Вам также может понравиться
- CPC Exam Review QuestionsДокумент3 страницыCPC Exam Review QuestionshevinpatelОценок пока нет
- GTG 55 Late Intrauterine Fetal Death and Stillbirth 10 11 10-2Документ33 страницыGTG 55 Late Intrauterine Fetal Death and Stillbirth 10 11 10-2fahlevyОценок пока нет
- Severe PreeclampsiaДокумент84 страницыSevere PreeclampsiaJm Bernardo50% (2)
- Bronchiolitis in ChildrenДокумент16 страницBronchiolitis in ChildrenDhan RamadhanОценок пока нет
- BMC Pediatrics PregnancyДокумент8 страницBMC Pediatrics PregnancyMobin Ur Rehman KhanОценок пока нет
- 39 Iajps39052018 PDFДокумент5 страниц39 Iajps39052018 PDFiajpsОценок пока нет
- Prevalence of Preeclampsia and The Associated Risk Factors Among Pregnant Women in BangladeshДокумент10 страницPrevalence of Preeclampsia and The Associated Risk Factors Among Pregnant Women in BangladeshNanda Puspita SariОценок пока нет
- Pregnancy Hypertension KnowledgeДокумент3 страницыPregnancy Hypertension Knowledgeazida90Оценок пока нет
- Hyperglycemia in Pregnant Ladies and Its Outcome Out in The Opd, Labor Ward, Gynecology and Obstetrics, Lady Atichison Hospital, LahoreДокумент7 страницHyperglycemia in Pregnant Ladies and Its Outcome Out in The Opd, Labor Ward, Gynecology and Obstetrics, Lady Atichison Hospital, LahoreiajpsОценок пока нет
- An Overview of Referral Patients With Severe Preeclampsia in Obstetric and Gynecology Department, Dr. Soetomo Hospital Surabaya in 2011 An OverviewДокумент10 страницAn Overview of Referral Patients With Severe Preeclampsia in Obstetric and Gynecology Department, Dr. Soetomo Hospital Surabaya in 2011 An OverviewAnonymous y6NmP9NHkYОценок пока нет
- 45 Iajps45052018 PDFДокумент7 страниц45 Iajps45052018 PDFiajpsОценок пока нет
- EclampsiaДокумент8 страницEclampsiaAtef Kamel SalamaОценок пока нет
- Analytical Study of Intrauterine Fetal Death Cases and Associated Maternal ConditionsДокумент5 страницAnalytical Study of Intrauterine Fetal Death Cases and Associated Maternal ConditionsNurvita WidyastutiОценок пока нет
- Jurnal AsliДокумент5 страницJurnal Aslipramono hanumОценок пока нет
- Morbidity Among Infants of Diabetic Mothers in SudanДокумент7 страницMorbidity Among Infants of Diabetic Mothers in SudanAde Gustina Siahaan100% (1)
- 2040 7117 1 PBДокумент8 страниц2040 7117 1 PBrizki ameliaОценок пока нет
- Patient's Profile With Hypertension in Pregnancy PatientsДокумент6 страницPatient's Profile With Hypertension in Pregnancy PatientsHendrik SuTopo LidaprajaОценок пока нет
- Ectopic Pregnancy's Impact on Future FertilityДокумент0 страницEctopic Pregnancy's Impact on Future FertilitynajmulОценок пока нет
- Pre-Eclampsia-Pregnancy Induced Hypertension Threats andДокумент5 страницPre-Eclampsia-Pregnancy Induced Hypertension Threats andSaima KhanОценок пока нет
- Maternal and Fetal Complications in Pregnant Epileptic WomenДокумент5 страницMaternal and Fetal Complications in Pregnant Epileptic WomenMedical Record PPDS OBGINОценок пока нет
- Chapter 3Документ32 страницыChapter 3Vaibhav JainОценок пока нет
- Prevalence of Factors Involved in Intracranial Hemorrhage of Premature Neonates Less Than 34 WeeksДокумент4 страницыPrevalence of Factors Involved in Intracranial Hemorrhage of Premature Neonates Less Than 34 WeeksTriponiaОценок пока нет
- 1 PB PDFДокумент7 страниц1 PB PDFAmanda Mustika AdiОценок пока нет
- Proforma For Registration of Subject For DissertationДокумент33 страницыProforma For Registration of Subject For DissertationRaafi Puristya Aries DarmawanОценок пока нет
- Maternal Outcomes of Severe Preeclampsia Eclampsia and Associated Factorsamong Mothers Admitted in Referral Hospitals NДокумент7 страницMaternal Outcomes of Severe Preeclampsia Eclampsia and Associated Factorsamong Mothers Admitted in Referral Hospitals NtalilaОценок пока нет
- Maternal and Perinatal Outcome in Antepartum HemorrhageДокумент5 страницMaternal and Perinatal Outcome in Antepartum HemorrhagebayukolorОценок пока нет
- GimikДокумент9 страницGimikNanda PuspitaОценок пока нет
- Frequency, Causes and Outcome of PolyhydramniosДокумент4 страницыFrequency, Causes and Outcome of PolyhydramniosMina LelymanОценок пока нет
- Determinan Risk Factor Wich Influence Occurence: The 4 Univesity Research Coloquium 2016 ISSN 2407-9189Документ7 страницDeterminan Risk Factor Wich Influence Occurence: The 4 Univesity Research Coloquium 2016 ISSN 2407-9189nova febrianiОценок пока нет
- Maternal and Perinatal Complications of Severe Preeclampsia in Three Referral Hospitals in Yaoundé, CameroonДокумент8 страницMaternal and Perinatal Complications of Severe Preeclampsia in Three Referral Hospitals in Yaoundé, CameroonIke Istofani KОценок пока нет
- Karakteristik Kehamilan Dengan Luaran Asfiksia Saat Lahir Di RSUP Prof. Dr. R. D. Kandou Manado Periode Januari - Desember 2014Документ7 страницKarakteristik Kehamilan Dengan Luaran Asfiksia Saat Lahir Di RSUP Prof. Dr. R. D. Kandou Manado Periode Januari - Desember 2014Fransiska PareraОценок пока нет
- Study of Sociodemographic Profile, Maternal, Fetal Outcome in Preeclamptic and Eclamptic Women A Prospective StudyДокумент6 страницStudy of Sociodemographic Profile, Maternal, Fetal Outcome in Preeclamptic and Eclamptic Women A Prospective StudyHarvey MatbaganОценок пока нет
- 2851-26. 31 Rasheed Eclampsia-1625840448Документ3 страницы2851-26. 31 Rasheed Eclampsia-1625840448Umair HasanОценок пока нет
- MATERNAL DISEASE-PEB-EclampsiaДокумент10 страницMATERNAL DISEASE-PEB-Eclampsiaari naОценок пока нет
- Artículo Nefro 2Документ6 страницArtículo Nefro 2Stephani RobinsonОценок пока нет
- A Clinical Study of Knowledge and Practice of Anemia Among Pregnant Women Attending Antenatal Clinic at Tertiary HospitalДокумент21 страницаA Clinical Study of Knowledge and Practice of Anemia Among Pregnant Women Attending Antenatal Clinic at Tertiary Hospitalhamsa2020Оценок пока нет
- Abstrak Makalah Bebas MedanДокумент11 страницAbstrak Makalah Bebas Medandr.raziОценок пока нет
- Morbidity and Mortality Amongst Infants of Diabetic Mothers Admitted Into A Special Care Baby Unit in Port Harcourt, NigeriaДокумент6 страницMorbidity and Mortality Amongst Infants of Diabetic Mothers Admitted Into A Special Care Baby Unit in Port Harcourt, Nigeriavighnaharta Online ServicesОценок пока нет
- Afhs0801 0044 2Документ6 страницAfhs0801 0044 2Noval FarlanОценок пока нет
- Case StudyДокумент8 страницCase StudyJay-ann MendozaОценок пока нет
- Incidence and Outcome of Severe Antepartum Hemorrhage at The Teaching Hospital Yalgado Ouédraogo in Burkina FasoДокумент12 страницIncidence and Outcome of Severe Antepartum Hemorrhage at The Teaching Hospital Yalgado Ouédraogo in Burkina Fasoshiffa ramadhantiОценок пока нет
- The Women Perception 2019 of Prevention PreeclampsiДокумент12 страницThe Women Perception 2019 of Prevention PreeclampsisatrioОценок пока нет
- Gambaran Karakteristik Dan Luaran Pada Preeklamsi Awitan Dini Dan Awitan Lanjut Di Rumah Sakit Hasan Sadikin BandungДокумент11 страницGambaran Karakteristik Dan Luaran Pada Preeklamsi Awitan Dini Dan Awitan Lanjut Di Rumah Sakit Hasan Sadikin BandungIndah SetiyaniОценок пока нет
- Idil Fitriani 2Документ6 страницIdil Fitriani 2ZenrizkyОценок пока нет
- Feto-Maternal Outcomes in Hypertensive Disorders of Pregnancy in A Tertiary Care Hospital: A Retrospective StudyДокумент7 страницFeto-Maternal Outcomes in Hypertensive Disorders of Pregnancy in A Tertiary Care Hospital: A Retrospective StudyIJAR JOURNALОценок пока нет
- Pengaruh Komsumsi Kripik Singkong Ebi Terhadap Tekanan Darah Pada Ibu Hamil Hipertensi Kabupaten Maros Tahun 2020Документ12 страницPengaruh Komsumsi Kripik Singkong Ebi Terhadap Tekanan Darah Pada Ibu Hamil Hipertensi Kabupaten Maros Tahun 2020Fiencen ReisaОценок пока нет
- Malaria Dan KeguguranДокумент23 страницыMalaria Dan Keguguranwoouuw0903Оценок пока нет
- Maternal Mortality in Papua New Guinea and Australia: Max Brinsmead MB Bs PHD December 2017Документ24 страницыMaternal Mortality in Papua New Guinea and Australia: Max Brinsmead MB Bs PHD December 2017DrChauhanОценок пока нет
- Evaluation of Risk Factors and Obstetric and Perinatal Outcome in Abruptio PlacentaДокумент4 страницыEvaluation of Risk Factors and Obstetric and Perinatal Outcome in Abruptio PlacentaIOSRjournalОценок пока нет
- Pre-Eclampsia, Eclampsia and Adverse Maternal and Perinatal Outcomes: A Secondary Analysis of The World Health Organization Multicountry Survey On Maternal and Newborn HealthДокумент11 страницPre-Eclampsia, Eclampsia and Adverse Maternal and Perinatal Outcomes: A Secondary Analysis of The World Health Organization Multicountry Survey On Maternal and Newborn HealthMariana CruzОценок пока нет
- Eclampsia: VI. Maternal-Perinatal Outcome in 254 Consecutive CasesДокумент6 страницEclampsia: VI. Maternal-Perinatal Outcome in 254 Consecutive CasesrizkaОценок пока нет
- Diabetes y Embarazo Tipo2 PDFДокумент3 страницыDiabetes y Embarazo Tipo2 PDFFRM2012Оценок пока нет
- Pregnancy Complications and Outcomes in Women With Epilepsy: Mirzaei Fatemeh, Ebrahimi B. NazaninДокумент5 страницPregnancy Complications and Outcomes in Women With Epilepsy: Mirzaei Fatemeh, Ebrahimi B. NazaninMentari SetiawatiОценок пока нет
- J of Obstet and Gynaecol - 2012 - Aksornphusitaphong - Risk Factors of Early and Late Onset Pre EclampsiaДокумент5 страницJ of Obstet and Gynaecol - 2012 - Aksornphusitaphong - Risk Factors of Early and Late Onset Pre EclampsiaDefi SelvianitaОценок пока нет
- Fetal Macrosomia : Its Maternal and Neonatal ComplicationsДокумент6 страницFetal Macrosomia : Its Maternal and Neonatal ComplicationsTheresia Herestuwito NaruОценок пока нет
- Anemia in Pregnancy : Related Risk Factors in Under Developed AreaДокумент4 страницыAnemia in Pregnancy : Related Risk Factors in Under Developed AreaShalini ShanmugalingamОценок пока нет
- Article 233230Документ11 страницArticle 233230arreyemilieneОценок пока нет
- Pregnancy Outcomes in Women with Renal DiseaseДокумент5 страницPregnancy Outcomes in Women with Renal DiseaselukitaОценок пока нет
- Louis Case Study RH1Документ17 страницLouis Case Study RH1Kuto Yvonne CheronoОценок пока нет
- Karakteristik Preeklampsia Di RSUP Prof. Dr. R. D. Kandou ManadoДокумент5 страницKarakteristik Preeklampsia Di RSUP Prof. Dr. R. D. Kandou ManadoDewanto ChandraОценок пока нет
- Knowledge, Attitudes, and Perceptions of Preeclampsia Among First-Generation Nigerian Women in the United StatesОт EverandKnowledge, Attitudes, and Perceptions of Preeclampsia Among First-Generation Nigerian Women in the United StatesОценок пока нет
- South Africa A Global View of Pulmonary HypertensionДокумент17 страницSouth Africa A Global View of Pulmonary HypertensionDhan RamadhanОценок пока нет
- De Baat 2021Документ7 страницDe Baat 2021Dhan RamadhanОценок пока нет
- Non Carbapenem Therapy For EsblДокумент1 страницаNon Carbapenem Therapy For EsblDhan RamadhanОценок пока нет
- Submission ChecklistДокумент1 страницаSubmission ChecklistDhan RamadhanОценок пока нет
- Please Take This Boarding Pass To The Airport For Your IghtДокумент3 страницыPlease Take This Boarding Pass To The Airport For Your IghtDhan RamadhanОценок пока нет
- KKKДокумент3 страницыKKKDhan RamadhanОценок пока нет
- PT Indo Premier Sekuritas Trade ConfirmationДокумент1 страницаPT Indo Premier Sekuritas Trade ConfirmationDhan RamadhanОценок пока нет
- Riwayat Penyakit KeluargaДокумент3 страницыRiwayat Penyakit KeluargaDhan RamadhanОценок пока нет
- Ethical challenges of fetal diagnosis and treatmentДокумент3 страницыEthical challenges of fetal diagnosis and treatmentDhan RamadhanОценок пока нет
- Untitled 3Документ1 страницаUntitled 3Miguel DinisОценок пока нет
- Common Male Genitourinary ConditionsДокумент3 страницыCommon Male Genitourinary ConditionsDhan RamadhanОценок пока нет
- Profile Keluarga Dampingan Bab 1Документ1 страницаProfile Keluarga Dampingan Bab 1Dhan RamadhanОценок пока нет
- MSCДокумент5 страницMSCDhan RamadhanОценок пока нет
- Hjjffvggtydndndjrbshd NFNDJDJ: FHJGFBHHCFTTRRFHTDCДокумент1 страницаHjjffvggtydndndjrbshd NFNDJDJ: FHJGFBHHCFTTRRFHTDCDhan RamadhanОценок пока нет
- Rational Drug Use in Hepatobiliary Disorders UdayanaДокумент27 страницRational Drug Use in Hepatobiliary Disorders UdayanaDhan RamadhanОценок пока нет
- 10 (2) Management Therapy of Folic Acid and B12 Anemia (VERSI LAMA)Документ44 страницы10 (2) Management Therapy of Folic Acid and B12 Anemia (VERSI LAMA)Muhammad RamadhanОценок пока нет
- Rational Drug Use in Hepatobiliary Disorders UdayanaДокумент27 страницRational Drug Use in Hepatobiliary Disorders UdayanaDhan RamadhanОценок пока нет
- The Partograph: Dr. Rimonta F Gunanegara, SpogДокумент30 страницThe Partograph: Dr. Rimonta F Gunanegara, SpogHans Natanael PosoОценок пока нет
- Case Study PneumothoraxДокумент9 страницCase Study PneumothoraxLee_Cabral_693967% (3)
- ICU Accomplishment Report and Improvement PlanДокумент5 страницICU Accomplishment Report and Improvement PlanMikhaelEarlSantosTacordaОценок пока нет
- Artikel IlmiahДокумент12 страницArtikel IlmiahAsti NurchasanahОценок пока нет
- PWAT (Panographic Wound Assesment Tool) RevisedДокумент4 страницыPWAT (Panographic Wound Assesment Tool) RevisedYunie ArmyatiОценок пока нет
- Position Paper On Teenage PregnancyДокумент3 страницыPosition Paper On Teenage PregnancyMark Anthony CabangonОценок пока нет
- ShineДокумент37 страницShineMohd SaifОценок пока нет
- Safe SexДокумент11 страницSafe SexnathanОценок пока нет
- Ebr 1 (Ob Ii)Документ2 страницыEbr 1 (Ob Ii)Kathleen JosolОценок пока нет
- Vermikompos and Gliocladium Effectiveness Against Fusarium WiltДокумент8 страницVermikompos and Gliocladium Effectiveness Against Fusarium WiltJioWongMenengОценок пока нет
- Leaflet YTiG Plus Tablet For CHCДокумент1 страницаLeaflet YTiG Plus Tablet For CHCDesi Health Tips UpdateОценок пока нет
- Autism Facts vs Myths: Debunking Common MisconceptionsДокумент14 страницAutism Facts vs Myths: Debunking Common Misconceptionsawardeco01Оценок пока нет
- Health Declaration Form For ApplicantsДокумент1 страницаHealth Declaration Form For Applicantsgopeng glamping park malaysiaОценок пока нет
- Htmle Diagnostic Exam RatioДокумент18 страницHtmle Diagnostic Exam RatioAlliah Jessa PascuaОценок пока нет
- Should Medical Marijuana Be Legalized For PatientsДокумент4 страницыShould Medical Marijuana Be Legalized For PatientsBing Cossid Quinones CatzОценок пока нет
- Remote Area Nursing Emergency GuidelinesДокумент325 страницRemote Area Nursing Emergency Guidelineslavinia_dobrescu_1Оценок пока нет
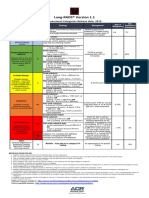
- Lung RADS® Version 1.1: Assessment Categories Release Date: 2019Документ1 страницаLung RADS® Version 1.1: Assessment Categories Release Date: 2019S Francisco MotОценок пока нет
- Corneal Dystrophies: Causes, Symptoms, and TreatmentДокумент2 страницыCorneal Dystrophies: Causes, Symptoms, and TreatmentBadgal BazingaОценок пока нет
- 7-Physiology of Normal PuerperiumДокумент24 страницы7-Physiology of Normal Puerperiumhade elОценок пока нет
- Effect of Temperature On FrogДокумент2 страницыEffect of Temperature On FrogPrerna DubeyОценок пока нет
- Askep CKD Bhs InggrisДокумент15 страницAskep CKD Bhs InggrisFitri MulyaОценок пока нет
- NobelReplace Conical Connect OverviewДокумент6 страницNobelReplace Conical Connect Overviewaziz2007Оценок пока нет
- COVID-19 Patient Report SummaryДокумент2 страницыCOVID-19 Patient Report Summarymuhammad imranОценок пока нет
- Windkessel EffectДокумент11 страницWindkessel EffectAkhmad HidayatОценок пока нет
- Prolonged LaborДокумент13 страницProlonged Laborsujinaranamagar18Оценок пока нет
- NCM101 Health Assessment ExaminationДокумент11 страницNCM101 Health Assessment ExaminationJonah R. Merano100% (1)
- ImmunosuppresentsДокумент13 страницImmunosuppresentsmadeputraОценок пока нет
- 01 PiCCO Brochure ENG 20160428 SДокумент1 страница01 PiCCO Brochure ENG 20160428 SFrancisco QuimbayoОценок пока нет
- Chapter 22: The Thyroid Gland: by Marissa Grotzke, Dev AbrahamДокумент21 страницаChapter 22: The Thyroid Gland: by Marissa Grotzke, Dev AbrahamJanielle FajardoОценок пока нет