Вам также может понравиться
- 3 - Important Topics For The AMC Part 1 MCQ CAT ExaminationДокумент23 страницы3 - Important Topics For The AMC Part 1 MCQ CAT ExaminationMohd FaizhakimОценок пока нет
- CardiologyДокумент4 страницыCardiologyES AbedОценок пока нет
- Review QuizДокумент107 страницReview QuizAhmad JalladОценок пока нет
- AMC Part 1 CAT MCQ Examination Important TopicsДокумент23 страницыAMC Part 1 CAT MCQ Examination Important TopicsSOMANATHAN UMAHSUTHANОценок пока нет
- Cardiology PDFДокумент27 страницCardiology PDFNada AKОценок пока нет
- 6 - Pericarditis & MyocarditisДокумент6 страниц6 - Pericarditis & MyocarditisAhmed AdelОценок пока нет
- SHOCKДокумент5 страницSHOCKSamridhi SrivastavaОценок пока нет
- Definition of Stroke: Risk FactorsДокумент12 страницDefinition of Stroke: Risk FactorsNik Fatnin YusoffОценок пока нет
- TCM3 Long Quiz 1-1Документ3 страницыTCM3 Long Quiz 1-1PARA SYTEОценок пока нет
- Express GI Notes 2012Документ31 страницаExpress GI Notes 2012Zul Azim AnuarОценок пока нет
- Pulmonary Valve Stenosis & RegurgitationДокумент5 страницPulmonary Valve Stenosis & Regurgitationwika.s1243Оценок пока нет
- MCQ Int - MedДокумент166 страницMCQ Int - MedOmar Ahmed100% (1)
- Recovery and ComplicationsДокумент36 страницRecovery and ComplicationsWalid KahinОценок пока нет
- MCQ IM DepДокумент183 страницыMCQ IM DepHesham A100% (3)
- Shock: DefinitionДокумент18 страницShock: DefinitionGaurav ChauhanОценок пока нет
- Theoretical Revision in 25 Days 2019Документ131 страницаTheoretical Revision in 25 Days 2019Sleman M BashirОценок пока нет
- Surgery II: Congenital Heart DiseaseДокумент10 страницSurgery II: Congenital Heart DiseaseRea Dominique CabanillaОценок пока нет
- 20-Feb-2023 at 2 - 11 - 12 PMДокумент37 страниц20-Feb-2023 at 2 - 11 - 12 PMmihikaОценок пока нет
- Management of Patientswith Complications From Heart DiseaseДокумент8 страницManagement of Patientswith Complications From Heart Diseasekristine keen buanОценок пока нет
- Shock, Acid-Base Balance and Fluid Therapy: Shock Stages of ShockДокумент4 страницыShock, Acid-Base Balance and Fluid Therapy: Shock Stages of ShockLonely WolfОценок пока нет
- TH Year Past Q InternalДокумент220 страницTH Year Past Q Internalibrahim 12Оценок пока нет
- Blood & HaematologyДокумент12 страницBlood & HaematologySagor DeyОценок пока нет
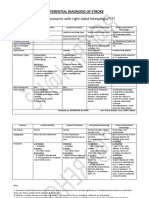
- Differential Diagnosis of StrokeДокумент2 страницыDifferential Diagnosis of StrokeAnonymous 7dsX2F8nОценок пока нет
- Echo Heart FailureДокумент82 страницыEcho Heart FailureJing CruzОценок пока нет
- General ExaminationДокумент2 страницыGeneral ExaminationYara WaelОценок пока нет
- Mphil Mid Term 1 With KeyДокумент3 страницыMphil Mid Term 1 With Keyasfandyar roghaniОценок пока нет
- Cardiovascular Pathology - 025) Valvular Heart Diseases Overview (Notes)Документ18 страницCardiovascular Pathology - 025) Valvular Heart Diseases Overview (Notes)Geraldine HernandezОценок пока нет
- CMSE 2019 Paper 1Документ26 страницCMSE 2019 Paper 1Sandip GaraiОценок пока нет
- Cardiology Revision DR - Ahmed MowafyДокумент35 страницCardiology Revision DR - Ahmed MowafyMohamed AlsaabОценок пока нет
- Cardiovascular NotesДокумент69 страницCardiovascular NotesAnnissaLarnardОценок пока нет
- NOTES - Heart FailureДокумент5 страницNOTES - Heart Failureeva halimОценок пока нет
- Aortic Valve RegurgitationДокумент3 страницыAortic Valve Regurgitationprakash ramОценок пока нет
- Cvspa07 Cardiac FailureДокумент6 страницCvspa07 Cardiac FailureRobert So JrОценок пока нет
- Heart FailureДокумент4 страницыHeart FailurersheedmahdiiОценок пока нет
- MCQ 1. Heart Sound Heart Sound S1 S2Документ7 страницMCQ 1. Heart Sound Heart Sound S1 S2Atirah AaОценок пока нет
- 200 Special Topics For 42 BCSДокумент187 страниц200 Special Topics For 42 BCSRezaul RazibОценок пока нет
- 2 Year 2 Term: PathophysiologyДокумент21 страница2 Year 2 Term: PathophysiologyMasyithah ZerlinaОценок пока нет
- Hings To Do: Tuesday, 28 October 2014 2:44 AmДокумент45 страницHings To Do: Tuesday, 28 October 2014 2:44 AmMital BhaktaОценок пока нет
- Chronic Liver DiseaseДокумент3 страницыChronic Liver DiseaseNikey LimОценок пока нет
- TH ND TH NDДокумент3 страницыTH ND TH NDSoumabho ParuiОценок пока нет
- 140 - Neurology Pathology) Seizures - Etiology, Pathophysiology, Clinical Features, Treatment, ComplicationsДокумент10 страниц140 - Neurology Pathology) Seizures - Etiology, Pathophysiology, Clinical Features, Treatment, ComplicationsUssama MDОценок пока нет
- Heart FailureДокумент1 страницаHeart FailureDarell M. BookОценок пока нет
- Triad of DeathДокумент4 страницыTriad of DeathHayudhiaОценок пока нет
- FCPS SurgeryДокумент106 страницFCPS Surgeryrehan hayderОценок пока нет
- Cvs Assesment 1 OrigkeyДокумент5 страницCvs Assesment 1 OrigkeydrashtisataОценок пока нет
- Atrial Fibrillation AtfДокумент11 страницAtrial Fibrillation AtfChristine MagnoОценок пока нет
- Aortic StenosisДокумент16 страницAortic StenosisAbdur RaqibОценок пока нет
- Hemodynamic DisorderДокумент7 страницHemodynamic DisorderYana MilyushinaОценок пока нет
- 150 Must Read Topics To Pass AMC MCQ CATДокумент4 страницы150 Must Read Topics To Pass AMC MCQ CATNomar Casiven NonatoОценок пока нет
- Cardiology DR - Ahmed MowafyДокумент150 страницCardiology DR - Ahmed MowafyMohamed AlsaabОценок пока нет
- 345 - Hematology Physiology) PolycythemiasДокумент3 страницы345 - Hematology Physiology) PolycythemiasAro DanaОценок пока нет
- Hemodynamic DisordersДокумент6 страницHemodynamic DisordersPradeep100% (1)
- Afmg Medicine Test+ 2023 1Документ6 страницAfmg Medicine Test+ 2023 1manishОценок пока нет
- MS Faculty Mock Test 1 Question PaperДокумент16 страницMS Faculty Mock Test 1 Question Paperbikalbelar123Оценок пока нет
- Pathophysiology CVA (Final2)Документ10 страницPathophysiology CVA (Final2)Jayselle Costes FelipeОценок пока нет
- Nigel Fong's MRCP NotesДокумент66 страницNigel Fong's MRCP Noteslucas0% (1)
- 10 CardiomyopathyДокумент71 страница10 CardiomyopathyAnonymous vUEDx8100% (5)
- THROMBOSISДокумент11 страницTHROMBOSISChandan DebbarmaОценок пока нет
- Dentistry: A Case of Drug - Induced Xerostomia and A Literature Review of The Management OptionsДокумент4 страницыDentistry: A Case of Drug - Induced Xerostomia and A Literature Review of The Management OptionsSasa AprilaОценок пока нет
- Serosal Appendicitis: Incidence, Causes and Clinical SignificanceДокумент3 страницыSerosal Appendicitis: Incidence, Causes and Clinical SignificancenaufalrosarОценок пока нет
- Letter Explanation To DoctorДокумент1 страницаLetter Explanation To DoctorDonnaОценок пока нет
- Exploratory Study of Self-Medication Practices Among StudentsДокумент5 страницExploratory Study of Self-Medication Practices Among StudentsN SОценок пока нет
- Carboplatin MonographДокумент9 страницCarboplatin Monographmerkuri100% (1)
- Test Bank For Medical Surgical Nursing 7th Edition Donna D IgnataviciusДокумент24 страницыTest Bank For Medical Surgical Nursing 7th Edition Donna D Ignataviciusrobertblackmwjkpnyfrq100% (37)
- Uterine Leiomyomas (Fibroids) - Epidemiology, Clinical Features, Diagnosis, and Natural History - UpToDateДокумент48 страницUterine Leiomyomas (Fibroids) - Epidemiology, Clinical Features, Diagnosis, and Natural History - UpToDateRuben Orduño RizoОценок пока нет
- Anti InflamasiДокумент27 страницAnti InflamasiAuLia DamayantiОценок пока нет
- Case Report Two Blue Chromhidrosis Patients in Emergency RoomДокумент2 страницыCase Report Two Blue Chromhidrosis Patients in Emergency RoomInternational Journal of Innovative Science and Research TechnologyОценок пока нет
- Children Complete QSTДокумент1 страницаChildren Complete QSTHoda AtwaОценок пока нет
- 4D CT With Respiratory GatingДокумент2 страницы4D CT With Respiratory GatingLaura Karina Sanchez ColinОценок пока нет
- OncologyДокумент3 страницыOncologyMichtropolisОценок пока нет
- Ebook Emergency Radiology The Requisites PDF Full Chapter PDFДокумент67 страницEbook Emergency Radiology The Requisites PDF Full Chapter PDFrobert.prinz849100% (22)
- TEACHING PLAN HypertensionДокумент2 страницыTEACHING PLAN Hypertensionpheochromocytoma59% (41)
- Approach To The Adult With Epistaxis - UpToDateДокумент29 страницApproach To The Adult With Epistaxis - UpToDateAntonella Angulo CruzadoОценок пока нет
- Departm Ent of Education: R e P U B Lic of Tlje JH JilippineffДокумент7 страницDepartm Ent of Education: R e P U B Lic of Tlje JH JilippineffJoyce CarilloОценок пока нет
- Hypertency Emergency Acute PDFДокумент12 страницHypertency Emergency Acute PDFmasdika09Оценок пока нет
- Rishum 1 262421216 2Документ1 страницаRishum 1 262421216 2HellcroZОценок пока нет
- Final Report Sero Survey0409Документ160 страницFinal Report Sero Survey0409BSL-2Оценок пока нет
- Grading Scale 2017 PDFДокумент2 страницыGrading Scale 2017 PDFAlibek ZhumanazarovОценок пока нет
- ATO - Compassionate - Release - of - SuperannuationДокумент5 страницATO - Compassionate - Release - of - SuperannuationBen RamalliОценок пока нет
- Seminar On Shock: IndexДокумент37 страницSeminar On Shock: IndexGayathri R100% (1)
- Common Dermatology Multiple Choice Questions and Answers - 6Документ3 страницыCommon Dermatology Multiple Choice Questions and Answers - 6Atul Kumar Mishra100% (1)
- Revisiting Structural Family TherapyДокумент2 страницыRevisiting Structural Family TherapyKim ScottОценок пока нет
- Clark 2004Документ18 страницClark 2004Joo XanderОценок пока нет
- GBS Source 1Документ4 страницыGBS Source 1PJHG50% (2)
- 30613167: Management of Osteitis Pubis in Athletes Rehabilitation and Return To Training - A Review of The Most Recent Literature PDFДокумент10 страниц30613167: Management of Osteitis Pubis in Athletes Rehabilitation and Return To Training - A Review of The Most Recent Literature PDFRicovially DavyaОценок пока нет
- M SДокумент162 страницыM SAnn Claudette SyОценок пока нет
- Subacute Bacterial Endocarditis and Antimicrobial ProphylaxisДокумент42 страницыSubacute Bacterial Endocarditis and Antimicrobial Prophylaxisalex-pham-2258Оценок пока нет
- Geriatric Medicine and Gerontology: Prevention of Frailty in The Elderly Through Physical Activity and NutritionДокумент8 страницGeriatric Medicine and Gerontology: Prevention of Frailty in The Elderly Through Physical Activity and NutritionSARAH AZIZAH 2015Оценок пока нет