Вам также может понравиться
- Mukesh Chawla Mukesh ChawlaДокумент62 страницыMukesh Chawla Mukesh Chawlajaideepjd06Оценок пока нет
- Health PolicyДокумент19 страницHealth PolicyBismah Saeed100% (1)
- Evolving Roles of Pharmacists in AMS by Dr. Mediadora SanielДокумент72 страницыEvolving Roles of Pharmacists in AMS by Dr. Mediadora SanielMark Anthony EllanaОценок пока нет
- An Introduction To Evidence-Based NursinДокумент8 страницAn Introduction To Evidence-Based NursinAli MaqsudiОценок пока нет
- Basic of PharmacoeconomicsДокумент34 страницыBasic of Pharmacoeconomicssridwiwulan dariОценок пока нет
- Methods of Pharmacoeconomic AnalysisДокумент19 страницMethods of Pharmacoeconomic AnalysisDoaa BadarnehОценок пока нет
- Chapter 01Документ14 страницChapter 01flaviamarottaОценок пока нет
- Decision Modelling For Health Economic Evaluation Handbooks in Health Economic Evaluation by Andrew Briggs Mark Sculpher Karl Claxton B00m0j1fooДокумент5 страницDecision Modelling For Health Economic Evaluation Handbooks in Health Economic Evaluation by Andrew Briggs Mark Sculpher Karl Claxton B00m0j1fooDeepanshuGupta100% (1)
- Pharmacoeconomicskeytoaffordablemedicines2012 130905064144Документ24 страницыPharmacoeconomicskeytoaffordablemedicines2012 130905064144Tarachand Lalwani100% (1)
- Pharmaco EconomicsДокумент49 страницPharmaco EconomicsSunil100% (1)
- Pharmacoeconomics LceДокумент118 страницPharmacoeconomics LceHope GemidaОценок пока нет
- Chapter 1: Introduction To The Concept of Drug Information: Learning ObjectivesДокумент17 страницChapter 1: Introduction To The Concept of Drug Information: Learning Objectiveskola belloОценок пока нет
- Minimum Standard For Hospital PharmacyДокумент15 страницMinimum Standard For Hospital PharmacyHaseeba Khan100% (2)
- Doing Health Policy AnalysisДокумент10 страницDoing Health Policy AnalysisPhan Uyen100% (1)
- Health Care Workers Motivation and Retention Approaches of Health Workersin Ethiopia A Scoping ReviewДокумент7 страницHealth Care Workers Motivation and Retention Approaches of Health Workersin Ethiopia A Scoping ReviewBSIT2C-REYES, ChristianОценок пока нет
- 4-Demand For HealthcareДокумент24 страницы4-Demand For HealthcareVaishali UzzielОценок пока нет
- Guidelines For The Medicines and Therapeutics CommitteeДокумент20 страницGuidelines For The Medicines and Therapeutics CommitteeLorezza Miranda Aguilar100% (1)
- HiAP PowerpointДокумент21 страницаHiAP Powerpointjaypee pengОценок пока нет
- Characteristics of Health Service SettingsДокумент24 страницыCharacteristics of Health Service SettingsOladipupo Joseph100% (1)
- Knowing What You Get For What You Pay: An Introduction To Cost EffectivenessДокумент30 страницKnowing What You Get For What You Pay: An Introduction To Cost EffectivenessGirish GopalakrishnanОценок пока нет
- PharmacoeconomicsДокумент10 страницPharmacoeconomicsKarl Ian Maliwat100% (1)
- Foundation Issues: Pharmacoeconomics: Principles, Methods, and ApplicationsДокумент16 страницFoundation Issues: Pharmacoeconomics: Principles, Methods, and ApplicationsbencleeseОценок пока нет
- PHME311 Week 3 Day 1 Module 7 Promotions Mix Decisions and StrategiesДокумент58 страницPHME311 Week 3 Day 1 Module 7 Promotions Mix Decisions and StrategiesJoemelyn SapitanОценок пока нет
- 2 PTCДокумент73 страницы2 PTCसन्दिप क्षेत्रीОценок пока нет
- Pareto Analysis of Total Quality ManagementДокумент18 страницPareto Analysis of Total Quality ManagementankitatiwarigОценок пока нет
- INSPolicyNotePharmaceutical PDFДокумент10 страницINSPolicyNotePharmaceutical PDFAna AsmaraОценок пока нет
- Multidisciplinary Healthcare PDFДокумент1 страницаMultidisciplinary Healthcare PDFRizza MascariñasОценок пока нет
- Introduction To Health EconomicsДокумент50 страницIntroduction To Health Economicsabdlfet rejatoОценок пока нет
- 3 Demand and Supply For Health CareДокумент76 страниц3 Demand and Supply For Health Carebereket gashu0% (1)
- Good Naming, Labeling, and Packaging Practices To Reduce Medication ErrorsДокумент23 страницыGood Naming, Labeling, and Packaging Practices To Reduce Medication ErrorssekahaОценок пока нет
- Exploratory Study of Self-Medication Practices Among StudentsДокумент5 страницExploratory Study of Self-Medication Practices Among StudentsN SОценок пока нет
- (PDF) Indicators of Hospital Performance Evaluation - A Systematic ReviewДокумент20 страниц(PDF) Indicators of Hospital Performance Evaluation - A Systematic ReviewFari ZafarОценок пока нет
- Organization of Hospital PharmacyДокумент27 страницOrganization of Hospital PharmacyMisty CheifОценок пока нет
- Scope of Tele-Pharmacists in A Pandemic PDFДокумент7 страницScope of Tele-Pharmacists in A Pandemic PDFjahangirОценок пока нет
- Milestones Health Promotion 05022010Документ42 страницыMilestones Health Promotion 05022010Claire Cassar100% (1)
- Chapter 38. Medication Reconciliation: BackgroundДокумент14 страницChapter 38. Medication Reconciliation: BackgroundnurhaidahОценок пока нет
- Administrative Order NoДокумент16 страницAdministrative Order NoNikkaMontilОценок пока нет
- Clinical ResearchДокумент5 страницClinical ResearchDeepti ShrivasОценок пока нет
- 0555 - Healthcare Risk Assessment Made Easy PDFДокумент16 страниц0555 - Healthcare Risk Assessment Made Easy PDFCecilia YeniОценок пока нет
- Hospital PricingДокумент41 страницаHospital Pricingaarti HingeОценок пока нет
- Pharmaceutical Care: by Musonda .K. Daka Department of Pharmacy School of Health Sciences University of ZambiaДокумент20 страницPharmaceutical Care: by Musonda .K. Daka Department of Pharmacy School of Health Sciences University of ZambiaLuka Mawele SinyangweОценок пока нет
- Introduction To Clinical PharmacyДокумент15 страницIntroduction To Clinical PharmacyNauman ChaudharyОценок пока нет
- Descriptive Epidemiology Study Designs: Zziwa Swaibu (BEH, MPH MUK)Документ47 страницDescriptive Epidemiology Study Designs: Zziwa Swaibu (BEH, MPH MUK)Nina100% (1)
- MT4001 Experimental Design: Monday, 12-3 PM Dr. Ir. Budi Hartono SetiamargaДокумент38 страницMT4001 Experimental Design: Monday, 12-3 PM Dr. Ir. Budi Hartono SetiamargaAndrew CarrОценок пока нет
- Rapid Risk Assessment of Acute Public Health EventsДокумент44 страницыRapid Risk Assessment of Acute Public Health EventsdinahajjarОценок пока нет
- Nurse Orientation - NarcoticsДокумент25 страницNurse Orientation - NarcoticsSalma MustafaОценок пока нет
- Introduction To Public HealthДокумент23 страницыIntroduction To Public HealthNhial Nyachol BolОценок пока нет
- What Is Health EconomicsДокумент8 страницWhat Is Health Economicssoar102Оценок пока нет
- Introduction To Health Economics & Econ Evaluation - HPAd 201Документ76 страницIntroduction To Health Economics & Econ Evaluation - HPAd 201Arianne A ZamoraОценок пока нет
- An Assestment of The Trinidad and Tobago Health Care SystemДокумент4 страницыAn Assestment of The Trinidad and Tobago Health Care SystemMarli MoiseОценок пока нет
- A Gift of Life Deserves Compensation: How To Increase Living Kidney Donation With Realistic Incentives, Cato Policy Analysis No. 604Документ24 страницыA Gift of Life Deserves Compensation: How To Increase Living Kidney Donation With Realistic Incentives, Cato Policy Analysis No. 604Cato Institute100% (1)
- Resuscitation Team ConceptДокумент7 страницResuscitation Team ConceptArun GeorgeОценок пока нет
- Patient Record MaintenanceДокумент2 страницыPatient Record MaintenanceSai SridharОценок пока нет
- Drug Utilization ReviewsДокумент7 страницDrug Utilization ReviewsenoyОценок пока нет
- Msc-Medication Administration PolicyДокумент42 страницыMsc-Medication Administration PolicyMarianne Laylo100% (1)
- Antimicrobial Prescribing PolicyДокумент20 страницAntimicrobial Prescribing PolicycraОценок пока нет
- Proper Disposal of Expired or Unwanted DrugsДокумент9 страницProper Disposal of Expired or Unwanted Drugscarramrod2Оценок пока нет
- Economics Evaluation: Faculty of Public Health, University of Muhammadiyah Jakarta Ridhwan Fauzi, MPH 08121914211Документ31 страницаEconomics Evaluation: Faculty of Public Health, University of Muhammadiyah Jakarta Ridhwan Fauzi, MPH 08121914211synyster92xОценок пока нет
- Pharmacoeconomics: Health vs. Cost: Netra RisalДокумент3 страницыPharmacoeconomics: Health vs. Cost: Netra RisalNetra RisalОценок пока нет
- Parmacoecnomics 2Документ43 страницыParmacoecnomics 2Aina ButtОценок пока нет
- There Is More To Military Medicine Than Combat Medical SupportДокумент2 страницыThere Is More To Military Medicine Than Combat Medical SupportOzkar ZaldivarОценок пока нет
- Key Indicators PhilippinesДокумент11 страницKey Indicators PhilippinesOzkar ZaldivarОценок пока нет
- Case-OperationsStrategy - Lasik Vision CorpДокумент2 страницыCase-OperationsStrategy - Lasik Vision CorpOzkar Zaldivar100% (2)
- Soldier Medical Readiness Campaign Version - 1.2Документ40 страницSoldier Medical Readiness Campaign Version - 1.2Ozkar ZaldivarОценок пока нет
- RA 10918 Philippine Pharmacy Act of 2016Документ36 страницRA 10918 Philippine Pharmacy Act of 2016Ozkar ZaldivarОценок пока нет
- Cls Student PDFДокумент137 страницCls Student PDFOzkar ZaldivarОценок пока нет
- S7b - Readings - Government Intervention in The MarketДокумент4 страницыS7b - Readings - Government Intervention in The MarketOzkar Zaldivar100% (1)
- Mine Gases (Part 1)Документ15 страницMine Gases (Part 1)Melford LapnawanОценок пока нет
- Juniper M5 M10 DatasheetДокумент6 страницJuniper M5 M10 DatasheetMohammed Ali ZainОценок пока нет
- Motion To DismissДокумент24 страницыMotion To DismisssandyemerОценок пока нет
- Man 3Документ38 страницMan 3Paylo KatolykОценок пока нет
- Revised Estimate Draft 24-12-2021Документ100 страницRevised Estimate Draft 24-12-2021Reenu CherianОценок пока нет
- Multicomponent Distillation Shortcut MethodДокумент5 страницMulticomponent Distillation Shortcut MethodDiegoAndréVegaDávalosОценок пока нет
- GTT NO96 LNG TanksДокумент5 страницGTT NO96 LNG TanksEdutamОценок пока нет
- JQuery Interview Questions and AnswersДокумент5 страницJQuery Interview Questions and AnswersShailesh M SassОценок пока нет
- Water Cooled Centrifugal Chiller (150-3000RT)Документ49 страницWater Cooled Centrifugal Chiller (150-3000RT)remigius yudhiОценок пока нет
- Blockchain Unit Wise Question BankДокумент3 страницыBlockchain Unit Wise Question BankMeghana50% (4)
- Emancipation Fact SheetДокумент2 страницыEmancipation Fact SheetKeelie SmithОценок пока нет
- Centurion Bank of PunjabДокумент7 страницCenturion Bank of Punjabbaggamraasi1234Оценок пока нет
- Job Description: Extensive ReadingДокумент12 страницJob Description: Extensive ReadingNatalia VivonaОценок пока нет
- Malinta - Malolos Via Mcarthur Hi-Way: Jeep Bus Time Schedule & Line MapДокумент6 страницMalinta - Malolos Via Mcarthur Hi-Way: Jeep Bus Time Schedule & Line MapMitchie CimorelliОценок пока нет
- Andaman & Nicobar: Port BlairДокумент4 страницыAndaman & Nicobar: Port BlairDevan BhallaОценок пока нет
- Chapter IДокумент38 страницChapter ITuyền PhạmОценок пока нет
- Lich King Chorus PDFДокумент21 страницаLich King Chorus PDFMacgy YeungОценок пока нет
- List of Approved Journals For Promoting Purposes at The University of JordanДокумент3 страницыList of Approved Journals For Promoting Purposes at The University of JordanZaid MarwanОценок пока нет
- Fashion Designing Sample Question Paper1Документ3 страницыFashion Designing Sample Question Paper1Aditi VermaОценок пока нет
- Water Quality Management For Production of Freshwater Ornamental SHДокумент14 страницWater Quality Management For Production of Freshwater Ornamental SHVarun KОценок пока нет
- Telemeter-Electronic Brochure Flexible Heaters WebДокумент12 страницTelemeter-Electronic Brochure Flexible Heaters WebXavierОценок пока нет
- JKR SPJ 1988 Standard Specification of Road Works - Section 1 - GeneralДокумент270 страницJKR SPJ 1988 Standard Specification of Road Works - Section 1 - GeneralYamie Rozman100% (1)
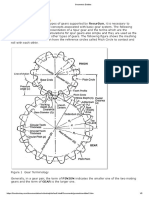
- Geometric Entities: Basic Gear TerminologyДокумент5 страницGeometric Entities: Basic Gear TerminologyMatija RepincОценок пока нет
- PCIB Vs ESCOLIN (G.R. No. L-27860 & L-27896)Документ61 страницаPCIB Vs ESCOLIN (G.R. No. L-27860 & L-27896)strgrlОценок пока нет
- Nelson/Salmo Pennywise March 15, 2016Документ48 страницNelson/Salmo Pennywise March 15, 2016Pennywise PublishingОценок пока нет
- Stps 20 H 100 CTДокумент8 страницStps 20 H 100 CTPablo Cruz ArchundiaОценок пока нет
- PLLV Client Consent FormДокумент4 страницыPLLV Client Consent Formapi-237715517Оценок пока нет
- Media ReportДокумент46 страницMedia ReportAndrew AB BurgoonОценок пока нет
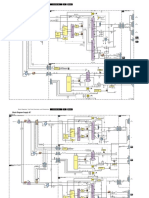
- Philips Chassis Lc4.31e Aa Power Dps 181 PDFДокумент9 страницPhilips Chassis Lc4.31e Aa Power Dps 181 PDFAouadi AbdellazizОценок пока нет
- Lecture Notes (Financial Economics)Документ136 страницLecture Notes (Financial Economics)americus_smile7474100% (2)