Вам также может понравиться
- Complementary and Alternative Medical Lab Testing Part 9: GynecologyОт EverandComplementary and Alternative Medical Lab Testing Part 9: GynecologyОценок пока нет
- Impact of Polycystic Ovary, Metabolic Syndrome and Obesity on Women Health: Volume 8: Frontiers in Gynecological EndocrinologyОт EverandImpact of Polycystic Ovary, Metabolic Syndrome and Obesity on Women Health: Volume 8: Frontiers in Gynecological EndocrinologyОценок пока нет
- Diagnosis of Polycystic Ovarian 9 Syndrome in AdolescenceДокумент17 страницDiagnosis of Polycystic Ovarian 9 Syndrome in AdolescenceTriratna FauziahОценок пока нет
- 6 - Contemporary Management of Polycystic Ovarian Syndrome - 2019Документ11 страниц6 - Contemporary Management of Polycystic Ovarian Syndrome - 2019Johanna Bustos NutricionistaОценок пока нет
- Ijmps - Prevalence of Polycystic Ovarian Syndrome Among PDFДокумент10 страницIjmps - Prevalence of Polycystic Ovarian Syndrome Among PDFAnonymous bqctvu8P3VОценок пока нет
- Epidemiology of Polycystic Ovary Syndrome: A Cross Sectional Study of University Students at An-Najah National University-PalestineДокумент6 страницEpidemiology of Polycystic Ovary Syndrome: A Cross Sectional Study of University Students at An-Najah National University-PalestineOckta KaruniaОценок пока нет
- Fenotipo PCOДокумент7 страницFenotipo PCONatalyОценок пока нет
- EscobarДокумент6 страницEscobarFernando Silva RivasОценок пока нет
- Acog 194Документ15 страницAcog 194Marco DiestraОценок пока нет
- AACE/ACE Disease State Clinical ReviewДокумент10 страницAACE/ACE Disease State Clinical ReviewSanjay NavaleОценок пока нет
- Diagnóstico Del SopДокумент13 страницDiagnóstico Del SopxcarlosfxОценок пока нет
- Association of Clinical Features With Obesity and Gonadotropin Levels in Women With Polycystic Ovarian SyndromeДокумент4 страницыAssociation of Clinical Features With Obesity and Gonadotropin Levels in Women With Polycystic Ovarian Syndromedoctor wajihaОценок пока нет
- Epidemiology, Phenotype, and Genetics of The Polycystic Ovary Syndrome in AdultsДокумент23 страницыEpidemiology, Phenotype, and Genetics of The Polycystic Ovary Syndrome in AdultsApotik ApotekОценок пока нет
- PCOS ProposalДокумент8 страницPCOS ProposalZain AkramОценок пока нет
- Systematic Review On Recognising Patterns in Incidence of Polycystic Ovarian Syndrome in Young WomenДокумент4 страницыSystematic Review On Recognising Patterns in Incidence of Polycystic Ovarian Syndrome in Young WomenInternational Journal of Innovative Science and Research TechnologyОценок пока нет
- GWAS PCOS KoreaДокумент9 страницGWAS PCOS KoreaedwardОценок пока нет
- Adolescent Gynecologic Care QUESTIONS 1, 2, 3Документ7 страницAdolescent Gynecologic Care QUESTIONS 1, 2, 3patelkn_2005Оценок пока нет
- Polikistik Pada RemajaДокумент9 страницPolikistik Pada Remajakinanti wulanОценок пока нет
- 3.review of Literature PDFДокумент38 страниц3.review of Literature PDFJalajarani AridassОценок пока нет
- PcosДокумент17 страницPcosshrabon001Оценок пока нет
- Health-Related Quality of Life in Adult MediterranДокумент21 страницаHealth-Related Quality of Life in Adult MediterrancxksvhszsvОценок пока нет
- PCOS Guidelines 1Документ14 страницPCOS Guidelines 1Angelie Therese ChuaОценок пока нет
- Original Study Differences in The Management of Adolescents With Polycystic Ovary Syndrome Across Pediatric SpecialtiesДокумент5 страницOriginal Study Differences in The Management of Adolescents With Polycystic Ovary Syndrome Across Pediatric SpecialtiesfujimeisterОценок пока нет
- Determining The Insulin Resistance Rate in Polycystic Ovary Syndrome Patients (Pcos)Документ9 страницDetermining The Insulin Resistance Rate in Polycystic Ovary Syndrome Patients (Pcos)ijasrjournalОценок пока нет
- Determining The Insulin Resistance Rate in Polycystic Ovary Syndrome Patients (Pcos)Документ9 страницDetermining The Insulin Resistance Rate in Polycystic Ovary Syndrome Patients (Pcos)ijasrjournalОценок пока нет
- Diagnostic Evaluation of Polycystic Ovary Syndrome in Adolescents - UpToDateДокумент31 страницаDiagnostic Evaluation of Polycystic Ovary Syndrome in Adolescents - UpToDateRICO NOVYANTOОценок пока нет
- Polycystic Ovarian SyndromeДокумент19 страницPolycystic Ovarian SyndromeAndreeaBiancaPuiuОценок пока нет
- Sign of Hyperandrogenism PDFДокумент6 страницSign of Hyperandrogenism PDFmisbah_mdОценок пока нет
- V Polycystic Ovarysyndrome: EpidemiologyДокумент13 страницV Polycystic Ovarysyndrome: Epidemiologyrolla_hiraОценок пока нет
- Polycystic Ovary Syndrome 2016 NEJMДокумент11 страницPolycystic Ovary Syndrome 2016 NEJMGabrielaОценок пока нет
- JurnalДокумент6 страницJurnalWidya Rachmania PutriОценок пока нет
- The Pubertal Presentation of Polycystic Ovary Syndrome PCOS 2002 Fertility and SterilityДокумент1 страницаThe Pubertal Presentation of Polycystic Ovary Syndrome PCOS 2002 Fertility and SterilityfujimeisterОценок пока нет
- Assessment of Thyroid and Prolactin Levels Among The Women With Abnormal Uterine BleedingДокумент6 страницAssessment of Thyroid and Prolactin Levels Among The Women With Abnormal Uterine BleedingMezouar AbdennacerОценок пока нет
- Seminar: Robert J Norman, Didier Dewailly, Richard S Legro, Theresa E HickeyДокумент13 страницSeminar: Robert J Norman, Didier Dewailly, Richard S Legro, Theresa E HickeyMédica Consulta ExternaОценок пока нет
- 10.1007@s00404 018 4680 1Документ12 страниц10.1007@s00404 018 4680 1Eva OretlaОценок пока нет
- LECTURE 24 Polycystic Ovary SyndromeДокумент13 страницLECTURE 24 Polycystic Ovary SyndromeCharisse Angelica MacedaОценок пока нет
- Ovario Poliquístico/Polycystic Ovary SyndromeДокумент14 страницOvario Poliquístico/Polycystic Ovary SyndromeJosé María Lauricella100% (1)
- 1 s2.0 S0026049517302743 MainДокумент11 страниц1 s2.0 S0026049517302743 MainTeodora OnofreiОценок пока нет
- Polycystic Ovary SyndromeДокумент13 страницPolycystic Ovary SyndromeNAYSHA YANET CHAVEZ RONDINELОценок пока нет
- Polycystic Ovary SyndromeДокумент13 страницPolycystic Ovary SyndromeLIZARDO CRUZADO DIAZОценок пока нет
- ImprovedДокумент8 страницImprovedCecilia CabanagОценок пока нет
- MetforminДокумент14 страницMetforminnidyaОценок пока нет
- RMB2 16 67 PDFДокумент5 страницRMB2 16 67 PDFMariam QaisОценок пока нет
- Renal Resistive Index in Patients With Polycystic Ovary SyndromeДокумент5 страницRenal Resistive Index in Patients With Polycystic Ovary Syndromemeltwithsnow163.comОценок пока нет
- New in JPNДокумент7 страницNew in JPNHar YudhaОценок пока нет
- Ijem 23 326Документ6 страницIjem 23 326calvinjohn1690Оценок пока нет
- Jhpn0033-0157 Nilai RДокумент11 страницJhpn0033-0157 Nilai RDavid Eka PrasetyaОценок пока нет
- The Prevalence of Thyroid Dysfunction and HyperproДокумент8 страницThe Prevalence of Thyroid Dysfunction and HyperproHannaОценок пока нет
- Laparoscopic ClomipenДокумент5 страницLaparoscopic ClomipenHar YudhaОценок пока нет
- 12 PDFДокумент6 страниц12 PDFsilvanaОценок пока нет
- Polycystic Ovary Syndrome in Adolescents: Alvina R. Kansra, MDДокумент7 страницPolycystic Ovary Syndrome in Adolescents: Alvina R. Kansra, MDHaviz YuadОценок пока нет
- 9 - Hyperandrogenemia and Insulin Resistance - The Chief Culprit of Polycystic Ovary Syndrome - 2019Документ32 страницы9 - Hyperandrogenemia and Insulin Resistance - The Chief Culprit of Polycystic Ovary Syndrome - 2019Johanna Bustos NutricionistaОценок пока нет
- The Prevalence of Polycystic Ovary Syndrome in A Community Sample Assessed Under Contrasting Diagnostic CriteriaДокумент8 страницThe Prevalence of Polycystic Ovary Syndrome in A Community Sample Assessed Under Contrasting Diagnostic CriteriaKe XuОценок пока нет
- Polycystic Ovary SyndromeДокумент11 страницPolycystic Ovary SyndromeViridiana Briseño GarcíaОценок пока нет
- NP020110 P18table1Документ1 страницаNP020110 P18table1Celine SuryaОценок пока нет
- Jpe 3 E05Документ6 страницJpe 3 E05amirreza jmОценок пока нет
- Jurnal 1Документ8 страницJurnal 1lomba Panah Dies UnsriОценок пока нет
- ReviewДокумент13 страницReviewNelly ElizabethОценок пока нет
- Chang 2020Документ13 страницChang 2020Fernando Silva RivasОценок пока нет
- Nonfar PcosДокумент13 страницNonfar PcosyuniОценок пока нет
- Cord Blood Revelations The Importance of Being A First Born Girl Big On Time and To A Young Mother 2007 Early Human DevelopmentДокумент9 страницCord Blood Revelations The Importance of Being A First Born Girl Big On Time and To A Young Mother 2007 Early Human DevelopmentfujimeisterОценок пока нет
- Effect of Preeclampsia On Umbilical Cord Blood Hematopoietic Progenitor Stem Cells 2001 American Journal of Obstetrics and GynecologyДокумент5 страницEffect of Preeclampsia On Umbilical Cord Blood Hematopoietic Progenitor Stem Cells 2001 American Journal of Obstetrics and GynecologyfujimeisterОценок пока нет
- In Vitro Transdifferentiation of Umbilical Cord Stem Cells Into Cardiac Myocytes: Role of Growth FactorsДокумент8 страницIn Vitro Transdifferentiation of Umbilical Cord Stem Cells Into Cardiac Myocytes: Role of Growth FactorsfujimeisterОценок пока нет
- Expression of Epithelial Markers by Human Umbilical Cord Stem Cells A Topographical Analysis 2014 PlacentaДокумент7 страницExpression of Epithelial Markers by Human Umbilical Cord Stem Cells A Topographical Analysis 2014 PlacentafujimeisterОценок пока нет
- Placenta: J.L. James, S. Srinivasan, M. Alexander, L.W. ChamleyДокумент8 страницPlacenta: J.L. James, S. Srinivasan, M. Alexander, L.W. ChamleyfujimeisterОценок пока нет
- European Journal of Obstetrics & Gynecology and Reproductive BiologyДокумент7 страницEuropean Journal of Obstetrics & Gynecology and Reproductive BiologyfujimeisterОценок пока нет
- Cell Salvage in Obstetrics 2008 International Journal of Obstetric AnesthesiaДокумент9 страницCell Salvage in Obstetrics 2008 International Journal of Obstetric AnesthesiafujimeisterОценок пока нет
- Poster Session VДокумент1 страницаPoster Session VfujimeisterОценок пока нет
- Birth Weight As A Risk Factor For Cancer in Adulthood The Stem Cell Perspective 2011 MaturitasДокумент3 страницыBirth Weight As A Risk Factor For Cancer in Adulthood The Stem Cell Perspective 2011 MaturitasfujimeisterОценок пока нет
- Stem Cells in Gynecology 2012 American Journal of Obstetrics and GynecologyДокумент8 страницStem Cells in Gynecology 2012 American Journal of Obstetrics and GynecologyfujimeisterОценок пока нет
- Banking Obstetric Related Tissues and Cells What Every Maternity Unit Must Know 2008 Obstetrics Gynaecology Reproductive MedicineДокумент4 страницыBanking Obstetric Related Tissues and Cells What Every Maternity Unit Must Know 2008 Obstetrics Gynaecology Reproductive MedicinefujimeisterОценок пока нет
- Social Science & Medicine: Julie KentДокумент10 страницSocial Science & Medicine: Julie KentfujimeisterОценок пока нет
- Review Endothelial Progenitor Cells in Pregnancy and Obstetric Pathologies 2013 PlacentaДокумент6 страницReview Endothelial Progenitor Cells in Pregnancy and Obstetric Pathologies 2013 PlacentafujimeisterОценок пока нет
- Factors Predicting The Hematopoietic Stem Cells Content of The Umbilical Cord Blood 2013 Transfusion and Apheresis ScienceДокумент6 страницFactors Predicting The Hematopoietic Stem Cells Content of The Umbilical Cord Blood 2013 Transfusion and Apheresis SciencefujimeisterОценок пока нет
- Optimizing Umbilical Cord Blood Collection Impact of ObstetricДокумент3 страницыOptimizing Umbilical Cord Blood Collection Impact of ObstetricGhada AlОценок пока нет
- What Is The Risk of Metabolic Syndrome in Adolescents With Normal BMI Who Have Polycystic Ovary Syndrome 2015 Journal of Pediatric and Adolescent GynДокумент4 страницыWhat Is The Risk of Metabolic Syndrome in Adolescents With Normal BMI Who Have Polycystic Ovary Syndrome 2015 Journal of Pediatric and Adolescent GynfujimeisterОценок пока нет
- Impact of Reduced Intensity Conditioning Allogeneic Stem Cell Transplantation On Women S Fertility 2013 Clinical Lymphoma Myeloma and LeukemiaДокумент7 страницImpact of Reduced Intensity Conditioning Allogeneic Stem Cell Transplantation On Women S Fertility 2013 Clinical Lymphoma Myeloma and LeukemiafujimeisterОценок пока нет
- Utility of Ultrasound in The Diagnosis of Polycystic Ovary Syndrome in Adolescents 2014 Fertility and SterilityДокумент7 страницUtility of Ultrasound in The Diagnosis of Polycystic Ovary Syndrome in Adolescents 2014 Fertility and SterilityfujimeisterОценок пока нет
- Giving To Receive The Right To Donate in Umbilical Cord Blood Banking For Stem Cell Therapies 2012 Health PolicyДокумент8 страницGiving To Receive The Right To Donate in Umbilical Cord Blood Banking For Stem Cell Therapies 2012 Health PolicyfujimeisterОценок пока нет
- Endometriosis - Pathogenesis, Clinical Features, and Diagnosis - UpToDateДокумент39 страницEndometriosis - Pathogenesis, Clinical Features, and Diagnosis - UpToDatefujimeisterОценок пока нет
- Obstetric Predictors of Placental Umbilical Cord Blood Volume For Transplantation 2003 American Journal of Obstetrics and GynecologyДокумент7 страницObstetric Predictors of Placental Umbilical Cord Blood Volume For Transplantation 2003 American Journal of Obstetrics and GynecologyfujimeisterОценок пока нет
- Utility of The Oral Glucose Tolerance Test To Assess Glucose Abnormalities in Adolescents With Polycystic Ovary Syndrome 2016 Journal of Pediatric andДокумент5 страницUtility of The Oral Glucose Tolerance Test To Assess Glucose Abnormalities in Adolescents With Polycystic Ovary Syndrome 2016 Journal of Pediatric andfujimeisterОценок пока нет
- Polycystic Ovary Syndrome An Under Recognized Cause of Abnormal Uterine Bleeding in Adolescents Admitted To A Children S Hospital 2016 Journal of PediДокумент7 страницPolycystic Ovary Syndrome An Under Recognized Cause of Abnormal Uterine Bleeding in Adolescents Admitted To A Children S Hospital 2016 Journal of PedifujimeisterОценок пока нет
- Polycystic Ovary Syndrome A Review For Dermatologists Part I Diagnosis and Manifestations 2014 Journal of The American Academy of DermatologyДокумент10 страницPolycystic Ovary Syndrome A Review For Dermatologists Part I Diagnosis and Manifestations 2014 Journal of The American Academy of DermatologyfujimeisterОценок пока нет
- Treatment of PCOS in Adolescence 2006 Best Practice Research Clinical Endocrinology MetabolismДокумент20 страницTreatment of PCOS in Adolescence 2006 Best Practice Research Clinical Endocrinology MetabolismfujimeisterОценок пока нет
- Vitamin D Deficiency Among Adolescent Females With Polycystic Ovary Syndrome 2015 Journal of Pediatric and Adolescent GynecologyДокумент4 страницыVitamin D Deficiency Among Adolescent Females With Polycystic Ovary Syndrome 2015 Journal of Pediatric and Adolescent GynecologyfujimeisterОценок пока нет
- Conclusions: Background:: Oral Abstracts / J Pediatr Adolesc Gynecol (2013) E47ee53 E49Документ2 страницыConclusions: Background:: Oral Abstracts / J Pediatr Adolesc Gynecol (2013) E47ee53 E49fujimeisterОценок пока нет
- Using The Androgen Excess PCOS Society Criteria To Diagnose Polycystic Ovary Syndrome and The Risk of Metabolic Syndrome in Adolescents 2013 The JournДокумент5 страницUsing The Androgen Excess PCOS Society Criteria To Diagnose Polycystic Ovary Syndrome and The Risk of Metabolic Syndrome in Adolescents 2013 The JournfujimeisterОценок пока нет
- The Utility of Ultrasonography in The Diagnosis of Polycystic Ovarian Syndrome PCOS in Adolescents 2014 Journal of Pediatric and Adolescent GynecologyДокумент1 страницаThe Utility of Ultrasonography in The Diagnosis of Polycystic Ovarian Syndrome PCOS in Adolescents 2014 Journal of Pediatric and Adolescent GynecologyfujimeisterОценок пока нет
- Advances in Reproductive EndocrinologyДокумент41 страницаAdvances in Reproductive Endocrinologyapi-3705046Оценок пока нет
- NDE AndrogenДокумент3 страницыNDE AndrogenRupert BautistaОценок пока нет
- Complete Steroid Handbook 2004 EditionДокумент82 страницыComplete Steroid Handbook 2004 Editionmathiouem100% (12)
- Sciences2lp ModakiratДокумент29 страницSciences2lp Modakiratapi-24974205850% (4)
- 10 Best CycleДокумент6 страниц10 Best CycleKaizer DaveОценок пока нет
- UT Progestin PDFДокумент10 страницUT Progestin PDFLidyaОценок пока нет
- Graphing Hormones LabДокумент4 страницыGraphing Hormones LabSarahlynn CampbellОценок пока нет
- Unit 3 Module 1 The Menstrual CycleДокумент20 страницUnit 3 Module 1 The Menstrual CycleMARIANNE SORIANO100% (2)
- Ambiguous Genitalia 5Документ6 страницAmbiguous Genitalia 5Claudetteanne6171Оценок пока нет
- Menstrual Cycle Test 1 1Документ8 страницMenstrual Cycle Test 1 1KvmLly100% (1)
- Sign of Hyperandrogenism PDFДокумент6 страницSign of Hyperandrogenism PDFmisbah_mdОценок пока нет
- PcosДокумент25 страницPcosing_claudia100% (3)
- CDGP Versus HypogonadismДокумент25 страницCDGP Versus HypogonadismmpintobОценок пока нет
- Testicular Growth and Development in PubertyДокумент10 страницTesticular Growth and Development in PubertyRaul DoctoОценок пока нет
- Menstrual Cycle Fuck UДокумент12 страницMenstrual Cycle Fuck UChong ChengОценок пока нет
- Barbell 55 Nutrition Plan by Guru MannДокумент2 страницыBarbell 55 Nutrition Plan by Guru MannVikas TomarОценок пока нет
- Ambiguousgenetalia 2017Документ13 страницAmbiguousgenetalia 2017willyОценок пока нет
- Developmental Aspects of The Reproductive SystemДокумент4 страницыDevelopmental Aspects of The Reproductive SystemDiana MartínezОценок пока нет
- Norge StrelДокумент7 страницNorge StrelPapaindoОценок пока нет
- Dr. Sachin Kapur M.Phil, PHD: 20+ Years Teaching ExperienceДокумент40 страницDr. Sachin Kapur M.Phil, PHD: 20+ Years Teaching ExperienceDivyansh VermaОценок пока нет
- Male and Female Sex HormonesДокумент20 страницMale and Female Sex HormonesJose Fernando Gregana ElpaОценок пока нет
- RFI Strip Chart 333 To 379Документ90 страницRFI Strip Chart 333 To 379mad21_Оценок пока нет
- Degarelix (SQ) : Flutamide, BicalutamideДокумент5 страницDegarelix (SQ) : Flutamide, BicalutamideGregОценок пока нет
- Anabolic Androgenic Steroids Muscle and Man 513877Документ4 страницыAnabolic Androgenic Steroids Muscle and Man 513877Wagen WerksОценок пока нет
- Anabolic Steroid ProfilesДокумент135 страницAnabolic Steroid ProfilesX-ON FITNESS100% (2)
- Anabolic Steroids PowerpointДокумент20 страницAnabolic Steroids Powerpointapi-252997462Оценок пока нет
- SteroidДокумент14 страницSteroidChifor Constantin25% (4)
- Q2 W1 Day 1 - 5 ScienceДокумент10 страницQ2 W1 Day 1 - 5 ScienceCastle Gelyn100% (1)
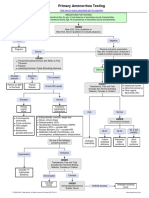
- Primary Amenorrhea Testing AlgorithmДокумент1 страницаPrimary Amenorrhea Testing AlgorithmfarmasiОценок пока нет
- Hormone/Contraceptive Use in O&G: Provera Acute Maintena NceДокумент2 страницыHormone/Contraceptive Use in O&G: Provera Acute Maintena Ncekhangsiean89Оценок пока нет