Академический Документы
Профессиональный Документы
Культура Документы
Metabolic Syndrome A Sympathetic Disease Schlaich2015
Загружено:
monteОригинальное название
Авторское право
Доступные форматы
Поделиться этим документом
Поделиться или встроить документ
Этот документ был вам полезен?
Это неприемлемый материал?
Пожаловаться на этот документАвторское право:
Доступные форматы
Metabolic Syndrome A Sympathetic Disease Schlaich2015
Загружено:
monteАвторское право:
Доступные форматы
Personal View
Metabolic syndrome: a sympathetic disease?
Markus Schlaich, Nora Straznicky, Elisabeth Lambert, Gavin Lambert
Metabolic syndrome is associated with adverse health outcomes and is a growing problem worldwide. Although Lancet Diabetes Endocrinol 2014
eorts to harmonise the denition of metabolic syndrome have helped to better understand the prevalence and the Published Online
adverse outcomes associated with the disorder on a global scale, the mechanisms underpinning the metabolic April 2, 2014
http://dx.doi.org/10.1016/
changes that dene it are incompletely understood. Accumulating evidence from laboratory and human studies S2213-8587(14)70033-6
suggests that activation of the sympathetic nervous system has an important role in metabolic syndrome. Indeed,
See Online/Comment
treatment strategies commonly recommended for patients with metabolic syndrome, such as diet and exercise to http://dx.doi.org/10.1016/
induce weight loss, are associated with sympathetic inhibition. Pharmacological and device-based approaches to S2213-8587(14)70072-5
target activation of the sympathetic nervous system directly are available and have provided evidence to support the Neurovascular Hypertension
important part played by sympathetic regulation, particularly for blood pressure and glucose control. Preliminary and Kidney Disease and Human
Neurotransmitters
evidence is encouraging, but whether therapeutically targeting sympathetic overactivity could help to prevent
Laboratories, Baker IDI Heart
metabolic syndrome and attenuate its adverse outcomes remains to be determined. and Diabetes Institute,
Melbourne, VIC, Australia
Introduction Sympathetic nervous activation in metabolic (Prof M Schlaich MD,
N Straznicky PhD, E Lambert PhD,
The large rise in incidence of obesity in both developed syndrome and obesity Prof G Lambert PhD);
and developing countries has led to a burgeoning in the Investigators have reported clear evidence that obesity and Department of Cardiovascular
incidence of risk factors associated with the development its metabolic eects are associated with a chronic Medicine, Alfred Hospital,
of cardiovascular disease and type 2 diabetes. Collectively activation of sympathetic nervous tone. Sympatho- Melbourne, VIC, Australia
(Prof M Schlaich); and Faculty of
termed metabolic syndrome, these risk factors can excitationas indicated by increases in urinary
Medicine, Nursing and Health
include a combination of abdominal obesity, increased noradrenaline and metabolite concentrations, eerent Sciences, Monash University,
triglyceride concentrations, reduced HDL cholesterol muscle sympathetic nerve activity, and increased rates of Melbourne, VIC, Australia
concentrations, high blood pressure, and hyperglycaemia spillover of noradrenaline to plasma, particularly in people (Prof M Schlaich, E Lambert,
Prof G Lambert)
(panel). Although various societies and interest groups with concomitant insulin resistancehas been recorded
Correspondence to:
initially provided their own criteria for the denition of in obese individuals. Additionally, sympathetic nervous
Prof Markus Schlaich,
metabolic syndrome (appendix),1 in 2009, an international responses to several physiologically relevant stimuli, such Neurovascular Hypertension and
task force proposed a single set of cuto points for all as changing energy states, food intake, glucose Kidney Disease Laboratory, Baker
components except waist circumference (for which they consumption, hyperinsulinaemia, and exposure to cold, IDI Heart and Diabetes Institute,
Melbourne, VIC 8008, Australia
recommended population and country specic are blunted in obese people.4 Blunted sympathetic
markus.schlaich@bakeridi.
denitions; appendix) to harmonise the denition of the responses could contribute to decient thermogenesis, edu.au
syndrome (panel).2 positive energy balance, and increased weight gain. By
A sedentary lifestyle, unfavourable diet, and genetic contrast, exaggerated responses to mental stress and See Online for appendix
predisposition are important factors that underlie increased resting sympathetic activity could predispose an
metabolic syndrome, but emerging evidence also individual to the development of insulin resistance,
indicates the importance of the sympathetic nervous hypertension, renal disease, and cardiac abnormalities
system in the development and progression of obesity- such as diastolic dysfunction and left ventricular
related illnesses. The sympathetic nervous system is hypertrophy.5
well recognised as being important for cardiovascular The exact mechanisms that link obesity and activation
control, but activation of the sympathetic nervous system of the sympathetic nervous system remain to be
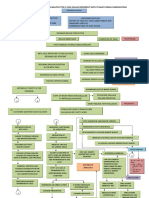
also has substantial metabolic eects (gure 1). For
example, direct stimulation of the hepatic sympathetic
nerves3 induces a rapid and marked release of glucose Panel: Criteria for metabolic syndrome2
from the liver, whereas the stimulation of nerves that Increased waist circumference (population and
supply the pancreas is associated with reduced insulin country specic denitions; see appendix)
and increased glucagon concentrations in portal blood. Triglyceride concentration 150 mg/dL (17 mmol/L), or
Furthermore, activation of sympathetic bres that patient undergoing drug treatment for high triglycerides
innervate adipose tissue results in lipolysis and neurally HDL cholesterol concentrations of <40 mg/dL (10 mmol/L)
mediated vasoconstriction of the peripheral arterioles, in men, <50 mg/dL (13 mmol/L) in women, or patient
which is associated with impaired glucose uptake in undergoing drug treatment for low HDL cholesterol
skeletal muscle. These metabolic and sympathetically Systolic blood pressure 130 mm Hg, diastolic 85 mm Hg,
mediated eects are important in stressful situations of or both; or patient with a history of hypertensioan
short duration to cope with increased energy undergoing antihypertensive treatment
requirements; however, sustained sympathetic activation Fasting plasma glucose concentrations of 100 mg/dL, or
can result in adverse metabolic and cardiovascular patient undergoing drug treatment for high glucose
outcomes.
www.thelancet.com/neurology Published online April 2, 2014 http://dx.doi.org/10.1016/S2213-8587(14)70033-6 1
Personal View
determined. Dierent investigators69 have proposed Mechanisms of sympathetic nervous activation
several theories to link overeating, obesity, insulin Hyperinsulinaemia
resistance, adipokines, non-esteried free fatty acid Insulin acts to reduce hepatic production of glucose
(NEFAs), and changes in -adrenergic responsiveness through direct eects on the liver to reduce glycogenolysis
with sympathetic activation, with their views diering and through indirect eects, including inhibition of
about whether sympathetic activation is a cause or a lipolysis, reduction in glucagon, and modication of
result of metabolic alterations (gure 2). Each theory has hypothalamic signalling. Selective reduction of insulin
merit, but in this Personal View, our main aim is to focus receptors in the medial area of the arcuate nucleus in
on the role of the sympathetic nervous activation in the animals is associated with hyperphagia, increased fat
pathology associated with obesity in metabolic syndrome. mass, and the rapid development of hepatic insulin
In their prospective study with a 10 year follow-up, resistance.13 Furthermore, stimulation of hypothalamic
Masuo and colleagues10,11 noted that increased circulating insulin signalling results in about a 40% inhibition of
noradrenaline at baseline predicted future weight gain glucose production. The central eect of insulin is
and increases in insulin concentrations and blood probably mediated, at least partly, by inhibition of
pressure, supporting a role of the sympathetic nervous neuropeptide Y neurones in the arcuate nucleus of the
system in the generation of obesity and metabolic hypothalamus. Intra-cerebroventricular infusion of
syndrome. Researchers have reported similar ndings neuropeptide Y in mice leads to the development of
that link plasma noradrenaline concentration at baseline insulin resistance to endogenous glucose production
and increased weight gain12 after an approximate through the activation of sympathetic drive to the liver.13
20 year follow-up. Although an undoubtedly important link exists
between insulin and sympathetic regulation, results of
Sympathetic nervous system studies in human beings indicate that the sympathetic
nervous response elicited by insulin is heterogeneous.
For example, muscle sympathetic nerve activity increases
in response to acute hyperinsulinaemia and this response
is blunted in obese people, whereas renal noradrenaline
spillover does not change.4 Consistent with no eect on
renal sympathetic outow, we have noted no association
between hyperinsulinaemia and the rate of renal
noradrenaline spillover to plasma in obese people.4 Given
that obesity and hypertension are accompanied by high
rates of noradrenaline spillover from the kidneys, the
mechanisms that underpin the increased sympathetic
outow in obesity in metabolic syndrome might not be
Adipocytes Liver Pancreatic Skeletal Skeletal muscle conned to hyperinsulinaemia.5,13 Indeed, Gentile and
cells muscle arteriole colleagues14 examined the eect of weight gain in lean
Lipolysis Gluconeogenesis Insulin release Impaired glucose Vasoconstriction; people and noted that even a slight increase in weight in
uptake rarefection
obese individuals was associated with increased
Figure 1: Overview of the eect of an activated sympathetic nervous system on pathways that adversely sympathetic nervous activity with no change in insulin
aect metabolic control concentration. Similarly, we have noted an association
between discrete increases in abdominal fat mass and
Landsberg and colleagues Reaven Grundy Julius and colleagues increased muscle sympathetic activity in people with
Overeating Insulin resistance Increased visceral fat Sympathetic activation
metabolic syndrome during a period of overall weight
stabilisation.15
Obesity Hyperinsulinaemia Increased adipokines and Reduced muscle blood Increased adiposity and hyperleptinaemia
non-esteried fatty acids ow and glucose uptake
Body fat, particularly abdominal visceral fat,16 is a major
Insulin resistance
determinant of muscle sympathetic nerve activity.
Products of visceral fat such as NEFAs and leptin might
Sympathetic activation Insulin resistance Insulin resistance contribute to sympathetic activation and to the
Hyperinsulinaemia development of insulin resistance in people with
abdominal obesity. Antigens derived from perivascular
Sympathetic activation Hypertension Sympathetic activation Obesity
fat surrounding the aorta might promote the inltration
of leucocytes into the aorta, kidney, and central nervous
system, and lead to sympathetic activation and
Figure 2: Various theories postulated to link elements of metabolic syndrome and changes in -adrenergic
responsiveness with sympathetic activation hypertension development.17,18 High plasma NEFA
Concepts based on Lansberg and colleagues,6 Reaven,7 Grundy,8 and Julius and colleagues.9 concentrations have been associated with worsening
2 www.thelancet.com/neurology Published online April 2, 2014 http://dx.doi.org/10.1016/S2213-8587(14)70033-6
Personal View
glucose tolerance.19 Studies in human beings have shown high blood pressure, hyperinsulinaemia, increased
a positive association between high blood pressure and plasma triglyceride concentrations, and decreased HDL
plasma concentrations of NEFAs,20 and investigators cholesterol concentrations.34 Although muscle sympathetic
note that acute increases in NEFA concentrations result nerve activity is higher in people with metabolic syndrome
in an increase in 1-adrenoceptor-mediated pressor with obstructive sleep apnoea than in those without,35
sensitivity,21 a rise in blood pressure, and increased sympathetic activity is also increased in lean people with
muscle sympathetic activity.22 Although these studies obstructive sleep apnoea (gure 3).36 Trombetta and
support the notion of an interaction between NEFAs and colleagues reported that the increase in sympathetic
the sympathetic nervous system, Grekin and colleagues23 activity in metabolic syndrome is at least partly due to
noted that whole-body and renal noradrenaline spillover increased chemoreex sensitivity.35 Interestingly, con-
tended to be reduced during fatty acid infusion, despite a tinuous positive airway pressure reduced sympathetic
substantial increase in circulating NEFAs. drive in obese patients with obstructive sleep apnoea,37
Researchers have noted a marked rise in muscle and it improved insulin sensitivity, blood pressure, and
sympathetic activity when healthy lean men are given the lipid prole in patients with both obstructive sleep
leptin.24 Although our own investigations have provided apnoea and metabolic syndrome.38 The improvement in
some support for interactions between leptin and insulin sensitivity was greater in lean people than in obese
activation of the renal sympathetic nervous system in individuals, suggesting that insulin sensitivity is more
obese individuals,25 whether leptin elicits changes in related to the degree of obesity rather than to obstructive
brain signalling and acts as a major driver of sympathetic sleep apnoea.38
activation in patients with metabolic syndrome is not
known. However, casting doubt over the importance of Results of sympathetic nervous activation in
leptin, researchers reported that leptin gene expression obesity in metabolic syndrome
was higher in subcutaneous than in visceral adipose Hypertension
tissue26 yet sympathetic activity in muscle was not Risk estimations ascribe 6575% of the risk for primary
increased in people with subcutaneous obesity, even hypertension to overweight and obesity, but the
though their plasma leptin concentrations were between mechanisms that link obesity and high blood pressure
two to three times higher.27 Additionally, results of remain incompletely understood.39 Activation of the
longitudinal studies show that rises in plasma sympathetic nervous system, particularly when directed
noradrenaline concentrations preceded weight gain and towards the kidneys as is commonly evident in obesity,
increases in blood pressure and plasma leptin results in increased renal tubular sodium reabsorption,
concentration.10,11
*
Hypothalamic-pituitary-adrenal axis activation 80 *
Glucocorticoid concentrations can increase in response *
to chronic stress and have been linked with the onset of
metabolic disturbances, including hyperinsulinaemia,
70
insulin resistance, glucose intolerance, hyperlipidaemia, *
increased visceral fat mass,28 and the development of *
hypertension.29 Activation of the hypothalamic-pituitary-
Bursts per 100 heartbeats
adrenal axis in response to a stressful life event such as 60
family bereavement or job change can lead to a rapid and
pronounced increase in weight gain in premenopausal
women.30 Men with high stress and hostility scores are
50
more likely to have insulin resistance than are those with
very low scores.31 In the Whitehall II study, work-related
stress was related to risk of development of general and
central obesity32 and to about a two-times increase in risk 40
of development of type 2 diabetes in middle-aged
(3555 years) women.33 Increased 24 h urinary cortisol
and normetanephrine concentrations were noted in 30
individuals with metabolic syndrome, with behavioural Lean Lean with Obese Obese with
obstructive sleep obstructive sleep
factors accounting for about 40% of the link between apnoea apnoea
sympathetic activation and metabolic syndrome. Patient groups
Figure 3: Muscle sympathetic nerve activity in lean and obese patients with
Obstructive sleep apnoea
and without obstructive sleep apnoea
Obstructive sleep apnoea is common in obese individuals *p<001. Figure reproduced from reference 36, with permission of Wolters
and is independently associated with insulin resistance, Kluwer Health.
www.thelancet.com/neurology Published online April 2, 2014 http://dx.doi.org/10.1016/S2213-8587(14)70033-6 3
Personal View
changes in renal blood ow, and release of renin, concentrations.3 Data from studies in dogs indicate that
engaging the renin-angiotensin-aldosterone system. In the hepatic sympathetic nerves inhibit liver glucose
combination with obesity-induced physical compression uptake and that hepatic sympathetic denervation leads to
of the kidneys, which is likely to further aggravate an increase in net hepatic glucose uptake in response to
sympathetic stimulation, a blood pressure increase in hyperglycaemia.52 Impaired glucose tolerance and insulin
obese individuals is an obvious result.40 In obese resistance are commonly noted in patients with liver
adolescents, high blood pressure is associated with cirrhosis.53 After liver transplantation, glucose tolerance
increased urinary catecholamine concentrations and an and insulin sensitivity are markedly improved, largely
unfavourable metabolic prole.41 Pharmacologically through improvements in hepatic glucose clearance and
blocking the autonomic system in obese individuals peripheral glucose disposal.54 These results indicate that
shows that sympathetic nervous activation has an therapeutically targeting the hepatic sympathetic outow
important role in increasing blood pressure in obesity.42 could provide clinical benet to patients with prediabetes
In patients with morning hypertension, 1-adrenergic or type 2 diabetes.
blockade with doxazosin before sleep improved both
morning blood pressure and insulin resistance.43 Obesity- Organ damage
related hypertension is characterised by activation of the In addition to metabolic eects, chronic activation of the
sympathetic nervous outows to the kidneys and skeletal sympathetic nervous system favours the development
muscle vasculature,13 with recruitment of previously and progression of target organ damage. Of particular
silent bres the salient feature that characterises the importance is damage to the kidney, heart, and
pattern of sympathetic activation.44 Importantly, although vasculature.
this pattern of sympathetic activation could underpin the Regional sympathetic activation, with evidence for
pathophysiology of hypertension in obesity, activation of increased sympathetic nervous outow to the kidneys,
the sympathetic nervous system is also evident in obese occurs in obese individuals and in patients with
normotensive people.44 hypertension.4 Obesity is independently associated with
the development of end-stage renal disease.55 Overweight
Insulin resistance (BMI >25 kg/m) at age 20 years has been linked to about
The physiological association between insulin and a three times increased risk of development of chronic
sympathetic nervous activation is complex. Increased renal failure later in life.56 Moreover, the presence of
circulating insulin might drive a regional increase in obesity poses a large risk for progressive renal
sympathetic activity, but, given that sympathetically impairment in patients with established renal disease.57,58
mediated vasoconstriction could antagonise insulins Researchers have described an increased prevalence of
eect on glucose uptake via a secondary eect on blood microalbuminuria59 and diminished renal function60 in
ow in skeletal muscle, hyperinsulinaemia might be a individuals with metabolic syndrome. Proteinuria and
result rather than a cause of sympathetic activation in the progressive development of renal dysfunction in
obese people.5 It is not known whether blood ow in obese individuals occurs even in the absence of severe
skeletal muscle is reduced in obesity and contributes to hypertension and diabetes.61 In obese people, high blood
the development of insulin resistance. In young people pressure, glomerular hyperltration, neurohumoral
with metabolic syndrome, forearm blood ow is activation, and metabolic changes that persist might
increased despite increased muscle sympathetic initiate further renal injury. Other factors such as
vasoconstrictor nerve activity and increased activation of the renin-angiotensin system, compression
2-adrenergic-mediated responsiveness.45 Raison and by fat accumulation within and around the kidneys, and
colleagues46 noted increased blood ow in skeletal muscle increased abdominal pressure could further aggravate
in obese hypertensive patients, whereas Ribeiro and and worsen renal impairment.40
colleagues47 noted an association between degree of Studies have shown a detrimental eect of obesity on
sympathetic activation and reduction in forearm blood cardiac structure and function. Obesity is an
ow in obese women.48 An acute increase in activation of independent predictor of left ventricular diastolic
the sympathetic nervous system, within the normal dysfunction in the general population.62 Left ventricular
range of physiological responses, caused acute insulin hypertrophy in people with metabolic syndrome can
resistance in the forearm of healthy individuals.49 occur irrespective of the magnitude of blood pressure
rise,63 indicating that other components of metabolic
Hyperglycaemia syndrome could exert adverse trophic eects on the
In the liver, noradrenaline-immunoreactive bres arise heart. Insulin stimulates growth of vascular smooth
from the coeliac and superior mesenteric ganglia and muscle cells in isolated human arterioles,64 and
project to hepatocytes.50,51 Direct electrical stimulation of structural alterations in the heart in normotensive
the splanchnic nerve leads to an increase in activity of people are related to concentrations of triglycerides and
liver glycogen phosphorylase and glucose-6-phosphatase, glucose.65 Our data show an increased sympathetic
and a rapid and sustained increase in circulating glucose activity after the transition from impaired glucose
4 www.thelancet.com/neurology Published online April 2, 2014 http://dx.doi.org/10.1016/S2213-8587(14)70033-6
Personal View
tolerance to type 2 diabetes that is associated with main driver in sympathetic neural adaptation. This
cardiac enlargement, diastolic dysfunction,66 and pattern of sympathetic activity and its association with
impairment in noradrenaline transporter function.67 In obesity might be aected by factors such as ethnic origin
patients with hypertension, development of left and sex. In African Americans, sympathetic activation is
ventricular hypertrophy is directly linked to the amount strongly associated with BMI in women, whereas in
of spillover of cardiac noradrenaline into plasma and to men, increased muscle sympathetic activity is present in
reduced neuronal noradrenaline reuptake.68 In patients lean people.81 Consistent with these ndings, diet-
with impaired glucose tolerance, a defect in sympathetic induced weight loss in black women was associated with
innervation has been shown.69 Increased noradrenaline a signicant reduction in leptin, abdominal fat mass, and
concentrations might be linked to a reduction in the sympathetic activity, whereas in black men, despite the
expression of nerve growth factor, a molecule that is loss of 11 kg and a diminution in plasma leptin and
essential for the viability of sympathetic nerves.70 visceral abdominal fat, sympathetic activity was
Importantly, the eects of increased bodyweight on the unchanged.82
heart are evident even at young ages. Cardiac structure
has been associated with the degree of sympathetic Pharmacological therapy
activation in young overweight and obese individuals In addition to weight reduction and exercise,
(gure 4).71 Wong and colleagues72 noted that overweight pharmacological inhibition of the sympathetic nervous
people aged about 45 years had subclinical changes in system might be a rational therapeutic approach for
left ventricular structure and function, even after
adjustment for blood pressure, age, sex, and left
Muscle sympathetic nerve activity Endothelial function
ventricular mass. Data from the Bogalusa Heart Study 80 25
indicated that the presence of obesity since childhood
was the only consistent and signicant determinant of 70
20
adverse cardiac remodelling.73 Signicant improvements
Peripheral arterial tonometry ratio
60
in cardiac structure and function have been reported
Bursts per 100 heartbeats
after surgically induced weight loss in severely obese 50
15
adolescents.74 Investigators have reported markers of
40
vascular damage, including arterial stiening,75
endothelial dysfunction,76 and increased carotid intima- 10
30
media thickness,77 in people with metabolic syndrome.
20
Some evidence exists for a link between sympathetic 05
activation and endothelial dysfunction.78 10
Therapeutic implications 0 0
The sympathetic nervous system as a target for therapy Creatinine clearance Left ventricular mass
At present, the main goal in treatment of patients with 250 150
metabolic syndrome is to control individual risk factors
such as overweight and obesity, high blood pressure, and
200
changes in glucose and lipid concentrations. We now
Creatinine clearance (mL/min)
Left ventricular mass index
examine the eects of common therapies for metabolic 100
syndrome on sympathetic activation, and then explore 150
*
the potential of direct modulation of activity of the
sympathetic nervous system as a therapeutic strategy.
100
50
Weight loss and exercise
Weight loss and exercise are key treatments for obesity 50
and metabolic syndrome. Short-term exercise training is
consistently associated with a reduction in sympathetic
0 0
nervous activity and an improvement in blood pressure. Lean individuals Overweight or obese Lean individuals Overweight or obese
In people with metabolic syndrome, weight loss after a individuals individuals
12 week dietary programme was accompanied by a Figure 4: Markers of sympathetic nervous activation and subclinical organ damage in young obese people
signicant reduction in sympathetic nervous activity and Sympathetic overactivation is already evident in very early stages of obesity (mean age 226 years [SE 07] years;
an improvement in all components of metabolic BMI 308 kg/m [11]; range 261501 kg/m) compared with age-matched lean people (226 [07] years;
syndrome.79 A subsequent study showed that the addition 209 kg/m [04], 180247 kg/m) and is associated with early markers of subclinical organ damage. Comparisons
between young lean people and young overweight or obese people for muscle sympathetic nerve activity,
of moderate-intensity aerobic exercise training to a endothelial function, creatinine clearance (with evidence of hyperltration in overweight or obese patients), and
hypocaloric diet did not have additional benets for left ventricular mass index are shown. *p<005, p<001, p<0001. Reproduced from reference 71 with permission
sympathetic tone,80 suggesting that weight loss was the of Wolters Kluwer Health.
www.thelancet.com/neurology Published online April 2, 2014 http://dx.doi.org/10.1016/S2213-8587(14)70033-6 5
Personal View
metabolic syndrome. Rather than being secondary to or Imidazoline I1 receptor agonists act centrally, at the level
reliant on weight reduction, benet associated with of the rostral ventrolateral medulla, to inhibit sympathetic
sympatho-inhibition might be associated with a reduction drive and reduce blood pressure. Drugs in this class, such
in end-organ damage. Several pharmacological approaches as moxonidine and rilmenidine, improve glucose
can lower sympathetic inhibition. -adrenergic blockers metabolism and insulin sensitivity100,101 and are associated
improve blood pressure levels and cholesterol and with a reduction in the progression of microalbuminuria
triglyceride concentrations.83 Decisions about whether the and renal dysfunction.102,103 Other benecial eects on end-
use of -blocker drugs are appropriate in obese people are organ function include reduced left ventricular
problematic. Investigations done from 1986 to 1998 clearly hypertrophy104 and improved endothelial function.105
indicated that blockers such as metoprolol, atenolol, and However, whether these drugs should be used
propranolol were associated with weight gain (particularly preferentially should be used preferentially over other
in the rst few months of use) and a worsening of insulin drug classes in patients with metabolic syndrome and
resistance and lipid prole, thereby favouring the tendency obesity-related hypertension remains to be shown.
of metabolic syndrome patients to develop diabetes.84 By
contrast, use of carvedilol in the GEMINI trial did not lead Device-based therapeutic approaches
to substantial weight gain85 and was associated with an Catheter-based renal denervation is a novel approach to
improvement in lipid prole86 and insulin resistance,87 and more directly target the sympathetic nervous system.
a large reduction in microalbuminuria.88 Clinicians previously used surgical sympathectomy to
Statins are potent inhibitors of cholesterol biosynthesis target sympathetic overactivity in patients with
and their use is established for the primary and secondary uncontrollable high blood pressure, substantially
prevention of coronary artery disease. Statins improve improving cardiovascular outcomes. Endovascular
endothelial function, inammation, and oxidative stress in catheter technology now allows selective denervation of
patients with hypercholesterolaemia and atherosclerosis. the human kidney using radiofrequency energy delivered
Additional pleiotropic eects of statins include an ability to via the renal artery lumen.106 Investigators have done
modulate sympathetic nervous activity.89 Investigators have clinical trials with this minimally invasive technique to
linked increased plasma cholesterol concentrations, even assess its safety and ecacy to lower uncontrolled blood
in the high-to-normal range, to sympathetic nervous pressure in patients with resistant hypertension.
activation and impaired endothelial function in young, Additional potential benets have been described,
otherwise healthy, women.90 Clinical studies show that particularly improvements in glucose metabolism, in
simvastatin reduces muscle sympathetic activity.91,92 In line with the pathophysiological considerations described
men with hypertension and hypercholesterolaemia, the earlier and the close interaction between the sympathetic
improvement in lipid prole that occurred after 8 weeks of nervous system and glucose metabolism. Catheter-based
statin treatment was accompanied by a signicant renal denervation not only lowers renal sympathetic
reduction in muscle sympathetic activity and increased nerve activity, reducing renal noradrenaline spillover by
baroreex sensitivity.91 In patients with non- about 50%,106 but also reduces whole-body sympathetic
hyperlipidaemic hypertension, simvastatin lowered nerve activity and muscle sympathetic nerve activity.107
muscle sympathetic activity and improved endothelium- Increased sympathetic outow to the skeletal muscle
independent vasodilation without aecting plasma lipids.92 vasculature has an important role in glucose metabolism,
Angiotensin-converting enzyme inhibitors and mainly through reduced skeletal muscle blood ow and,
angiotensin-receptor blockers protect the kidney and as a result, diminished uptake of glucose, a hallmark of
heart.93,94 Whether these eects are mediated by interactions insulin resistance.49
between the renin-angiotensin and sympathetic nervous Data from patients that undergo renal denervation for
systems is not known. Intracoronary infusion of resistant hypertension provide evidence to suggest that
angiotensin 2 enhances, and intracoronary inhibition of sympathetic inhibition with this approach can lower
angiotensin-converting enzyme attenuates, sympa- blood pressure and benecially aects glucose
thetically mediated coronary vasoconstriction in patients metabolism.108 Of 50 patients with resistant hypertension,
with mild to severe coronary artery disease,95,96 indicating 37 underwent renal denervation and 13 continued on
that the renin-angiotensin system might allow sympathetic their medication regimen as a control group. In addition
nerve ring. Contrary to this notion, researchers did not to signicant reductions in blood pressure after
show a signicant eect for angiotensin-receptor blockade 1 and 3 months, the investigators noted reduced fasting
on muscle sympathetic nerve activity or the rate of spillover glucose, insulin, C-peptide, and HOMA index, as well as
of noradrenaline to plasma in hypertensive patients.97,98 reduced 2 h glucose during an oral glucose-tolerance test,
Both candesartan and telmisartan similarly reduced blood in patients who underwent renal denervation. By contrast,
pressure in individuals with metabolic syndrome, but they reported no signicant changes in blood pressure or
telmisartan had a larger eect on endothelial function and metabolic markers in the control group (gure 5).
was associated with a reduction in circulating Researchers reported similar outcomes after a study of
noradrenaline concentrations.99 renal denervation in ten patients with obstructive sleep
6 www.thelancet.com/neurology Published online April 2, 2014 http://dx.doi.org/10.1016/S2213-8587(14)70033-6
Personal View
Fasting glucose Fasting insulin
175 p=0366 Renal denervation (n=33) p=0328
15
Control (n=14)
Change in fasting glucose concentration (mg/dL)
Change in fasting insulin concentration (U/mL)
125
10
75 p=0506
5
25 +12
+76 +74
0
68 130 77 89 21
25
5 p=0404
75
10
125 p=0011
p=0033
p=0033
175 p=0006 15
Fasting C-peptide HOMA-IR
20 5
p=0353 p=0143
Change in fasting C-peptide concentraion (ng/ML)
15 4
10
p=0944 3
05
Change in HOMA-IR (ng/mL)
+07 +01 2
00
20 21
05 1
+25
10 0
29 35 09
15 1
20
2 p=0308
25
p=0039 3
30 p=0007
35 4 p=0037
40 5 p=0003
1 month 3 months 1 month 3 months
Figure 5: Changes in fasting glucose, insulin, C-peptide, and HOMA-IR index, after renal denervation in patients with resistant hypertension
P values refer to dierence compared with baseline in same patients. HOMA-IR calculated from the product of fasting plasma glucose and insulin divided by 405.
HOMA-IR=homoeostasis model assessment for insulin resistance. Used from reference 108, with permission of Wolters Kluwer Health.
apnoea.109 Most patients had a decrease in the severity of activation of the sympathetic nervous system has been
obstructive sleep apnoea after renal denervation, and clearly documented both in animals and in human beings
they also had signicantly changed 2 h glucose with obesity and metabolic syndrome. Furthermore,
concentrations during an oral glucose-tolerance test, and disorders commonly associated with obesity and metabolic
reduced HbA1c after 6 months. Investigators using a syndrome, such as hypertension, diastolic dysfunction,
hyperinsulinaemiceuglycaemic clamp technique to and renal impairment, are modulated by the sympathetic
assess insulin sensitivity reported that two patients with nervous system. Mechanistically, sympathetic nervous
resistant hypertension and metabolic disturbances activation aects relevant aspects of the pathophysiology
associated with polycystic ovary syndrome had improved that underlies obesity and its metabolic eects, perhaps
insulin sensitivity associated with reductions in best shown by insulin resistance occurring in response to
sympathetic nerve activity induced by renal denervation.110 an acute increase in sympathetic drive. Although the exact
These data are promising, but preliminary; additional nature of the association between sympathetic activation
studies are needed to dene the mechanisms by which and the metabolic results of obesity remains to be
renal denervation can lower blood glucose and improve determined, some evidence suggests a key role for the
insulin sensitivity in patients with resistant hypertension sympathetic nervous system in the generation of obesity
or other cardiovascular diseases. and metabolic syndrome. Common metabolic syndrome
treatments such as weight loss and exercise have been
Conclusions and future directions associated with large reductions in the activity of the
Aside from its well described eects on cardiovascular sympathetic nervous system. To target the sympathetic
control, accumulating data from laboratory and clinical nervous system directlyeither with drugs or with novel
studies now provide compelling evidence for an important device-based interventionsseems to be a logical and
role for the sympathetic nervous system in obesity and attractive next step, particularly since many patients with
metabolic syndrome. With use of state-of-the-art methods, obesity and metabolic syndrome do not achieve sustained
www.thelancet.com/neurology Published online April 2, 2014 http://dx.doi.org/10.1016/S2213-8587(14)70033-6 7
Personal View
9 Julius S, Gudbrandsson T, Jamerson K, Andersson O. The
Search strategy and selection criteria interconnection between sympathetics, microcirculation, and
insulin resistance in hypertension. Blood Press 1992; 1: 919.
We searched Medline and Embase with the terms 10 Masuo K, Mikami H, Ogihara T, Tuck ML. Sympathetic nerve
sympathetic, metabolic syndrome, diabetes, hyperactivity precedes hyperinsulinemia and blood pressure
elevation in a young, nonobese Japanese population. Am J Hypertens
dyslipidemia, insulin resistance, hypertension, and 1997; 10: 7783.
obesity. We limited our search to articles written in English 11 Masuo K, Mikami H, Ogihara T, Tuck ML. Weight gain-induced
and published between Jan 1, 2000, and June 30, 2013, but did blood pressure elevation. Hypertension 2000; 35: 113540.
12 Gudmundsdottir H, Strand A, Kjeldsen S, Hoieggen A, Os I.
not exclude commonly referenced and highly regarded older Arterial noradrenaline predicts rise in body mass index in a 20-year
articles. We read the relevant papers and used their follow-up of lean normotensive and hypertensive men. J Hypertens
bibliographies further to identify other works for inclusion. 2008; 26: S347.
13 Kalil GZ, Haynes WG. Sympathetic nervous system in
obesity-related hypertension: mechanisms and clinical implications.
Hypertens Res 2012; 35: 416.
weight loss. Although promising preliminary data exist, 14 Gentile CL, Orr JS, Davy BM, Davy KP. Modest weight gain is
further studies are needed to substantiate the role of the associated with sympathetic neural activation in nonobese humans.
Am J Physiol Regul Integr Comp Physiol 2007; 292: R183438.
sympathetic nervous system as a useful therapeutic target.
15 Straznicky NE, Grima MT, Eikelis N, et al. The eects of weight loss
Contributors versus weight loss maintenance on sympathetic nervous system
All authors contributed to the conception and design, acquisition of data, activity and metabolic syndrome components.
or analysis and interpretation of data for this Personal View; drafted or J Clin Endocrinol Metab 2011; 96: E50308.
revised the Personal View; and approved the nal version. 16 Alvarez GE, Beske SD, Ballard TP, Davy KP. Sympathetic neural
activation in visceral obesity. Circulation 2002; 106: 253336.
Declaration of interests 17 Zubcevic J, Waki H, Raizada MK, Paton JF. Autonomic-immune-
MS and GL receive research funding from the National Health and vascular interaction: an emerging concept for neurogenic
Medical Research Council of Australia (NHMRC), Medtronic, Abbott hypertension. Hypertension 2011; 57: 102633.
Pharmaceuticals, Servier Australia, and Allergan, and are supported by 18 Harrison DG, Guzik TJ, Lob HE, et al. Inammation, immunity,
NHMRC Research Fellowships. MS serves on scientic advisory boards and hypertension. Hypertension 2011; 57: 13240.
for Abbott Pharmaceuticals, Novartis Pharmaceuticals, and Medtronic, 19 Charles MA, Eschwge E, Thibult N, et al. The role of non-esteried
and has received honoraria and travel support from Abbott, Servier, fatty acids in the deterioration of glucose tolerance in Caucasian
Novartis, MSD, Boehringer Ingelheim, and Medtronic. GL has acted as a subjects: results of the Paris Prospective Study. Diabetologia 1997;
consultant for Medtronic and has received honoraria or travel support 40: 110106.
for presentations from Pzer, Wyeth Pharmaceuticals, Servier, and 20 Maison P, Byrne CD, Hales CN, Wareham NJ. Hypertension and its
Medtronic. NS receives research funding from the NHMRC, National treatment inuence changes in fasting nonesteried fatty acid
Heart Foundation, and Diabetes Australia. EL receives research funding concentrations: a link between the sympathetic nervous system and
from the NHMRC. the metabolic syndrome? Metabolism 2000; 49: 8187.
21 Haastrup AT, Stepniakowski KT, Goodfriend TL, Egan BM.
Acknowledgments Intralipid enhances alpha1-adrenergic receptor mediated pressor
The writing of this Personal View was supported by the NHMRC and, in sensitivity. Hypertension 1998; 32: 69398.
part, by the Victoria Governments Operation Infrastructure Support 22 Florian JP, Pawelczyk JA. Non-esteried fatty acids increase arterial
Program. pressure via central sympathetic activation in humans.
References Clin Sci (Lond) 2010; 118: 6169.
1 Alberti KG, Zimmet P, Shaw J; for the IDF Epidemiology Task 23 Grekin RJ, Ngarmukos CO, Williams DM, Supiano MA. Renal
Force Consensus Group. The metabolic syndromea new norepinephrine spillover during infusion of nonesteried fatty
worldwide denition. Lancet 2005; 366: 105962. acids. Am J Hypertens 2005; 18: 42226.
2 Alberti KG, Eckel RH, Grundy SM, et al; for the International 24 Machleidt F, Simon P, Krapalis AF, Hallschmid M, Lehnert H,
Diabetes Federation Task Force on Epidemiology and Prevention, Sayk F. Experimental hyperleptinemia acutely increases
and the Hational Heart, Lung, and Blood Institute, and the vasoconstrictory sympathetic nerve activity in healthy humans.
American Heart Association, and the World Heart Federation, and J Clin Endocrinol Metab 2013; 98: E49196.
the International Atherosclerosis Society, and the International 25 Eikelis N, Schlaich M, Aggarwal A, Kaye D, Esler M. Interactions
Association for the Study of Obesity. Harmonizing the metabolic between leptin and the human sympathetic nervous system.
syndrome: a joint interim statement of the International Diabetes Hypertension 2003; 41: 107279.
Federation Task Force on Epidemiology and Prevention; National 26 Dusserre E, Moulin P, Vidal H. Dierences in mRNA expression of
Heart, Lung, and Blood Institute; American Heart Association; the proteins secreted by the adipocytes in human subcutaneous and
World Heart Federation; International Atherosclerosis Society; and visceral adipose tissues. Biochim Biophys Acta 2000; 1500: 8896.
International Association for the Study of Obesity. Circulation 2009; 27 Alvarez GE, Ballard TP, Beske SD, Davy KP. Subcutaneous obesity
120: 164045. is not associated with sympathetic neural activation.
3 Jrhult J, Falck B, Ingemansson S, Nobin A. The functional Am J Physiol Heart Circ Physiol 2004; 287: H41418.
importance of sympathetic nerves to the liver and endocrine 28 Bjrntorp P. Neuroendocrine abnormalities in human obesity.
pancreas. Ann Surg 1979; 189: 96100. Metabolism 1995; 44 (suppl 2): 3841.
4 Esler M, Straznicky N, Eikelis N, Masuo K, Lambert G, Lambert E. 29 Esler M, Eikelis N, Schlaich M, et al. Chronic mental stress is a
Mechanisms of sympathetic activation in obesity-related cause of essential hypertension: presence of biological markers of
hypertension. Hypertension 2006; 48: 78796. stress. Clin Exp Pharmacol Physiol 2008; 35: 498502.
5 Mancia G, Bousquet P, Elghozi JL, et al. The sympathetic nervous 30 Vicennati V, Pasqui F, Cavazza C, Pagotto U, Pasquali R.
system and the metabolic syndrome. J Hypertens 2007; 25: 90920. Stress-related development of obesity and cortisol in women.
6 Landsberg L, Young JB. Fasting, feeding and regulation of the Obesity (Silver Spring) 2009; 17: 167883.
sympathetic nervous system. N Engl J Med 1978; 298: 1295301. 31 Zhang J, Niaura R, Dyer JR, et al. Hostility and urine
7 Reaven G. The metabolic syndrome or the insulin resistance norepinephrine interact to predict insulin resistance: the VA
syndrome? Dierent names, dierent concepts, and dierent goals. Normative Aging Study. Psychosom Med 2006; 68: 71826.
Endocrinol Metab Clin North Am 2004; 33: 283303. 32 Brunner EJ, Chandola T, Marmot MG. Prospective eect of job
8 Grundy SM. What is the contribution of obesity to the metabolic strain on general and central obesity in the Whitehall II Study.
syndrome? Endocrinol Metab Clin North Am 2004; 33: 26782. Am J Epidemiol 2007; 165: 82837.
8 www.thelancet.com/neurology Published online April 2, 2014 http://dx.doi.org/10.1016/S2213-8587(14)70033-6
Personal View
33 Heraclides A, Chandola T, Witte DR, Brunner EJ. Psychosocial stress 55 Hsu CY, McCulloch CE, Iribarren C, Darbinian J, Go AS. Body
at work doubles the risk of type 2 diabetes in middle-aged women: mass index and risk for end-stage renal disease. Ann Intern Med
evidence from the Whitehall II study. Diabetes Care 2009; 32: 223035. 2006; 144: 2128.
34 Coughlin SR, Mawdsley L, Mugarza JA, Calverley PM, Wilding JP. 56 Ejerblad E, Fored CM, Lindblad P, Fryzek J, McLaughlin JK,
Obstructive sleep apnoea is independently associated with an Nyrn O. Obesity and risk for chronic renal failure.
increased prevalence of metabolic syndrome. Eur Heart J 2004; J Am Soc Nephrol 2006; 17: 1695702.
25: 73541. 57 Bonnet F, Deprele C, Sassolas A, et al. Excessive body weight as a
35 Trombetta IC, Maki-Nunes C, Toschi-Dias E, et al. Obstructive sleep new independent risk factor for clinical and pathological progression
apnea is associated with increased chemoreex sensitivity in in primary IgA nephritis. Am J Kidney Dis 2001; 37: 72027.
patients with metabolic syndrome. Sleep 2013; 36: 4149. 58 Praga M, Hernndez E, Herrero JC, et al. Inuence of obesity on
36 Grassi G, Facchini A, Trevano FQ, et al. Obstructive sleep apnea- the appearance of proteinuria and renal insuciency after
dependent and -independent adrenergic activation in obesity. unilateral nephrectomy. Kidney Int 2000; 58: 211118.
Hypertension 2005; 46: 32125. 59 Palaniappan L, Carnethon M, Fortmann SP. Association between
37 Narkiewicz K, Kato M, Phillips BG, Pesek CA, Davison DE, microalbuminuria and the metabolic syndrome: NHANES III.
Somers VK. Nocturnal continuous positive airway pressure Am J Hypertens 2003; 16: 95258.
decreases daytime sympathetic trac in obstructive sleep apnea. 60 Chen J, Muntner P, Hamm LL, et al. The metabolic syndrome and
Circulation 1999; 100: 233235. chronic kidney disease in U.S. adults. Ann Intern Med 2004;
38 Harsch IA, Schahin SP, Radespiel-Trger M, et al. Continuous 140: 16774.
positive airway pressure treatment rapidly improves insulin 61 Henegar JR, Bigler SA, Henegar LK, Tyagi SC, Hall JE. Functional
sensitivity in patients with obstructive sleep apnea syndrome. and structural changes in the kidney in the early stages of obesity.
Am J Respir Crit Care Med 2004; 169: 15662. J Am Soc Nephrol 2001; 12: 121117.
39 Straznicky N, Grassi G, Esler M, et al, for the European Society of 62 Levy D, Garrison RJ, Savage DD, Kannel WB, Castelli WP.
Hypertension Working Group on Obesity, and the Australian, New Prognostic implications of echocardiographically determined left
Zealand Obesity Society. European Society of Hypertension working ventricular mass in the Framingham Heart Study. N Engl J Med
group on obesity antihypertensive eects of weight loss: myth or 1990; 322: 156166.
reality? J Hypertens 2010; 28: 63743. 63 Davis CL, Kapuku G, Snieder H, Kumar M, Treiber FA. Insulin
40 Hall JE, Jones DW, Kuo JJ, da Silva A, Tallam LS, Liu J. Impact of resistance syndrome and left ventricular mass in healthy young
the obesity epidemic on hypertension and renal disease. people. Am J Med Sci 2002; 324: 7275.
Curr Hypertens Rep 2003; 5: 38692. 64 Doronzo G, Russo I, Mattiello L, Anfossi G, Bosia A, Trovati M.
41 Gilardini L, Parati G, Sartorio A, Mazzilli G, Pontiggia B, Invitti C. Insulin activates vascular endothelial growth factor in vascular
Sympathoadrenergic and metabolic factors are involved in smooth muscle cells: inuence of nitric oxide and of insulin
ambulatory blood pressure rise in childhood obesity. resistance. Eur J Clin Invest 2004; 34: 66473.
J Hum Hypertens 2008; 22: 7582. 65 Ferrara AL, Vaccaro O, Cardoni O, Panarelli W, Laurenzi M,
42 Shibao C, Gamboa A, Diedrich A, et al. Autonomic contribution to Zanchetti A. Is there a relationship between left ventricular mass and
blood pressure and metabolism in obesity. Hypertension 2007; plasma glucose and lipids independent of body mass index? Results
49: 2733. of the Gubbio Study. Nutr Metab Cardiovasc Dis 2003; 13: 12632.
43 Shibasaki S, Eguchi K, Matsui Y, et al, for the Japan Morning 66 Straznicky NE, Grima MT, Sari CI, et al. The relation of glucose
Surge-1 (JMS-1) study group. Adrenergic blockade improved insulin metabolism to left ventricular mass and function and sympathetic
resistance in patients with morning hypertension: the Japan nervous system activity in obese subjects with metabolic syndrome.
Morning Surge-1 study. J Hypertens 2009; 27: 125257. J Clin Endocrinol Metab 2013; 98: E22737.
44 Lambert E, Straznicky N, Schlaich M, et al. Diering pattern of 67 Straznicky NE, Lambert EA, Grima MT, et al. The eects of dietary
sympathoexcitation in normal-weight and obesity-related weight loss on indices of norepinephrine turnover: Modulatory
hypertension. Hypertension 2007; 50: 86268. inuence of hyperinsulinemia. Obesity (Silver Spring) 2013;
45 Limberg JK, Morgan BJ, Sebranek JJ, et al. Altered neurovascular published online Sep 2. DOI:10.1002/oby.20614.
control of the resting circulation in human metabolic syndrome. 68 Schlaich MP, Kaye DM, Lambert E, Sommerville M, Socratous F,
J Physiol 2012; 590: 610919. Esler MD. Relation between cardiac sympathetic activity and
46 Raison JM, Safar ME, Cambien FA, London GM. Forearm hypertensive left ventricular hypertrophy. Circulation 2003;
haemodynamics in obese normotensive and hypertensive subjects. 108: 56065.
J Hypertens 1988; 6: 299303. 69 Ziegler D, Weise F, Langen KJ, et al. Eect of glycaemic control on
47 Ribeiro MM, Trombetta IC, Batalha LT, et al. Muscle sympathetic myocardial sympathetic innervation assessed by [123I]
nerve activity and hemodynamic alterations in middle-aged obese metaiodobenzylguanidine scintigraphy: a 4-year prospective study
women. Braz J Med Biol Res 2001; 34: 47578. in IDDM patients. Diabetologia 1998; 41: 44351.
48 Kuniyoshi FH, Trombetta IC, Batalha LT, et al. Abnormal 70 Kaye DM, Vaddadi G, Gruskin SL, Du XJ, Esler MD. Reduced
neurovascular control during sympathoexcitation in obesity. myocardial nerve growth factor expression in human and
Obes Res 2003; 11: 141119. experimental heart failure. Circ Res 2000; 86: E8084.
49 Jamerson KA, Julius S, Gudbrandsson T, Andersson O, Brant DO. 71 Lambert E, Sari CI, Dawood T, et al. Sympathetic nervous system
Reex sympathetic activation induces acute insulin resistance in the activity is associated with obesity-induced subclinical organ damage
human forearm. Hypertension 1993; 21: 61823. in young adults. Hypertension 2010; 56: 35158.
50 Tiniakos DG, Lee JA, Burt AD. Innervation of the liver: morphology 72 Wong CY, OMoore-Sullivan T, Leano R, Byrne N, Beller E,
and function. Liver 1996; 16: 15160. Marwick TH. Alterations of left ventricular myocardial characteristics
51 Akiyoshi H, Gonda T, Terada T. A comparative histochemical and associated with obesity. Circulation 2004; 110: 308187.
immunohistochemical study of aminergic, cholinergic and 73 Toprak A, Wang H, Chen W, Paul T, Srinivasan S, Berenson G.
peptidergic innervation in rat, hamster, guinea pig, dog and human Relation of childhood risk factors to left ventricular hypertrophy
livers. Liver 1998; 18: 35259. (eccentric or concentric) in relatively young adulthood (from the
52 Dicostanzo CA, Dardevet DP, Neal DW, et al. Role of the hepatic Bogalusa Heart Study). Am J Cardiol 2008; 101: 162125.
sympathetic nerves in the regulation of net hepatic glucose uptake 74 Ippisch HM, Inge TH, Daniels SR, et al. Reversibility of cardiac
and the mediation of the portal glucose signal. abnormalities in morbidly obese adolescents. J Am Coll Cardiol
Am J Physiol Endocrinol Metab 2006; 290: E916. 2008; 51: 134248.
53 Petrides AS, DeFronzo RA. Glucose metabolism in cirrhosis: a 75 Wildman RP, Mackey RH, Bostom A, Thompson T,
review with some perspectives for the future. Diabetes Metab Rev Sutton-Tyrrell K. Measures of obesity are associated with vascular
1989; 5: 691709. stiness in young and older adults. Hypertension 2003; 42: 46873.
54 Merli M, Leonetti F, Riggio O, et al. Glucose intolerance and insulin 76 Lteif AA, Han K, Mather KJ. Obesity, insulin resistance, and the
resistance in cirrhosis are normalized after liver transplantation. metabolic syndrome: determinants of endothelial dysfunction in
Hepatology 1999; 30: 64954. whites and blacks. Circulation 2005; 112: 3238.
www.thelancet.com/neurology Published online April 2, 2014 http://dx.doi.org/10.1016/S2213-8587(14)70033-6 9
Personal View
77 Tzou WS, Douglas PS, Srinivasan SR, et al. Increased subclinical 95 Saino A, Pomidossi G, Perondi R, Morganti A, Turolo L, Mancia G.
atherosclerosis in young adults with metabolic syndrome: the Modulation of sympathetic coronary vasoconstriction by cardiac
Bogalusa Heart Study. J Am Coll Cardiol 2005; 46: 45763. renin-angiotensin system in human coronary heart disease.
78 Sverrisdttir YB, Jansson LM, Hgg U, Gan LM. Muscle Circulation 2000; 101: 227783.
sympathetic nerve activity is related to a surrogate marker of 96 Saino A, Pomidossi G, Perondi R, et al. Intracoronary angiotensin
endothelial function in healthy individuals. PLoS One 2010; 5: e9257. II potentiates coronary sympathetic vasoconstriction in humans.
79 Straznicky NE, Lambert EA, Lambert GW, Masuo K, Esler MD, Circulation 1997; 96: 14853.
Nestel PJ. Eects of dietary weight loss on sympathetic activity and 97 Grassi G, Turri C, DellOro R, Stella ML, Bolla GB, Mancia G. Eect
cardiac risk factors associated with the metabolic syndrome. of chronic angiotensin converting enzyme inhibition on
J Clin Endocrinol Metab 2005; 90: 59986005. sympathetic nerve trac and baroreex control of the circulation in
80 Straznicky NE, Lambert EA, Nestel PJ, et al. Sympathetic neural essential hypertension. J Hypertens 1998; 16: 178996.
adaptation to hypocaloric diet with or without exercise training in 98 Krum H, Lambert E, Windebank E, Campbell DJ, Esler M. Eect of
obese metabolic syndrome subjects. Diabetes 2010; 59: 7179. angiotensin II receptor blockade on autonomic nervous system
81 Abate NI, Mansour YH, Tuncel M, et al. Overweight and function in patients with essential hypertension.
sympathetic overactivity in black Americans. Hypertension 2001; Am J Physiol Heart Circ Physiol 2006; 290: H170612.
38: 37983. 99 Kishi T, Hirooka Y, Konno S, Sunagawa K. Angiotensin II receptor
82 Abbas A, Szczepaniak LS, Tuncel M, et al. Adiposity-independent blockers improve endothelial dysfunction associated with
sympathetic activity in black men. J Appl Physiol (1985) 2010; sympathetic hyperactivity in metabolic syndrome. J Hypertens 2012;
108: 161318. 30: 164655.
83 Itskovitz HD. Alpha 1-blockade for the treatment of hypertension: 100 Chazova I, Almazov VA, Shlyakhto E. Moxonidine improves
a megastudy of terazosin in 2214 clinical practice settings. Clin Ther glycaemic control in mildly hypertensive, overweight patients: a
1994; 16: 490504. comparison with metformin. Diabetes Obes Metab 2006; 8: 45665.
84 Sharma AM, Pischon T, Hardt S, Kunz I, Luft FC. Hypothesis: 101 Haenni A, Lithell H. Moxonidine improves insulin sensitivity in
beta-adrenergic receptor blockers and weight gain: a systematic insulin-resistant hypertensives. J Hypertens Suppl 1999; 17: S2935.
analysis. Hypertension 2001; 37: 25054. 102 Strojek K, Grzeszczak W, Grska J, Leschinger MI, Ritz E. Lowering
85 Messerli FH, Bell DS, Fonseca V, et al, for the GEMINI of microalbuminuria in diabetic patients by a sympathicoplegic
Investigators. Body weight changes with beta-blocker use: results agent: novel approach to prevent progression of diabetic
from GEMINI. Am J Med 2007; 120: 61015. nephropathy? J Am Soc Nephrol 2001; 12: 60205.
86 Bell DS, Bakris GL, McGill JB. Comparison of carvedilol and 103 Vonend O, Marsalek P, Russ H, Wulkow R, Oberhauser V,
metoprolol on serum lipid concentration in diabetic hypertensive Rump LC. Moxonidine treatment of hypertensive patients with
patients. Diabetes Obes Metab 2009; 11: 23438. advanced renal failure. J Hypertens 2003; 21: 170917.
87 Fonseca V, Bakris GL, Bell DS, et al, for the GEMINI Investigators. 104 Prichard BN, Graham BR, Owens CW. Moxonidine: a new
Dierential eect of beta-blocker therapy on insulin resistance as a antiadrenergic antihypertensive agent. J Hypertens Suppl 1999;
function of insulin sensitizer use: results from GEMINI. 17: S4154.
Diabet Med 2007; 24: 75963. 105 Topal E, Cikim AS, Cikim K, Temel I, Ozdemir R. The eect of
88 Bakris GL, Fonseca V, Katholi RE, et al, for the GEMINI moxonidine on endothelial dysfunction in metabolic syndrome.
Investigators. Dierential eects of beta-blockers on albuminuria in Am J Cardiovasc Drugs 2006; 6: 34348.
patients with type 2 diabetes. Hypertension 2005; 46: 130915. 106 Krum H, Schlaich M, Whitbourn R, et al. Catheter-based renal
89 Millar PJ, Floras JS. Statins and the autonomic nervous system. sympathetic denervation for resistant hypertension: a multicentre
Clin Sci (Lond) 2014; 126: 40115. safety and proof-of-principle cohort study. Lancet 2009; 373: 127581.
90 Lambert E, Straznicky N, Sari CI, et al. Dyslipidemia is associated 107 Hering D, Lambert EA, Marusic P, et al. Substantial reduction in
with sympathetic nervous activation and impaired endothelial single sympathetic nerve ring after renal denervation in patients
function in young females. Am J Hypertens 2013; 26: 25056. with resistant hypertension. Hypertension 2013; 61: 45764.
91 Lewandowski J, Siski M, Bidiuk J, et al. Simvastatin reduces 108 Mahfoud F, Schlaich M, Kindermann I, et al. Eect of renal
sympathetic activity in men with hypertension and sympathetic denervation on glucose metabolism in patients with
hypercholesterolemia. Hypertens Res 2010; 33: 1038-43. resistant hypertension: a pilot study. Circulation 2011; 123: 194046.
92 McGowan CL, Murai H, Millar PJ, Notarius CF, Morris BL, 109 Witkowski A, Prejbisz A, Florczak E, et al. Eects of renal
Floras JS. Simvastatin reduces sympathetic outow and augments sympathetic denervation on blood pressure, sleep apnea course,
endothelium-independent dilation in non-hyperlipidaemic primary and glycemic control in patients with resistant hypertension and
hypertension. Heart 2013; 99: 24046. sleep apnea. Hypertension 2011; 58: 55965.
93 Brenner BM, Cooper ME, de Zeeuw D, et al, for the RENAAL Study 110 Schlaich MP, Straznicky N, Grima M, et al. Renal denervation: a
Investigators. Eects of losartan on renal and cardiovascular potential new treatment modality for polycystic ovary syndrome?
outcomes in patients with type 2 diabetes and nephropathy. J Hypertens 2011; 29: 99196.
N Engl J Med 2001; 345: 86169.
94 Dahlf B, Devereux RB, Kjeldsen SE, et al, for the LIFE Study
Group. Cardiovascular morbidity and mortality in the losartan
intervention for endpoint reduction in hypertension study (LIFE):
a randomised trial against atenolol. Lancet 2002; 359: 9951003.
10 www.thelancet.com/neurology Published online April 2, 2014 http://dx.doi.org/10.1016/S2213-8587(14)70033-6
Вам также может понравиться
- Research Papers in Violin Acoustics (Vol 1) PDFДокумент700 страницResearch Papers in Violin Acoustics (Vol 1) PDFmonte100% (1)
- Ingested Hyaluronan Moisturizes Dry Skin Kawada2014 PDFДокумент9 страницIngested Hyaluronan Moisturizes Dry Skin Kawada2014 PDFmonteОценок пока нет
- Elastin Hydrolysate Derived From Fish Enhances Proliferation of Human Skin Fibroblasts Shiratsuchi2015Документ6 страницElastin Hydrolysate Derived From Fish Enhances Proliferation of Human Skin Fibroblasts Shiratsuchi2015monteОценок пока нет
- Measures of Postprandial Wellness After Single Intake of Two Boelsma2010Документ9 страницMeasures of Postprandial Wellness After Single Intake of Two Boelsma2010monteОценок пока нет
- Inflammation and The Metabolic SyndromeДокумент13 страницInflammation and The Metabolic SyndromemonteОценок пока нет
- The Geometric PrinciplesДокумент21 страницаThe Geometric PrinciplesmonteОценок пока нет
- Third ConditionalДокумент0 страницThird ConditionalGregorio RamirezОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Anti Diabetic DrugsДокумент54 страницыAnti Diabetic Drugsmanj99Оценок пока нет
- Coy Diet Patient BrochureДокумент32 страницыCoy Diet Patient BrochureRebeca Daniela CherloabaОценок пока нет
- Alteration of Metabolic Profiles in Young and Adult Murrah Buffaloes Exposed To Acute Heat StressДокумент8 страницAlteration of Metabolic Profiles in Young and Adult Murrah Buffaloes Exposed To Acute Heat StressAna Júlia LogradoОценок пока нет
- Biochem 442 Ruohola-Baker Midterm 2Документ18 страницBiochem 442 Ruohola-Baker Midterm 2bpwalshОценок пока нет
- Sample RCP-FlattenedДокумент238 страницSample RCP-FlattenedTahir AliОценок пока нет
- 6 Bodily Tissues That Can Be Regenerated Through NutritionДокумент16 страниц6 Bodily Tissues That Can Be Regenerated Through Nutritionjanroos1Оценок пока нет
- NP3 Nursing Board Exam December 2006 Answer Key 'Nursing Care of Client With Physiological and Psychosocial Alteration'Документ13 страницNP3 Nursing Board Exam December 2006 Answer Key 'Nursing Care of Client With Physiological and Psychosocial Alteration'Marjorie RefuerzoОценок пока нет
- A Systematic Review On The Pre-Clinical Study of Cephalandra Indica and Gymnema Sylvestre in Diabetes Mellitus Type 2Документ7 страницA Systematic Review On The Pre-Clinical Study of Cephalandra Indica and Gymnema Sylvestre in Diabetes Mellitus Type 2International Journal of Innovative Science and Research TechnologyОценок пока нет
- HESI CASE STUDY - Gestational DiabetesДокумент17 страницHESI CASE STUDY - Gestational DiabetesDrSandHill67% (6)
- Biology PancreasДокумент10 страницBiology Pancreasjavier orellana mejiaОценок пока нет
- Insulinas de OsmosisДокумент3 страницыInsulinas de OsmosisDennise A. Hernández JuárezОценок пока нет
- Cadayona-Clinical Sas 4Документ33 страницыCadayona-Clinical Sas 4kateОценок пока нет
- Classifications of Insulin2Документ116 страницClassifications of Insulin2loglesb1Оценок пока нет
- Drugs For Diabetes (Part 1)Документ6 страницDrugs For Diabetes (Part 1)حوراء عارف الموسويОценок пока нет
- Pathophysiology of Diabetes Mellitus Type Ii With ComplicationsДокумент4 страницыPathophysiology of Diabetes Mellitus Type Ii With ComplicationsEricka Genove100% (1)
- Getting Started With Insulin InjectionsДокумент4 страницыGetting Started With Insulin InjectionsJianhua ShiОценок пока нет
- Labor Cases Full TextДокумент66 страницLabor Cases Full TextRian Niño TrinidadОценок пока нет
- Feedback MechanismДокумент25 страницFeedback Mechanismkaloy domanaisОценок пока нет
- Understanding Diabetes: A Treatise For The General PublicДокумент6 страницUnderstanding Diabetes: A Treatise For The General PublicRaghuvir Keni Jr.Оценок пока нет
- PROJECTДокумент38 страницPROJECTJohnОценок пока нет
- Clinical ChemistryДокумент7 страницClinical Chemistrysciencetopic4Оценок пока нет
- Digital Technology For DiabetesДокумент11 страницDigital Technology For Diabetesvvandv123Оценок пока нет
- Elliot Hulse - Rational Fasting Diet ManualДокумент43 страницыElliot Hulse - Rational Fasting Diet ManualRyan Franco96% (27)
- Muscle Maximum Growth IIДокумент116 страницMuscle Maximum Growth IIAlex Antoniou88% (16)
- Obesity-code-Jason FungДокумент10 страницObesity-code-Jason Fungsimas0% (1)
- Personal Fat ThresholdДокумент6 страницPersonal Fat ThresholdPROJETO PRI E GABIОценок пока нет
- (Diabetes No More) Diabetes DestroyerДокумент30 страниц(Diabetes No More) Diabetes Destroyerzigzag7842611100% (1)
- Epn 3 Modul 1 StudentДокумент3 страницыEpn 3 Modul 1 StudentLukman Kim HakimОценок пока нет
- Type 2 Diabetes MellitusДокумент4 страницыType 2 Diabetes MellitususaantiniОценок пока нет
- Dietary Management of Indian Vegetarian Diabetics: M. Viswanathan and V. MohanДокумент2 страницыDietary Management of Indian Vegetarian Diabetics: M. Viswanathan and V. Mohanrockingtwo07Оценок пока нет