Вам также может понравиться
- Holistic Solutions For Anxiety & Depression in Therapy - Peter BongiornoДокумент290 страницHolistic Solutions For Anxiety & Depression in Therapy - Peter Bongiornojohnlived100% (2)
- Selected Instructional Course LecturesДокумент27 страницSelected Instructional Course LecturesAhmad ShakirОценок пока нет
- Length Tension Testing Book 1, Lower Quadrant: A Workbook of Manual Therapy TechniquesОт EverandLength Tension Testing Book 1, Lower Quadrant: A Workbook of Manual Therapy TechniquesРейтинг: 3.5 из 5 звезд3.5/5 (3)
- CNA Practice TestДокумент12 страницCNA Practice TestJoe Prempeh50% (4)
- Ii. NCP: Black, Et - Al. (2005) .Me Dical Surgical Nursing. 7 Edition - Elsevie R Pte LTD.P 927Документ4 страницыIi. NCP: Black, Et - Al. (2005) .Me Dical Surgical Nursing. 7 Edition - Elsevie R Pte LTD.P 927Lecery Sophia Wong75% (4)
- Length Tension Testing Book 2, Upper Quadrant: A Workbook of Manual Therapy TechniquesОт EverandLength Tension Testing Book 2, Upper Quadrant: A Workbook of Manual Therapy TechniquesРейтинг: 1 из 5 звезд1/5 (1)
- Interpretation of MriДокумент12 страницInterpretation of Mrijimitkapadia100% (1)
- 9 PropofolДокумент2 страницы9 PropofolAbdelhafiz Susmiran100% (3)
- Neuromuscular Blocking DrugsДокумент3 страницыNeuromuscular Blocking DrugsYogi drОценок пока нет
- 544 Prophetic MedicineДокумент6 страниц544 Prophetic MedicineMohd HasanОценок пока нет
- BCS RadiologiДокумент46 страницBCS RadiologiHananya Manroe100% (1)
- Acute Glomerulonephritis (AGN) : Paediatric Department CMEДокумент25 страницAcute Glomerulonephritis (AGN) : Paediatric Department CMENurul Syazwani Ramli67% (3)
- Neuro RehabilitationДокумент58 страницNeuro Rehabilitationsyafaat164Оценок пока нет
- Nomina Anatomica VeterinariaДокумент177 страницNomina Anatomica VeterinariaAnđelka PopovićОценок пока нет
- OB Drug Study - MethylergonovineДокумент2 страницыOB Drug Study - MethylergonovineJustin Ancog0% (1)
- NCP OrthoДокумент5 страницNCP OrthoMyluck Elaine Wailan100% (4)
- Nursing Care Plan - NumbnessДокумент2 страницыNursing Care Plan - NumbnessJasmin Jacob100% (3)
- Drug Study: Adult: Induction: 40 MGДокумент2 страницыDrug Study: Adult: Induction: 40 MGpretty_mary100% (4)
- Regaining Bladder Control: For Incontinence on Exertion or Following Pelvic SurgeryОт EverandRegaining Bladder Control: For Incontinence on Exertion or Following Pelvic SurgeryОценок пока нет
- NCM 106 IntroductionДокумент126 страницNCM 106 IntroductionYra JhaneОценок пока нет
- Nursing Care Plan-Herniated Nucleus PulposusДокумент3 страницыNursing Care Plan-Herniated Nucleus PulposusJasmin Jacob67% (3)
- Patterson - Allergic Diseases 6th EdДокумент370 страницPatterson - Allergic Diseases 6th Edvasile100% (2)
- Nursing Care Plan: Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective Data: IndependentДокумент3 страницыNursing Care Plan: Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective Data: IndependentP BОценок пока нет
- HALOPERIDOLДокумент3 страницыHALOPERIDOLculla annaОценок пока нет
- Case StudyДокумент5 страницCase StudyJanina Jean ViñegasОценок пока нет
- Acute ConfusionДокумент7 страницAcute ConfusionYasin JazОценок пока нет
- NCP Mugar Icu3 Batch2 GRP3Документ2 страницыNCP Mugar Icu3 Batch2 GRP3FRANZI ALYANNA MUGARОценок пока нет
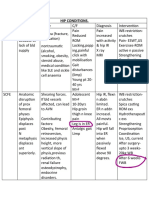
- Hip ConditionsДокумент2 страницыHip ConditionsseemaОценок пока нет
- Lower Limb Trauma in A Young Man CASE STUDY1Документ8 страницLower Limb Trauma in A Young Man CASE STUDY1Renee RoSeОценок пока нет
- Drug Study Irene 9 11Документ10 страницDrug Study Irene 9 11Irene Grace BalcuevaОценок пока нет
- Drug Study 3Документ6 страницDrug Study 3Daniela DianaОценок пока нет
- 3rd Year Neuro Treatment LectureДокумент31 страница3rd Year Neuro Treatment LectureSelinah Sslengs SeepeОценок пока нет
- نسخة vaginal delieveryДокумент4 страницыنسخة vaginal delieveryرهف الرفاعيОценок пока нет
- NCP Mugar Leptospirosis TLJPHДокумент2 страницыNCP Mugar Leptospirosis TLJPHFRANZI ALYANNA MUGARОценок пока нет
- General Guidelines /precautions:: Non-Operative Labral/FAI Hip Rehabilitation GuidelineДокумент4 страницыGeneral Guidelines /precautions:: Non-Operative Labral/FAI Hip Rehabilitation GuidelineBurr NerrОценок пока нет
- NCP CVA ImmoblityДокумент3 страницыNCP CVA ImmoblityAnalyn FloresОценок пока нет
- Drug StudyДокумент6 страницDrug StudyLarr SumalpongОценок пока нет
- NCP ImmobilityДокумент1 страницаNCP ImmobilityBcoi QuilacioОценок пока нет
- DS Male SurgicalДокумент6 страницDS Male SurgicalErryl Justine AdvinculaОценок пока нет
- Breathing Problems Drowsiness, Dizziness Constipation, Nausea Vomiting Sweating Numbness, Tingling, or Cold Feeling in Your Hands and FeetДокумент8 страницBreathing Problems Drowsiness, Dizziness Constipation, Nausea Vomiting Sweating Numbness, Tingling, or Cold Feeling in Your Hands and FeetGino B. BulanaОценок пока нет
- Pasion, James Nicole R. BSN - 2 NCM 101 Lec Assignment: 1 ML, 0.2 MGДокумент4 страницыPasion, James Nicole R. BSN - 2 NCM 101 Lec Assignment: 1 ML, 0.2 MGۦۦ JamesОценок пока нет
- Paracetamol Tramadol KCLДокумент5 страницParacetamol Tramadol KCLDani DaniОценок пока нет
- OrthopeadicsДокумент30 страницOrthopeadicsharshaОценок пока нет
- Status POMR LBPДокумент4 страницыStatus POMR LBPGiovanno HermawanОценок пока нет
- Chapter 36Документ3 страницыChapter 36Samantha QuintoОценок пока нет
- Cauda Equina Syndrom in Hernia Nukleus Pulposus: Dr. Riski AmandaДокумент46 страницCauda Equina Syndrom in Hernia Nukleus Pulposus: Dr. Riski AmandaMagista NugrahaОценок пока нет
- SPINEДокумент8 страницSPINEadrian kristopher dela cruzОценок пока нет
- NOTESДокумент1 страницаNOTESTrixter GarciaОценок пока нет
- Cardio Case Study 11Документ5 страницCardio Case Study 11api-646131765Оценок пока нет
- Bab IiiДокумент14 страницBab IiiLisa Anggrayni RamliОценок пока нет
- NursingCribcom Nursing Care Plan KyphosisДокумент2 страницыNursingCribcom Nursing Care Plan KyphosisKrissa Pearl CalleraОценок пока нет
- Week 2 NURS 2016 Cheat Sheet: by ViaДокумент1 страницаWeek 2 NURS 2016 Cheat Sheet: by ViaReihann N. EdresОценок пока нет
- L&D DrugsДокумент3 страницыL&D DrugsJessica 'Baker' IsaacsОценок пока нет
- Short Term:: As Acetaminophen (Tylenol), Ibuprofen (Advil, Motrin), or Naproxen (Aleve)Документ2 страницыShort Term:: As Acetaminophen (Tylenol), Ibuprofen (Advil, Motrin), or Naproxen (Aleve)Aleeyah Krizle EstabilloОценок пока нет
- Assessment Nursing Diagnosis Nursing Outcome Intervention Implementation EvaluationДокумент14 страницAssessment Nursing Diagnosis Nursing Outcome Intervention Implementation EvaluationNur Fatima SanaaniОценок пока нет
- Surgical - Floor RequirementДокумент8 страницSurgical - Floor RequirementPureza Maye SalapangОценок пока нет
- Mindanao State University - Iligan Institute of Technology Student: EGAO, Vanessa Jones C. - Section:260Документ1 страницаMindanao State University - Iligan Institute of Technology Student: EGAO, Vanessa Jones C. - Section:260Vanessa EgaoОценок пока нет
- Drug Therapeutic RecordДокумент10 страницDrug Therapeutic RecordstrawberryОценок пока нет
- Health AssessmentДокумент13 страницHealth AssessmentImee TolentinoОценок пока нет
- Impaired Physical Mobility R/T Neuromuscular ImpairmentДокумент3 страницыImpaired Physical Mobility R/T Neuromuscular ImpairmentjisooОценок пока нет
- Drug Study Case AnalysisДокумент7 страницDrug Study Case AnalysisNine SaguiboОценок пока нет
- TBR Doktung LaveniaДокумент11 страницTBR Doktung LaveniaRiaОценок пока нет
- Drug StudyДокумент2 страницыDrug StudyEden Astred ObilloОценок пока нет
- Geria NCP, Dela CruzДокумент7 страницGeria NCP, Dela CruzStephany Dela CruzОценок пока нет
- Chp-2 An Introduction To Movement by Dr. WajidaДокумент12 страницChp-2 An Introduction To Movement by Dr. WajidaHusain MirzaОценок пока нет
- MethergineДокумент3 страницыMethergineLoue Jean GulfanОценок пока нет
- Nursing Care Plan: Non-Pharmacological InterventionsДокумент4 страницыNursing Care Plan: Non-Pharmacological InterventionsVivian PhamОценок пока нет
- Drug Study NifedipineДокумент3 страницыDrug Study NifedipineJanzelvine Lee MontenegroОценок пока нет
- Nursing Diagnosis Objectiv eДокумент4 страницыNursing Diagnosis Objectiv eرهف الرفاعيОценок пока нет
- Brain Breakthrough: The Art of Neurological Rehabilitation: Easy and Innovative Techniques, #1От EverandBrain Breakthrough: The Art of Neurological Rehabilitation: Easy and Innovative Techniques, #1Оценок пока нет
- Wse Week 4Документ2 страницыWse Week 4api-302138606Оценок пока нет
- Careplan Week2Документ2 страницыCareplan Week2api-302138606Оценок пока нет
- Wse Week 1 2Документ1 страницаWse Week 1 2api-302138606Оценок пока нет
- Makaha ClubhouseДокумент1 страницаMakaha Clubhouseapi-302138606Оценок пока нет
- Sbar CommunicationДокумент4 страницыSbar Communicationapi-302138606Оценок пока нет
- QUESTION: Does A Minor Have The Right To Request Contraception From A Doctor Without Parental Consent?Документ5 страницQUESTION: Does A Minor Have The Right To Request Contraception From A Doctor Without Parental Consent?api-302138606Оценок пока нет
- Health Policy Memo MgenoviaДокумент5 страницHealth Policy Memo Mgenoviaapi-302138606Оценок пока нет
- Wse Week 6 EportfolioДокумент2 страницыWse Week 6 Eportfolioapi-302138606Оценок пока нет
- Wse Week 1 MgenoviaДокумент2 страницыWse Week 1 Mgenoviaapi-302138606Оценок пока нет
- Uk Cultural PaperДокумент6 страницUk Cultural Paperapi-302138606Оценок пока нет
- Emotion Color WheelДокумент1 страницаEmotion Color Wheelapi-302138606Оценок пока нет
- MgenoviaresumeДокумент1 страницаMgenoviaresumeapi-302138606Оценок пока нет
- Mobility ReflectionДокумент1 страницаMobility Reflectionapi-302138606Оценок пока нет
- Diabetes HDL ArticleДокумент3 страницыDiabetes HDL Articleapi-302138606Оценок пока нет
- Cover LetterДокумент1 страницаCover Letterapi-302138606Оценок пока нет
- Ethics Paper Final DraftДокумент5 страницEthics Paper Final Draftapi-302138606Оценок пока нет
- A Report On Depression: Mental HealthДокумент12 страницA Report On Depression: Mental HealthArchiev KumarОценок пока нет
- Prob PDFДокумент12 страницProb PDFwallace120Оценок пока нет
- Peran Perawat Dalam Penanggulangan Bencana: Vol 6, No 1 Mei, Pp. 63-70 P-ISSN 2549-4880, E-ISSN 2614-1310 WebsiteДокумент8 страницPeran Perawat Dalam Penanggulangan Bencana: Vol 6, No 1 Mei, Pp. 63-70 P-ISSN 2549-4880, E-ISSN 2614-1310 WebsiteEbato SanaeОценок пока нет
- Drug To Drug InteractionДокумент47 страницDrug To Drug InteractionMannan SokaОценок пока нет
- Corrected Ortho QsДокумент48 страницCorrected Ortho QsMuhamad Danial Kholili Al-JaloriОценок пока нет
- Atlas of Gastrointestinal Endoscopy and Related PathologyДокумент2 страницыAtlas of Gastrointestinal Endoscopy and Related PathologyMaria PatituОценок пока нет
- History of Physiological Psychology PDFДокумент14 страницHistory of Physiological Psychology PDFYusril Abdan Nur100% (1)
- The Indian Haunting at Malibu Canyon - Book #6 of Freddie Brenner's Mystical AdventuresДокумент25 страницThe Indian Haunting at Malibu Canyon - Book #6 of Freddie Brenner's Mystical AdventuresDr. Kathy Forti100% (2)
- LT 2 Members: Raazia Jalil, Ali Amjad & Ali Raza: Project 2 Doctors InterviewДокумент3 страницыLT 2 Members: Raazia Jalil, Ali Amjad & Ali Raza: Project 2 Doctors InterviewfatimaОценок пока нет
- Understanding Basics of EKG: by Alula A. (R III)Документ37 страницUnderstanding Basics of EKG: by Alula A. (R III)sky nutsОценок пока нет
- Assignment 1Документ13 страницAssignment 1林佑邦Оценок пока нет
- Blood Vessels and Circulation 1Документ36 страницBlood Vessels and Circulation 1Kuya RnJОценок пока нет
- Ointment Box OutlineДокумент1 страницаOintment Box OutlineDon Nestor Razon Jr.Оценок пока нет
- T 1234029783 11845985 Nursing Crib Com Nursing Care Plan Dengue FeverДокумент2 страницыT 1234029783 11845985 Nursing Crib Com Nursing Care Plan Dengue Feversamantha cortezОценок пока нет
- Ayuvediya Approch Toward Iron Deficiency Anaemia - A Case StudyДокумент4 страницыAyuvediya Approch Toward Iron Deficiency Anaemia - A Case StudyIJAR JOURNALОценок пока нет
- Carrubba Botanical Guide RДокумент247 страницCarrubba Botanical Guide Rafridikhanjan100% (3)
- KS4 Physical Education: The Circulatory SystemДокумент36 страницKS4 Physical Education: The Circulatory SystemAjay Pal NattОценок пока нет
- Hunter2019 PDFДокумент15 страницHunter2019 PDFCarlos Andrés BernalОценок пока нет
- Screening Questionnaire: Dha Eligibility LetterДокумент2 страницыScreening Questionnaire: Dha Eligibility LetterDr. Emad Elbadawy د عماد البدويОценок пока нет