Вам также может понравиться
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Peter Attia Measuring Cardiovascular Disease Risk and The Importance of ApoBДокумент14 страницPeter Attia Measuring Cardiovascular Disease Risk and The Importance of ApoBabhimanyu50% (2)
- Medical Surgical Nursing CompilationДокумент17 страницMedical Surgical Nursing CompilationLevi Rae CLerigo EstiponaОценок пока нет
- BMLE SecretsДокумент224 страницыBMLE SecretsAli Al.Juffairi75% (4)
- Aortic Valve DiseaseДокумент63 страницыAortic Valve DiseaseFaridOrahaОценок пока нет
- 2020 International Society of Hypertension Global Hypertension Practice GuidelinesДокумент48 страниц2020 International Society of Hypertension Global Hypertension Practice GuidelinesNicoleta Popa-FoteaОценок пока нет
- Mego Afek Medical CatalogДокумент24 страницыMego Afek Medical CatalogPedro KleinОценок пока нет
- Sinus Node Dysfunction: Anatomy, Physiology, Pathophysiology, and DiagnosisДокумент11 страницSinus Node Dysfunction: Anatomy, Physiology, Pathophysiology, and DiagnosisVasishta Nadella100% (1)
- Evidence-Based Review and Consensus Statement On Monitoring of Hemodynamics and Oxygen Transport BalanceДокумент61 страницаEvidence-Based Review and Consensus Statement On Monitoring of Hemodynamics and Oxygen Transport Balancesusanita1974Оценок пока нет
- Nursing Care Plan Myocardia InfarctionДокумент3 страницыNursing Care Plan Myocardia Infarctionaldrin1920Оценок пока нет
- Jurnal PPT Sindrom BrugadaДокумент64 страницыJurnal PPT Sindrom Brugadasoraya olyfiaОценок пока нет
- Xper Information Management: Quick Reference Guide - Arterial TreesДокумент11 страницXper Information Management: Quick Reference Guide - Arterial TreeswiwingОценок пока нет
- Central Venous Catheterization: Maret 2021Документ39 страницCentral Venous Catheterization: Maret 2021Rudy SiahaanОценок пока нет
- Kalibrasi Alkes Dan TimbangaДокумент27 страницKalibrasi Alkes Dan Timbangavica_ilmiОценок пока нет
- .Pulse Oximetry..)Документ7 страниц.Pulse Oximetry..)Kristzel Peralta FerrerОценок пока нет
- Auscultation of Pediatric Heart MurmursДокумент14 страницAuscultation of Pediatric Heart MurmursBasofi Ashari MappakayaОценок пока нет
- Physical Examination of Cardiovascular SystДокумент13 страницPhysical Examination of Cardiovascular Systgamal attamОценок пока нет
- Assessment of CardiomyopathyДокумент75 страницAssessment of CardiomyopathyMaria GarabajiuОценок пока нет
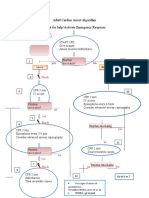
- Adult Cardiac Arrest Treatment AlgorithmДокумент1 страницаAdult Cardiac Arrest Treatment AlgorithmICU RSBMОценок пока нет
- Reflective Writing 4Документ2 страницыReflective Writing 4Luiza NiyazmetovaОценок пока нет
- The Influence of Anesthesia On Cardiac RepolarizationДокумент13 страницThe Influence of Anesthesia On Cardiac Repolarizationzuraini_mdnoorОценок пока нет
- RAD RLE MCN 9 Case StudyДокумент9 страницRAD RLE MCN 9 Case StudyCathleen Nasis ForrosueloОценок пока нет
- Arteriovenous FistulaДокумент11 страницArteriovenous FistulaAbby GuiritanОценок пока нет
- Heart EssayДокумент4 страницыHeart EssayQammar AhmedОценок пока нет
- Bifascicular Block Revealing Steinerts Myotonic DystrophyДокумент8 страницBifascicular Block Revealing Steinerts Myotonic DystrophyIJAR JOURNALОценок пока нет
- Icf KardiorespirasiДокумент8 страницIcf KardiorespirasiTahu BulatОценок пока нет
- Cardiogenic ShockДокумент3 страницыCardiogenic Shockmerin sunilОценок пока нет
- NSTEMIДокумент22 страницыNSTEMImadeputraОценок пока нет
- DO S09 User ManualДокумент10 страницDO S09 User Manualserhan gençerОценок пока нет
- Sympatholytic DrugsДокумент8 страницSympatholytic DrugsJianne CaloОценок пока нет
- Anatomy Review Blood Vessel PDFДокумент6 страницAnatomy Review Blood Vessel PDFAngeliki HoОценок пока нет