Вам также может понравиться
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Fraser Island MapДокумент1 страницаFraser Island Mapmohammed el erianОценок пока нет
- Downtown Map 2015 WhiteДокумент1 страницаDowntown Map 2015 Whitemohammed el erianОценок пока нет
- Ancient Egypt & Civilizations Map: Name - HourДокумент2 страницыAncient Egypt & Civilizations Map: Name - Hourmohammed el erianОценок пока нет
- Egypt PDFДокумент1 страницаEgypt PDFmohammed el erianОценок пока нет
- Channel Islands: Hiking Eastern Santa Cruz IslandДокумент2 страницыChannel Islands: Hiking Eastern Santa Cruz Islandmohammed el erianОценок пока нет
- Anchorage Map JHДокумент1 страницаAnchorage Map JHmohammed el erianОценок пока нет
- Trans Alaska Pipeline System: P.O. Box 196660, MS 542 Anchorage, Alaska 99519-6660 2016Документ66 страницTrans Alaska Pipeline System: P.O. Box 196660, MS 542 Anchorage, Alaska 99519-6660 2016mohammed el erianОценок пока нет
- Three Months EIBOR Rates Trend - HSBC Review MonthsДокумент1 страницаThree Months EIBOR Rates Trend - HSBC Review Monthsmohammed el erianОценок пока нет
- BP RP30 4 PDFДокумент136 страницBP RP30 4 PDFmohammed el erian100% (1)
- Mike Tyson: Undisputed TruthДокумент1 страницаMike Tyson: Undisputed Truthmohammed el erianОценок пока нет
- Ins SesignДокумент65 страницIns SesignRakesh Nayak100% (1)
- Example: - Derive Wet Unit Weight With Dry Unit Weight and and Water Content. - SolutionДокумент1 страницаExample: - Derive Wet Unit Weight With Dry Unit Weight and and Water Content. - Solutionmohammed el erianОценок пока нет
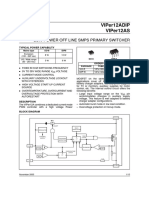
- Viper12Adip Viper12As: Low Power Off Line Smps Primary SwitcherДокумент16 страницViper12Adip Viper12As: Low Power Off Line Smps Primary Switchermohammed el erianОценок пока нет
- 28FCS147Practice Exercise 1Документ3 страницы28FCS147Practice Exercise 1mohammed el erianОценок пока нет
- The Dubai Mall Map: Parking CinemaДокумент2 страницыThe Dubai Mall Map: Parking Cinemamohammed el erianОценок пока нет
- 28FCS147Practice Exercise 1Документ2 страницы28FCS147Practice Exercise 1mohammed el erianОценок пока нет
- Homework 5 SolutionДокумент7 страницHomework 5 Solutionmohammed el erianОценок пока нет
- Homework 5 SolutionДокумент7 страницHomework 5 Solutionmohammed el erianОценок пока нет
- Arctic Engineering Module 5aДокумент30 страницArctic Engineering Module 5amohammed el erianОценок пока нет
- Arctic Engineering Module 5bДокумент30 страницArctic Engineering Module 5bmohammed el erianОценок пока нет
- 4a ScriptДокумент51 страница4a Scriptmohammed el erianОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Above The Law (2020)Документ23 страницыAbove The Law (2020)Western Sahara Resource WatchОценок пока нет
- Ordinance 2018-01 S. 2018 - Barangay Official Seal OrdinanceДокумент5 страницOrdinance 2018-01 S. 2018 - Barangay Official Seal OrdinanceRobe Jan Ivan Pagulong100% (3)
- Gurrea V LezamaДокумент2 страницыGurrea V LezamaEdward Kenneth Kung100% (1)
- NationalismДокумент5 страницNationalismFahwhwhwywwywyywgОценок пока нет
- Blackbirded Sicilians LouisianaДокумент2 страницыBlackbirded Sicilians LouisianaAuntie DogmaОценок пока нет
- 1 StarhawkДокумент5 страниц1 StarhawkЯрослав ДерубаОценок пока нет
- Garcia, Nehemiah B. BSN 2Y2 - 2A TLWD 111Документ2 страницыGarcia, Nehemiah B. BSN 2Y2 - 2A TLWD 111Mushy_aya100% (1)
- Delhi 2024Документ2 страницыDelhi 2024jeetukumarjk1991Оценок пока нет
- 65 RR - LPC Forwarding LetterДокумент46 страниц65 RR - LPC Forwarding LetterAbhijeet Singh KadianОценок пока нет
- MAY 19, 1898 JUNE 23, 1898: The Return of Aguinaldo To The PhilippinesДокумент9 страницMAY 19, 1898 JUNE 23, 1898: The Return of Aguinaldo To The PhilippinesCriziaClaire CosmeОценок пока нет
- Human TraffickingДокумент1 страницаHuman TraffickingBest ComparisonОценок пока нет
- Two Re Foundation Projects of Democracy in Contemporary French Philosophy, Castoriadis and RanciereДокумент30 страницTwo Re Foundation Projects of Democracy in Contemporary French Philosophy, Castoriadis and Ranciereradical_imaginaryОценок пока нет
- Pengembangan Daya Saing Umkm Di Malaysia Dan Singapura: Sebuah KomparasiДокумент11 страницPengembangan Daya Saing Umkm Di Malaysia Dan Singapura: Sebuah KomparasiKJA CentreОценок пока нет
- Kiaer Christina Imagine No Possessions The Socialist Objects of Russian ConstructivismДокумент363 страницыKiaer Christina Imagine No Possessions The Socialist Objects of Russian ConstructivismAnalía Capdevila100% (2)
- Listen and and Fill in The Gaps 1-6 With A Correct Sentence A-FДокумент3 страницыListen and and Fill in The Gaps 1-6 With A Correct Sentence A-FSelin DurakОценок пока нет
- Municipal Government of Kalayaan, LagunaДокумент2 страницыMunicipal Government of Kalayaan, LagunaJuan Paolo S. BrosasОценок пока нет
- Admission Application Form - 2021: Chhatrapati Shahu Ji Maharaj University, KanpurДокумент1 страницаAdmission Application Form - 2021: Chhatrapati Shahu Ji Maharaj University, KanpurTrilok GuptaОценок пока нет
- ProgramДокумент48 страницProgramSebastian JimenezОценок пока нет
- Mans Social and Cultural BackgroundДокумент36 страницMans Social and Cultural BackgroundAngeline DiazОценок пока нет
- The Link The Link The Link The Link The Link: AdvisorsДокумент4 страницыThe Link The Link The Link The Link The Link: AdvisorsDebabrata MalickОценок пока нет
- Lozana v. DepakakiboДокумент2 страницыLozana v. DepakakibocassieОценок пока нет
- 5 Pspca Vs CoaДокумент2 страницы5 Pspca Vs Coagianfranco0613Оценок пока нет
- Dypedahl - Snow Falling On Cedars As A Historical (Crime) NovelДокумент17 страницDypedahl - Snow Falling On Cedars As A Historical (Crime) NoveldekonstrukcijaОценок пока нет
- Human Rights Watch ReportДокумент74 страницыHuman Rights Watch ReportSoksan HingОценок пока нет
- Sable Venus She DevilДокумент30 страницSable Venus She DevilMuurish DawnОценок пока нет
- The Anti-Rape Law of 1997 - Philippine E-Legal Forum PDFДокумент7 страницThe Anti-Rape Law of 1997 - Philippine E-Legal Forum PDFPrhylleОценок пока нет
- Third Party Anti-Corruption Compliance CertificationДокумент1 страницаThird Party Anti-Corruption Compliance CertificationEdelmanОценок пока нет
- Franzini Et Al - Extreme Inequalities in Contemporary Capitalism Should We Be Concerned About The Rich (2016)Документ134 страницыFranzini Et Al - Extreme Inequalities in Contemporary Capitalism Should We Be Concerned About The Rich (2016)wolfgang.villarreal2984Оценок пока нет
- 06 The Creation of Wealth V03Документ1 страница06 The Creation of Wealth V03publius_federalistОценок пока нет
- Desiree 3Документ26 страницDesiree 3Arul MuruganОценок пока нет