Вам также может понравиться
- Six Building Blocks of Health SystemДокумент19 страницSix Building Blocks of Health Systemrajucha67% (6)
- 2016 Convocation Brochure JHSPHДокумент52 страницы2016 Convocation Brochure JHSPHPriyo DjatmikoОценок пока нет
- Emergency MedДокумент4 страницыEmergency MedbencleeseОценок пока нет
- Case Report Miliary TuberculosisДокумент20 страницCase Report Miliary Tuberculosissrijelita marbunОценок пока нет
- Tuberculosis - Disease Management - CompДокумент17 страницTuberculosis - Disease Management - CompAhsan kamalОценок пока нет
- Nursing Care Management 103 Cap MRДокумент9 страницNursing Care Management 103 Cap MRkarenfaye00Оценок пока нет
- TB Case HistoryДокумент4 страницыTB Case HistoryMarisa PetersonОценок пока нет
- Tuberculosis ICD-10 A15-A19: Dr. Nadia Aziz C.A.B.C.M Department of Community Medicine Baghdad Medical CollegeДокумент58 страницTuberculosis ICD-10 A15-A19: Dr. Nadia Aziz C.A.B.C.M Department of Community Medicine Baghdad Medical CollegeMazinОценок пока нет
- Clinical Presentation and Diagnosis of Pneumocystis Pulmonary Infection in HIVДокумент42 страницыClinical Presentation and Diagnosis of Pneumocystis Pulmonary Infection in HIVmariano villavicencioОценок пока нет
- Jurnal Bahasa InggrisДокумент12 страницJurnal Bahasa InggrisVanessa Angelica SitepuОценок пока нет
- HepatitisДокумент18 страницHepatitismaheen aurangzaibОценок пока нет
- Peritoneal Tuberculosis: ReviewДокумент5 страницPeritoneal Tuberculosis: ReviewEvellyna MeilanyОценок пока нет
- Case Study PcapДокумент3 страницыCase Study PcapClaire PalaciosОценок пока нет
- CS TBДокумент16 страницCS TB025 MUHAMAD HAZIQ BIN AHMAD AZMANОценок пока нет
- 2017 Sept ReviewДокумент7 страниц2017 Sept ReviewJem QuintoОценок пока нет
- A 45-Year-Old Man With Shortness of Breath, Cough, and Fever BackgroundДокумент7 страницA 45-Year-Old Man With Shortness of Breath, Cough, and Fever BackgroundFluffyyy BabyyyОценок пока нет
- Pulmonary TuberculosisДокумент19 страницPulmonary TuberculosisKristinelou Marie ReynaОценок пока нет
- Infectious Disease Chapter Five Mycobacterial DiseasesДокумент47 страницInfectious Disease Chapter Five Mycobacterial DiseasesHasrul RosliОценок пока нет
- DR As TuberculosisДокумент59 страницDR As TuberculosisAchhar SinghОценок пока нет
- Chronic CoughДокумент4 страницыChronic CoughlalitrajindoliaОценок пока нет
- TuberculosisДокумент5 страницTuberculosismeraj.jaleel250Оценок пока нет
- 1b. TBP & VIHДокумент4 страницы1b. TBP & VIHRaida Uceda GarniqueОценок пока нет
- Shingadia 2003Документ9 страницShingadia 2003syifa fileОценок пока нет
- TUBERCULOSIS Imaging ManifestationsДокумент21 страницаTUBERCULOSIS Imaging ManifestationsEdgard Eduardo Azañero EstradaОценок пока нет
- Tuberculosis: BackgroundДокумент25 страницTuberculosis: BackgroundLuis Alberto Basurto RomeroОценок пока нет
- DR Budi Enoch SPPDДокумент29 страницDR Budi Enoch SPPDMuhammad Iyhan NuriansyahОценок пока нет
- Bronquiectasias Revision 2016 MEdicineДокумент7 страницBronquiectasias Revision 2016 MEdicinerecursitaОценок пока нет
- Pneumonia With Pleural EffusionДокумент24 страницыPneumonia With Pleural EffusionMund CheleОценок пока нет
- TB SeminarДокумент67 страницTB Seminarnewlife.toshi.harneОценок пока нет
- Clinical Manifestations and Complications of Pulmonary Tuberculosis - UpToDateДокумент20 страницClinical Manifestations and Complications of Pulmonary Tuberculosis - UpToDatedixama9519Оценок пока нет
- Diagnostic Standards and Classification of Tuberculosis: CDC WonderДокумент20 страницDiagnostic Standards and Classification of Tuberculosis: CDC Wondereloi moliОценок пока нет
- Bacterial PneumoniaДокумент19 страницBacterial PneumoniaAryo DirgantaraОценок пока нет
- Current Medical Management of Pulmonary TuberculosisДокумент9 страницCurrent Medical Management of Pulmonary TuberculosisFaradilla FirdausaОценок пока нет
- Eraksoy2021 PDFДокумент20 страницEraksoy2021 PDFAnita RahmawatiОценок пока нет
- Community Acquired PneumoniaДокумент4 страницыCommunity Acquired PneumoniaKenPedreso100% (2)
- Tuberculosis PowerpointДокумент69 страницTuberculosis PowerpointCeline Villo100% (1)
- Thesis Pulmonary TuberculosisДокумент5 страницThesis Pulmonary TuberculosisDoMyPaperCanada100% (2)
- Research Paper TuberculosisДокумент5 страницResearch Paper Tuberculosispeputaqlg100% (1)
- TuberculosisДокумент4 страницыTuberculosisDr Mangesti Utami PKM Kebaman BanyuwangiОценок пока нет
- Multi Drug Resistant TBДокумент28 страницMulti Drug Resistant TBmedeviОценок пока нет
- Etiologies of Fever of Unknown Origin in Adults - UpToDate (2019) PDFДокумент17 страницEtiologies of Fever of Unknown Origin in Adults - UpToDate (2019) PDFMoisés León RuizОценок пока нет
- Fact Sheet - PneumoniaДокумент9 страницFact Sheet - PneumoniaAbdelrahman AlshatnawiОценок пока нет
- Ascitits BKДокумент16 страницAscitits BKAjengОценок пока нет
- EBR Format For StudentsДокумент1 страницаEBR Format For StudentsAPRIL GWEN DALAGANОценок пока нет
- Case Study Group 4 - XI IPAДокумент15 страницCase Study Group 4 - XI IPAkeisya angОценок пока нет
- TuberculosisДокумент20 страницTuberculosisBader AljarboaОценок пока нет
- IM GRP 3Документ11 страницIM GRP 3Dale Maninantan De DiosОценок пока нет
- Case 1Документ3 страницыCase 1maralgoo.medОценок пока нет
- Pulmonary Tuberculosis Presenting With Acute Respiratory Distress Syndrome (Ards) : A Case Report and Review of LiteratureДокумент5 страницPulmonary Tuberculosis Presenting With Acute Respiratory Distress Syndrome (Ards) : A Case Report and Review of Literatureamelya asryОценок пока нет
- Ncbi - Nlm.nih - Gov-Pediatric PneumoniaДокумент10 страницNcbi - Nlm.nih - Gov-Pediatric Pneumoniako naythweОценок пока нет
- Final Case Study of Cap EditДокумент50 страницFinal Case Study of Cap EditBem Bem Kai Hinoguin100% (1)
- AJRM MARCH PP 5-7Документ3 страницыAJRM MARCH PP 5-7Vito Sahala TobiasОценок пока нет
- Case Study On Communicable DiseaseДокумент15 страницCase Study On Communicable DiseaseThiradevi BalakrisnanОценок пока нет
- Nosocomial Pneumonia: Self AssessmentДокумент10 страницNosocomial Pneumonia: Self AssessmentZali AhmadОценок пока нет
- READINGS PcapДокумент2 страницыREADINGS PcapEden RelacionОценок пока нет
- Tuberculosis Thesis StatementДокумент7 страницTuberculosis Thesis Statementrqopqlvcf100% (2)
- Pulmonary Tuberculosis Research PaperДокумент6 страницPulmonary Tuberculosis Research Paperutwvgkxgf100% (1)
- HIV and The Lung 2013Документ7 страницHIV and The Lung 2013Katherin J.Оценок пока нет
- Bronchiectasis: A Guide For Primary CareДокумент10 страницBronchiectasis: A Guide For Primary CareJuwitaОценок пока нет
- Tuberculosis in ChildrenДокумент4 страницыTuberculosis in ChildrenMarthin TheservantОценок пока нет
- StillbirthДокумент27 страницStillbirthJoseph Nawen SindiongОценок пока нет
- Reynier AssignmentДокумент1 страницаReynier AssignmentJoseph Nawen SindiongОценок пока нет
- Case Study LabДокумент5 страницCase Study LabJoseph Nawen SindiongОценок пока нет
- Physical Examination NewДокумент3 страницыPhysical Examination NewJoseph Nawen SindiongОценок пока нет
- Nursing Care PlanДокумент2 страницыNursing Care PlanJoseph Nawen Sindiong100% (1)
- Drugs Used in Pregnancy-Induced Hypertension: Drug Indication Dosage CommentsДокумент1 страницаDrugs Used in Pregnancy-Induced Hypertension: Drug Indication Dosage CommentsJoseph Nawen SindiongОценок пока нет
- Topic DiscussionДокумент7 страницTopic DiscussionJoseph Nawen SindiongОценок пока нет
- ProQuestDocuments 2016-09-22Документ4 страницыProQuestDocuments 2016-09-22Joseph Nawen SindiongОценок пока нет
- Workplan AugustДокумент4 страницыWorkplan AugustJoseph Nawen SindiongОценок пока нет
- Workplan AugustДокумент4 страницыWorkplan AugustJoseph Nawen SindiongОценок пока нет
- PesДокумент2 страницыPesJoseph Nawen SindiongОценок пока нет
- Nursing StudentsДокумент14 страницNursing StudentsJoseph Nawen SindiongОценок пока нет
- NurseДокумент2 страницыNurseJoseph Nawen SindiongОценок пока нет
- Proposed Activities and Advanced Work Plan - Docx2Документ4 страницыProposed Activities and Advanced Work Plan - Docx2Joseph Nawen SindiongОценок пока нет
- Table of ContentsДокумент2 страницыTable of ContentsJoseph Nawen SindiongОценок пока нет
- Nursing Care PlanДокумент2 страницыNursing Care PlanJoseph Nawen Sindiong100% (1)
- Table of ContentsДокумент2 страницыTable of ContentsJoseph Nawen SindiongОценок пока нет
- Mission Aims To Provide Accessible, Cost Effective, Competitive and Efficient Primary Health Care For The Resident of Barangay Bawang VisionДокумент1 страницаMission Aims To Provide Accessible, Cost Effective, Competitive and Efficient Primary Health Care For The Resident of Barangay Bawang VisionJoseph Nawen SindiongОценок пока нет
- Topic DiscussionДокумент7 страницTopic DiscussionJoseph Nawen SindiongОценок пока нет
- Physical Examination NewДокумент3 страницыPhysical Examination NewJoseph Nawen SindiongОценок пока нет
- Key Words: Case Study, Pregnancy Induced Hypertension, ManagementДокумент1 страницаKey Words: Case Study, Pregnancy Induced Hypertension, ManagementJoseph Nawen SindiongОценок пока нет
- A Case Study of A Primigravida With Pregnancy-Induced HypertensionДокумент1 страницаA Case Study of A Primigravida With Pregnancy-Induced HypertensionJoseph Nawen SindiongОценок пока нет
- Acknowledgement: Sibugay GroupДокумент1 страницаAcknowledgement: Sibugay GroupJoseph Nawen SindiongОценок пока нет
- INTROДокумент73 страницыINTROJoseph Nawen SindiongОценок пока нет
- Chapter IДокумент3 страницыChapter IJoseph Nawen SindiongОценок пока нет
- Key Words: Case Study, Pregnancy Induced Hypertension, ManagementДокумент1 страницаKey Words: Case Study, Pregnancy Induced Hypertension, ManagementJoseph Nawen SindiongОценок пока нет
- Sample Content ValidationДокумент2 страницыSample Content ValidationJoseph Nawen SindiongОценок пока нет
- Joseph Nawen M Reflection PaperДокумент2 страницыJoseph Nawen M Reflection PaperJoseph Nawen SindiongОценок пока нет
- Review of Related LiteratureДокумент2 страницыReview of Related LiteratureJoseph Nawen SindiongОценок пока нет
- Hiv AidsДокумент41 страницаHiv AidsNela Rosa Harianja100% (1)
- Islamic Relief South Africa: Gaza Medical Aid AppealДокумент7 страницIslamic Relief South Africa: Gaza Medical Aid AppealShanaaz Ebrahim GireОценок пока нет
- On MCH and Maternal Health in BangladeshДокумент46 страницOn MCH and Maternal Health in BangladeshTanni ChowdhuryОценок пока нет
- Grand RevalidaДокумент342 страницыGrand RevalidaJoeОценок пока нет
- Fluorescent Treponemal Antibody Absorption FTA ABS TestДокумент22 страницыFluorescent Treponemal Antibody Absorption FTA ABS TestMekar PalupiОценок пока нет
- 2013 Article 326Документ8 страниц2013 Article 326Ariyati MandiriОценок пока нет
- Annual Report 2009 10Документ189 страницAnnual Report 2009 10tkhalifaОценок пока нет
- Boost Your PA ProtectionДокумент22 страницыBoost Your PA ProtectionLogen TiranОценок пока нет
- Plummer - Male SexualitiesДокумент18 страницPlummer - Male SexualitiesmargitajemrtvaОценок пока нет
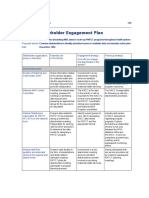
- Sample Stakeholder Engagement PlanДокумент3 страницыSample Stakeholder Engagement PlanMonique Ruste100% (2)
- Candida VulvovaginitisДокумент29 страницCandida VulvovaginitisPepe VizcarraОценок пока нет
- SEMINAR-Clinical Microbiology: Topic-Human Immuno-Deficiency Virus (HIV)Документ54 страницыSEMINAR-Clinical Microbiology: Topic-Human Immuno-Deficiency Virus (HIV)sushant_dharОценок пока нет
- Dengue Fever and Other Hemorrhagic Viruses (Deadly Diseases and Epidemics) - T. Chakraborty (Chelsea House, 2008) WW PDFДокумент103 страницыDengue Fever and Other Hemorrhagic Viruses (Deadly Diseases and Epidemics) - T. Chakraborty (Chelsea House, 2008) WW PDFLavinia GeorgianaОценок пока нет
- Digumarti Bhaskara RaoДокумент22 страницыDigumarti Bhaskara Raodbrao100% (3)
- AIMS and OBJECTIVES Communty Services ReportДокумент2 страницыAIMS and OBJECTIVES Communty Services ReportAlwyn Luva ChikonoОценок пока нет
- Mycobacterium LectureДокумент39 страницMycobacterium LectureDegee GonzalesОценок пока нет
- Faktor Yang Mempengaruhi Ketidakteraturan Berobat Penderita TB Paru Di Puskesmas Kota Binjai Tahun 2004Документ21 страницаFaktor Yang Mempengaruhi Ketidakteraturan Berobat Penderita TB Paru Di Puskesmas Kota Binjai Tahun 2004jojor simamoraОценок пока нет
- County Health Strategic and Investment Plan 2013 - 2018Документ96 страницCounty Health Strategic and Investment Plan 2013 - 2018api-258641606100% (1)
- AHF Sierra Leone EOI For Engineering Firms - 2021 (LC Comments)Документ3 страницыAHF Sierra Leone EOI For Engineering Firms - 2021 (LC Comments)Samuel WilliamsОценок пока нет
- Including Proper Education in Every Student's BackpackДокумент1 страницаIncluding Proper Education in Every Student's BackpackBlesshy Feb Melecio VisitacionОценок пока нет
- 376 - Marine Sponges As PharmacyДокумент21 страница376 - Marine Sponges As PharmacyshemishamzОценок пока нет
- What Will Life Be Like in 2050Документ2 страницыWhat Will Life Be Like in 2050Victor CiupОценок пока нет
- Good Shepherd Hospital (Swaziland) TB Infection Control Policy Dec 2014Документ30 страницGood Shepherd Hospital (Swaziland) TB Infection Control Policy Dec 2014COMDIS-HSDОценок пока нет
- Antifungal AntibioticsДокумент16 страницAntifungal AntibioticsLyadelou FortuОценок пока нет
- AIDS and PeriodontiumДокумент25 страницAIDS and PeriodontiumKarthik Krishna M100% (1)
- Neheng Tankiso CV EnglishДокумент1 страницаNeheng Tankiso CV Englishapi-242563415Оценок пока нет
- Critical Review SampleДокумент3 страницыCritical Review SampleAhmad Muammar100% (1)
- Bisexual Invisibility Impacts and Recommendations (Adopted March 2011)Документ47 страницBisexual Invisibility Impacts and Recommendations (Adopted March 2011)Cecilia C Chung100% (1)