plan: University of Tabuk Faculty of Applied Medical Science Department of NursingZedoo AlmaroaaneОценок пока нет
- Case 4-2021: A 70-Year-Old Woman With Dyspnea On Exertion and Abnormal Findings On Chest ImagingДокумент12 страницCase 4-2021: A 70-Year-Old Woman With Dyspnea On Exertion and Abnormal Findings On Chest ImagingBruno ConteОценок пока нет
- Dilated CardiomyopathyДокумент23 страницыDilated CardiomyopathyYanna Habib-MangotaraОценок пока нет
- Pterygium & DacryocystitisДокумент45 страницPterygium & DacryocystitisAngelaTrinidadОценок пока нет
- Presented by DR Muhammad Usman Senior Lecturer BUCPT: Introduction To Screening For Referral in Physical TherapyДокумент27 страницPresented by DR Muhammad Usman Senior Lecturer BUCPT: Introduction To Screening For Referral in Physical Therapysaba ramzanОценок пока нет
- Case Study On Nephrotic SyndromeДокумент7 страницCase Study On Nephrotic SyndromeArchana VermaОценок пока нет
- ECG Crib SheetДокумент2 страницыECG Crib Sheetkp180surfingОценок пока нет
- Anatomic Therapy PDFДокумент364 страницыAnatomic Therapy PDFrahul_choubey_9Оценок пока нет
- Syphilis Symptoms, Causes, and DiagnosisДокумент3 страницыSyphilis Symptoms, Causes, and DiagnosisIndra FahleviОценок пока нет
- Combined Orthokeratology With Atropine For Children With Myopia: A Meta-AnalysisДокумент9 страницCombined Orthokeratology With Atropine For Children With Myopia: A Meta-AnalysiskarakuraОценок пока нет
- Chapter 27 - Common Reproductive ConditionsДокумент6 страницChapter 27 - Common Reproductive ConditionsEunice CortésОценок пока нет
- Immunology and Immunochemistry PDFДокумент8 страницImmunology and Immunochemistry PDFboatcomОценок пока нет
- Thyroid Hormone Profile in Chronic Kidney DiseaseДокумент6 страницThyroid Hormone Profile in Chronic Kidney DiseaserefaОценок пока нет
- The Truth About Polio VaccineДокумент23 страницыThe Truth About Polio Vaccinemagnumquest67% (3)
- Vigabatrin For IsДокумент12 страницVigabatrin For IsAndrew SantosoОценок пока нет
- SPC For Health Care Providers - Ivermax - Kaplet 12 MG - Ivermektin - DKL2107926604A1 - 2021 - 0 - 0Документ4 страницыSPC For Health Care Providers - Ivermax - Kaplet 12 MG - Ivermektin - DKL2107926604A1 - 2021 - 0 - 0Timothy OlsonОценок пока нет
- Pathological Repertory of The NosodesДокумент20 страницPathological Repertory of The Nosodespawajee100% (1)
- Systematic Review Pelaksanaan Programmatic Management of Drug-Resistant Tuberculosis Pada Pasien Tuberkulosis Resistan ObatДокумент8 страницSystematic Review Pelaksanaan Programmatic Management of Drug-Resistant Tuberculosis Pada Pasien Tuberkulosis Resistan ObatAdinda Pramesthi RiadyaniОценок пока нет