Вам также может понравиться
- Nail Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandNail Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- Mycology Lecture FinalДокумент258 страницMycology Lecture FinalBahaa Shaaban100% (1)
- Dermatomycosis GuideДокумент114 страницDermatomycosis GuideQonita Qurrota AyunОценок пока нет
- Tinea - The DermatophytesДокумент67 страницTinea - The Dermatophytesmansoor aliОценок пока нет
- Fungal Skin Infections ملزمةДокумент6 страницFungal Skin Infections ملزمةعبدالرحمن طارق عبدالله صالحОценок пока нет
- Cutaneous Mycoses GuideДокумент55 страницCutaneous Mycoses GuideAlpana Laisom100% (2)
- Mycology: Clinical FindingsДокумент5 страницMycology: Clinical FindingsLuqman Al-Bashir FauziОценок пока нет
- Fungal InfectionsДокумент42 страницыFungal InfectionsleenaloveuОценок пока нет
- Superficial Fungal Infections ExplainedДокумент69 страницSuperficial Fungal Infections Explainedputri.SpAОценок пока нет
- The Diagnosis and Management of Tinea CapitisДокумент4 страницыThe Diagnosis and Management of Tinea CapitisKeyla Kehara PutriОценок пока нет
- Tinea Corporis Pedia-1Документ11 страницTinea Corporis Pedia-1Denso Antonius LimОценок пока нет
- The Diagnosis and Management Of: Tinea CapitisДокумент4 страницыThe Diagnosis and Management Of: Tinea CapitisQuraisy jamal sahilОценок пока нет
- Superficial MycosisДокумент8 страницSuperficial MycosisLuqman Al-Bashir FauziОценок пока нет
- Fungal Skin Infections-1Документ27 страницFungal Skin Infections-1Fabb Nelson100% (1)
- Ringworm (Tinea Capitis)Документ15 страницRingworm (Tinea Capitis)farmasi_hmОценок пока нет
- Superficial Fungal InfectionsДокумент40 страницSuperficial Fungal InfectionsMarimuthu PrabhakaranОценок пока нет
- Fungal Skin Infections: Causes, Types and TreatmentsДокумент67 страницFungal Skin Infections: Causes, Types and TreatmentsMedo JT100% (1)
- (JURNAL) Update Terapy MycosesДокумент51 страница(JURNAL) Update Terapy MycosesHabibah Nurla LumiereОценок пока нет
- Chapter 4Документ103 страницыChapter 4tenaw100% (1)
- Fungal InfectionsДокумент9 страницFungal InfectionsCoral Srinivasa RamaluОценок пока нет
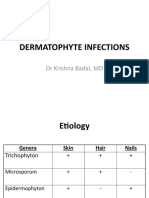
- Dermatophyte InfectionsДокумент41 страницаDermatophyte Infectionsshoaib khanОценок пока нет
- DermatophytesДокумент42 страницыDermatophytesማላያላም ማላያላም100% (1)
- Tinea Barbae Is A Rare Dermatophytic Infection That Is Limited To The Bearded Areas of The FaceДокумент3 страницыTinea Barbae Is A Rare Dermatophytic Infection That Is Limited To The Bearded Areas of The FaceMardiah Nurul HasanahОценок пока нет
- Ringworm Guide: Symptoms, Types, and TreatmentДокумент5 страницRingworm Guide: Symptoms, Types, and TreatmentAnnisa SyaflianiОценок пока нет
- Tinea CapitisДокумент9 страницTinea CapitisadityakafiberkahsmgОценок пока нет
- MycosesДокумент2 страницыMycosesMadabout MusicОценок пока нет
- Bacterial Skin InfectionsДокумент4 страницыBacterial Skin InfectionsFiras HamidehОценок пока нет
- Tinea Barbae Is A Rare Dermatophytic Infection That Is Limited To The Bearded Areas of The FaceДокумент5 страницTinea Barbae Is A Rare Dermatophytic Infection That Is Limited To The Bearded Areas of The Facemardiah nurulОценок пока нет
- Fungal InfectionДокумент114 страницFungal InfectionAini Shofa Haniah100% (1)
- Guide to Fungal Skin Infections (DermatomycosisДокумент128 страницGuide to Fungal Skin Infections (DermatomycosisDevy KurniawatiОценок пока нет
- Fungal Infections of the Skin and NailsДокумент22 страницыFungal Infections of the Skin and NailsDragon Gie30Оценок пока нет
- Superficial MycosesДокумент26 страницSuperficial Mycosesdhainey100% (3)
- 004 - PyodermasДокумент67 страниц004 - PyodermasLucas Victor AlmeidaОценок пока нет
- Medical MycologyДокумент14 страницMedical Mycologyhawkar omerОценок пока нет
- Dermatomycosis 18th July 2021Документ120 страницDermatomycosis 18th July 2021Sekar OktaviaОценок пока нет
- Mycopedis 2017Документ110 страницMycopedis 2017Ahmed RadwanОценок пока нет
- K7 Jamur Superficial 2020Документ51 страницаK7 Jamur Superficial 2020Jimmy Fran IIОценок пока нет
- MYCOSESДокумент41 страницаMYCOSESDayana PrasanthОценок пока нет
- Tinea Capitis: Fungal Infection of the ScalpДокумент16 страницTinea Capitis: Fungal Infection of the ScalpIkram IkramОценок пока нет
- Tinea Capitis Favus-Like Appearance: Problem of Diagnosis: Dwi Ratna Adisty, Linda AstariДокумент7 страницTinea Capitis Favus-Like Appearance: Problem of Diagnosis: Dwi Ratna Adisty, Linda AstarihaningpradyОценок пока нет
- DermatophyteДокумент8 страницDermatophyteBhuvana RajОценок пока нет
- Superficial Fungal InfectionДокумент24 страницыSuperficial Fungal InfectionzakiОценок пока нет
- Tine AДокумент6 страницTine AMemo AliОценок пока нет
- Tinea CapitisДокумент7 страницTinea Capitismufidah nurfajОценок пока нет
- Acute Otitis Media: Definition, Causes, Symptoms, TreatmentДокумент3 страницыAcute Otitis Media: Definition, Causes, Symptoms, TreatmentMalvinder Singh DhillonОценок пока нет
- Fungal Pathogens GroupingsДокумент25 страницFungal Pathogens GroupingsJhade Rio GadinganОценок пока нет
- Diagnosis and Management of Common Tinea InfectionsДокумент23 страницыDiagnosis and Management of Common Tinea InfectionsGiovanni AnggastaОценок пока нет
- BAHAN Tinea CapitisДокумент28 страницBAHAN Tinea CapitisYorika HafelaniОценок пока нет
- Tinea Capitis Inggris CKДокумент3 страницыTinea Capitis Inggris CKBhagawanta AptakayanaОценок пока нет
- Tinea capitis causes and treatmentДокумент10 страницTinea capitis causes and treatmentSyamsul ArifinОценок пока нет
- Fungal & Parasitic Infestations of The SkinДокумент67 страницFungal & Parasitic Infestations of The SkinGhaith HamdiОценок пока нет
- Fungal Infections - InfestationsДокумент48 страницFungal Infections - InfestationsMoayad NawaflehОценок пока нет
- Dermatophytosis: LectureДокумент35 страницDermatophytosis: LectureGideon MukalaziОценок пока нет
- Cutaneous Mycoses Guide: Classification, Agents and Clinical ManifestationsДокумент56 страницCutaneous Mycoses Guide: Classification, Agents and Clinical ManifestationsHafsa ImranОценок пока нет
- Jamur-Jamur Penyebab: Mikosis Superfisial Dermatofitosis Mikosis SubkutanДокумент104 страницыJamur-Jamur Penyebab: Mikosis Superfisial Dermatofitosis Mikosis SubkutanJimmy Fran IIОценок пока нет
- Derma LMRДокумент11 страницDerma LMRadiОценок пока нет
- The Kerion An Angry Tinea Capitis PBДокумент7 страницThe Kerion An Angry Tinea Capitis PBprajnamitaОценок пока нет
- ImpetigoДокумент21 страницаImpetigoHanif GandohОценок пока нет
- Kata PengantarДокумент21 страницаKata PengantarKartika RosyahОценок пока нет
- Classification of Fungal InfectionsДокумент26 страницClassification of Fungal Infectionstev26Оценок пока нет
- Serial KeyДокумент1 страницаSerial KeyFiras HamidehОценок пока нет
- Bacterial Skin InfectionsДокумент4 страницыBacterial Skin InfectionsFiras HamidehОценок пока нет
- Filler Course MaterialДокумент106 страницFiller Course MaterialFiras HamidehОценок пока нет
- Read MeДокумент1 страницаRead MeFiras HamidehОценок пока нет
- 2013Документ4 страницы2013Firas HamidehОценок пока нет
- Bullos DiseaseДокумент4 страницыBullos DiseaseFiras HamidehОценок пока нет
- Cutaneous LymphomasДокумент1 страницаCutaneous LymphomasFiras HamidehОценок пока нет
- Cutaneous LymphomasДокумент1 страницаCutaneous LymphomasFiras HamidehОценок пока нет
- Cutaneous LymphomasДокумент1 страницаCutaneous LymphomasFiras HamidehОценок пока нет
- Acne VulgarisДокумент2 страницыAcne VulgarisFiras HamidehОценок пока нет
- Benign TumorsДокумент4 страницыBenign TumorsFiras HamidehОценок пока нет
- Functional DysphoniaДокумент5 страницFunctional DysphoniaCati GallardoОценок пока нет
- 1494870C 9912 C184 4CC9 B401 A53f4d8de290Документ5 страниц1494870C 9912 C184 4CC9 B401 A53f4d8de290Firas HamidehОценок пока нет
- 1494870C 9912 C184 4CC9 B401 A53f4d8de290 PDFДокумент1 страница1494870C 9912 C184 4CC9 B401 A53f4d8de290 PDFAngelo ZambranoОценок пока нет
- ReleaseNote FileList of T200TA WIN10 32 V1.00Документ2 страницыReleaseNote FileList of T200TA WIN10 32 V1.00Firas HamidehОценок пока нет
- Tablet Mobile Dock: Asus AsusДокумент108 страницTablet Mobile Dock: Asus AsusFiras HamidehОценок пока нет
- Functional DysphoniaДокумент5 страницFunctional DysphoniaCati GallardoОценок пока нет
- Functional Dysphonia 2Документ1 страницаFunctional Dysphonia 2Firas HamidehОценок пока нет
- Klasifikasi InfluenzaДокумент33 страницыKlasifikasi InfluenzaLike Radjalabis100% (1)
- WA Tuberculosis Control Program BCG Vaccination GuideДокумент3 страницыWA Tuberculosis Control Program BCG Vaccination GuideAdham MisdarОценок пока нет
- Timeout PosterДокумент2 страницыTimeout Posterapi-138096780100% (1)
- Prevent COVID-19: A Guide to Awareness and PreventionДокумент22 страницыPrevent COVID-19: A Guide to Awareness and PreventionGirjesh VishwakarmaОценок пока нет
- Smallpox Pamphlet Group 2Документ3 страницыSmallpox Pamphlet Group 2classdocsОценок пока нет
- EPI Program Principles Immunization DiseasesДокумент4 страницыEPI Program Principles Immunization DiseasesSarahLabadan67% (3)
- Epidemics and PandemicsДокумент36 страницEpidemics and PandemicsRusu CristianaОценок пока нет
- EPI Program Goals Immunize Children Against DiseasesДокумент5 страницEPI Program Goals Immunize Children Against DiseasesStephen EleserioОценок пока нет
- VPD Report 2019 MayДокумент12 страницVPD Report 2019 MaystprepsОценок пока нет
- Coronavirus Reading Comprehension WorksheetДокумент5 страницCoronavirus Reading Comprehension WorksheetDorina Crețu100% (1)
- Public Health CampaignsДокумент1 страницаPublic Health Campaignsরাজর্ষীОценок пока нет
- Transfusion Transmitted InfectionsДокумент30 страницTransfusion Transmitted InfectionsSadio KeitaОценок пока нет
- Platelet Activation in Adult HIV-infectedДокумент35 страницPlatelet Activation in Adult HIV-infectedbokobokobokanОценок пока нет
- John Jay Immunization FormДокумент3 страницыJohn Jay Immunization FormIsam BoukattayaОценок пока нет
- Single Congenital AbnormalitiesДокумент5 страницSingle Congenital AbnormalitiesTrangPhamОценок пока нет
- Major Infectious Diseases by TypeДокумент1 страницаMajor Infectious Diseases by TypeDilipsingh RajputОценок пока нет
- Worksheet For Aids and HivДокумент3 страницыWorksheet For Aids and HivSarika AhujaОценок пока нет
- SpirocheteДокумент32 страницыSpirocheteSAYMABANU100% (1)
- Bovine Viral Diarrhoea: BVD Is A Sub Acute, Acute or INAPPARENT Contagious Disease Characterized byДокумент27 страницBovine Viral Diarrhoea: BVD Is A Sub Acute, Acute or INAPPARENT Contagious Disease Characterized byhari krishnaa athotaОценок пока нет
- Herpes Simplex Virus Types, Transmission, Symptoms & TreatmentДокумент3 страницыHerpes Simplex Virus Types, Transmission, Symptoms & TreatmentkyawОценок пока нет
- EbolaДокумент4 страницыEbolaapi-271224704Оценок пока нет
- Causes, Types & Treatment of Congenital Heart DefectsДокумент2 страницыCauses, Types & Treatment of Congenital Heart Defectsjhayviec0% (1)
- The Flu - Expository EssayДокумент2 страницыThe Flu - Expository EssaytessafikriОценок пока нет
- ViralZone Human VirusesДокумент22 страницыViralZone Human VirusesFalio HarenaОценок пока нет
- Kindly Correlate With Clinical FindingsДокумент2 страницыKindly Correlate With Clinical FindingsAaryaveer KatochОценок пока нет
- Syphilis & Gonorrhea: Other Emerging Community Acquired Sexually Transmitted DiseasesДокумент29 страницSyphilis & Gonorrhea: Other Emerging Community Acquired Sexually Transmitted DiseasesRegine Delos SantosОценок пока нет
- K 6 PertussisДокумент22 страницыK 6 PertussisAnonymous hK8RDoОценок пока нет
- IDSP P&L FormsДокумент2 страницыIDSP P&L FormsKunal YadavОценок пока нет
- SARS (Severe Acute Respiratory Syndrome)Документ5 страницSARS (Severe Acute Respiratory Syndrome)Hazel EstayanОценок пока нет
- DAFTAR PUSTAKA Serologi Dan ImunologiДокумент2 страницыDAFTAR PUSTAKA Serologi Dan ImunologiSari Anggun NОценок пока нет