Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Alice Hoffman - Green AngelДокумент24 страницыAlice Hoffman - Green AngelHristiyana Yotova71% (14)
- USMLE Step 1 Board Exam High Yield Anatomy For MedicineДокумент7 страницUSMLE Step 1 Board Exam High Yield Anatomy For Medicinesirp328100% (2)
- NBME Answer With Explanation in DepthДокумент10 страницNBME Answer With Explanation in DepthDejan Zolak100% (3)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- E2309 137950-1Документ8 страницE2309 137950-1Sarvesh MishraОценок пока нет
- Empower Your PenisДокумент32 страницыEmpower Your Penisdakkid64% (22)
- Success-On-The-Wards For 3rd Year RotationДокумент82 страницыSuccess-On-The-Wards For 3rd Year RotationthescarletpimpernelsОценок пока нет
- How To Study USMLE Step 1 - 42 DaysДокумент43 страницыHow To Study USMLE Step 1 - 42 Daysnovatj100% (1)
- Hypothesis: Lipoprotein (A) Is A Surrogate For AscorbateДокумент4 страницыHypothesis: Lipoprotein (A) Is A Surrogate For AscorbateDejan ZolakОценок пока нет
- Vitamin C How To Use The Great Missing VitaminДокумент4 страницыVitamin C How To Use The Great Missing VitaminDejan ZolakОценок пока нет
- A Path To Usmle PDFДокумент70 страницA Path To Usmle PDFPriya Arun100% (2)
- MUSCULAR PATHOLOGIES Which Have and Which Do Not Have Elevated CKДокумент1 страницаMUSCULAR PATHOLOGIES Which Have and Which Do Not Have Elevated CKDejan ZolakОценок пока нет
- Leo (Step 1 264)Документ5 страницLeo (Step 1 264)IAMSANWAR019170100% (1)
- How To Study USMLE Step 1 - 42 DaysДокумент43 страницыHow To Study USMLE Step 1 - 42 Daysnovatj100% (1)
- Your Kaplan Medical Timeline PDFДокумент6 страницYour Kaplan Medical Timeline PDFDejan ZolakОценок пока нет
- Medical Ethic More Then 100casesДокумент30 страницMedical Ethic More Then 100casesDejan ZolakОценок пока нет
- Behavioral ScienceДокумент28 страницBehavioral ScienceGeorge HananiaОценок пока нет
- Anatomy Aid Anatomy Aid (86592)Документ9 страницAnatomy Aid Anatomy Aid (86592)Aladdin Ali Abu DanielОценок пока нет
- First Aid Microbiologz Flashcards Part 1Документ12 страницFirst Aid Microbiologz Flashcards Part 1Dejan ZolakОценок пока нет
- Anatomy Aid Anatomy Aid (86592)Документ9 страницAnatomy Aid Anatomy Aid (86592)Aladdin Ali Abu DanielОценок пока нет
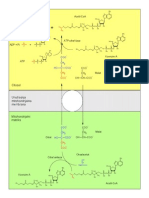
- Transport Acetil CoAДокумент1 страницаTransport Acetil CoADejan ZolakОценок пока нет
- Anatomy Aid Anatomy Aid (86592)Документ9 страницAnatomy Aid Anatomy Aid (86592)Aladdin Ali Abu DanielОценок пока нет
- Varenje Amiloze, Amilopektina, GlikogenaДокумент1 страницаVarenje Amiloze, Amilopektina, GlikogenaDejan ZolakОценок пока нет
- In Sunni IslamДокумент5 страницIn Sunni IslamMk AkangbeОценок пока нет
- Assessing Learning Methods and TestsДокумент2 страницыAssessing Learning Methods and TestsZarah Joyce SegoviaОценок пока нет
- ManipalCigna Active Retail Hospital Network List as on 01 Apr 2022Документ415 страницManipalCigna Active Retail Hospital Network List as on 01 Apr 2022sanjay kumarОценок пока нет
- Commercial Bank of Africa Market ResearchДокумент27 страницCommercial Bank of Africa Market Researchprince185Оценок пока нет
- ENG01P001S02U00Документ14 страницENG01P001S02U00arghasen2014100% (1)
- ID Rekonstruksi Sistem Birokrasi PertanahanДокумент24 страницыID Rekonstruksi Sistem Birokrasi PertanahanMuhammad FakhriОценок пока нет
- Ansys Geotechnical Geology - Finite Element ModelingДокумент25 страницAnsys Geotechnical Geology - Finite Element ModelingvishnuОценок пока нет
- One, Two and Three PerspectiveДокумент10 страницOne, Two and Three PerspectiveNikko Bait-itОценок пока нет
- 1 Unpacking The SelfДокумент13 страниц1 Unpacking The SelfJEMABEL SIDAYENОценок пока нет
- Ethics Module 1-7Документ57 страницEthics Module 1-7Maey RoledaОценок пока нет
- Holy Trinity University: Puerto Princesa City Basic Education DepartmentДокумент2 страницыHoly Trinity University: Puerto Princesa City Basic Education DepartmentBrian Reyes GangcaОценок пока нет
- Ch5 Multivariate MethodsДокумент26 страницCh5 Multivariate MethodsRikiОценок пока нет
- The CIA Tavistock Institute and The GlobalДокумент34 страницыThe CIA Tavistock Institute and The GlobalAnton Crellen100% (4)
- How To Download Cosmetic Injection Techniques A Text and Video Guide To Neurotoxins Fillers Ebook PDF Docx Kindle Full ChapterДокумент36 страницHow To Download Cosmetic Injection Techniques A Text and Video Guide To Neurotoxins Fillers Ebook PDF Docx Kindle Full Chapterkerri.kite140100% (23)
- ISO/IEC 20000 Lead Implementer Course (5 Days)Документ3 страницыISO/IEC 20000 Lead Implementer Course (5 Days)rohitbanerjeeОценок пока нет
- Clinical Study of Incidence of Extraocular Foreign Bodies in Teritiary HospitalДокумент5 страницClinical Study of Incidence of Extraocular Foreign Bodies in Teritiary HospitalIJAR JOURNALОценок пока нет
- Assessing The NeckДокумент3 страницыAssessing The NeckAnne Joyce Lara AlbiosОценок пока нет
- Eight Principles of Ethical Leadership in EducationДокумент2 страницыEight Principles of Ethical Leadership in EducationKimberly Rose Nativo100% (1)
- Learning Disabilities in The ClassroomДокумент5 страницLearning Disabilities in The ClassroomekielaszekОценок пока нет
- November 2008Документ14 страницNovember 2008Aldrin ThomasОценок пока нет
- Florence NightingaleДокумент11 страницFlorence NightingaleSharmaine Palattao LappayОценок пока нет
- ĐỀ CHUẨN MINH HỌA SỐ 03Документ17 страницĐỀ CHUẨN MINH HỌA SỐ 03Lê Thị Ngọc ÁnhОценок пока нет
- ChaseDream Business School Guide LBS - ZH-CN - enДокумент27 страницChaseDream Business School Guide LBS - ZH-CN - enRafael LimaОценок пока нет
- Dilo SpaДокумент2 страницыDilo SpajosefОценок пока нет
- Gajendra-Moksha HTMLДокумент7 страницGajendra-Moksha HTMLankitОценок пока нет
- Module 1 Sociological PerspectivesДокумент39 страницModule 1 Sociological PerspectivesCristine BalocaОценок пока нет
- Description Text About Cathedral Church Jakarta Brian Evan X MIPA 2Документ2 страницыDescription Text About Cathedral Church Jakarta Brian Evan X MIPA 2Brian KristantoОценок пока нет