Вам также может понравиться
- Cardiology An Introduction: 12 Cardiomyopathy With Joseph S. Alpert, M.DДокумент36 страницCardiology An Introduction: 12 Cardiomyopathy With Joseph S. Alpert, M.DpasambalyrradjohndarОценок пока нет
- Loop Diuretics: Producers of The Greatest Diuresis With Rhonda LawesДокумент23 страницыLoop Diuretics: Producers of The Greatest Diuresis With Rhonda LawespasambalyrradjohndarОценок пока нет
- (PHA) 2.13 Immunopharmacology - Dr. Marbella PDFДокумент10 страниц(PHA) 2.13 Immunopharmacology - Dr. Marbella PDFpasambalyrradjohndarОценок пока нет
- Application For Academic RecordДокумент1 страницаApplication For Academic RecordpasambalyrradjohndarОценок пока нет
- Cardiac Cycle: With Thad WilsonДокумент25 страницCardiac Cycle: With Thad WilsonpasambalyrradjohndarОценок пока нет
- Monthly Blood Glucose Diary PDFДокумент1 страницаMonthly Blood Glucose Diary PDFpasambalyrradjohndarОценок пока нет
- (CLINPATH) 2.02 Transfusion II - Dr.-VillamayorДокумент7 страниц(CLINPATH) 2.02 Transfusion II - Dr.-VillamayorpasambalyrradjohndarОценок пока нет
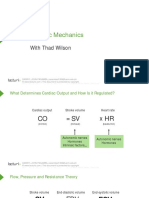
- Cardiac Mechanics: With Thad WilsonДокумент26 страницCardiac Mechanics: With Thad WilsonpasambalyrradjohndarОценок пока нет
- Psych Osce Reviewer 1Документ10 страницPsych Osce Reviewer 1pasambalyrradjohndarОценок пока нет
- Psych Osce Reviewer 1Документ10 страницPsych Osce Reviewer 1pasambalyrradjohndarОценок пока нет
- 8 Part Eye Exam RevisedДокумент17 страниц8 Part Eye Exam RevisedpasambalyrradjohndarОценок пока нет
- Promissory NoteДокумент1 страницаPromissory NotepasambalyrradjohndarОценок пока нет
- 8 Part Eye Exam RevisedДокумент17 страниц8 Part Eye Exam RevisedpasambalyrradjohndarОценок пока нет
- A Cross-Sectional Study On The Association Between Screen Time Exposure and Concentration Among Undergraduate University Students of UermmmciДокумент3 страницыA Cross-Sectional Study On The Association Between Screen Time Exposure and Concentration Among Undergraduate University Students of UermmmcipasambalyrradjohndarОценок пока нет
- Recording The Medical HistoryДокумент8 страницRecording The Medical HistorypasambalyrradjohndarОценок пока нет
- Amoeba: Cytoplasm (Both in Cyst and Peripheral Chromatin (Both Trophozoite Cyst AmoebaДокумент1 страницаAmoeba: Cytoplasm (Both in Cyst and Peripheral Chromatin (Both Trophozoite Cyst AmoebapasambalyrradjohndarОценок пока нет
- Charcoal Tracing Revised - ResultsДокумент3 страницыCharcoal Tracing Revised - ResultspasambalyrradjohndarОценок пока нет
- Oral Rehydration TherapyДокумент12 страницOral Rehydration TherapypasambalyrradjohndarОценок пока нет
- PATHO 1.01a Cellular Response To Stress and Toxic Insults Part I - YanezДокумент8 страницPATHO 1.01a Cellular Response To Stress and Toxic Insults Part I - Yanezpasambalyrradjohndar100% (1)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Free Radicals and The SkinДокумент5 страницFree Radicals and The SkinTamina PfeifferОценок пока нет
- Kalish GI ProtocolsДокумент5 страницKalish GI Protocolsgoosenl100% (1)
- Daily Lesson Log Senior High School: I. ObjectivesДокумент3 страницыDaily Lesson Log Senior High School: I. ObjectivesAl-John EspejoОценок пока нет
- Human Papilloma VirusДокумент3 страницыHuman Papilloma Virusxwendnla russiaОценок пока нет
- Relation of Fruit Flower and SeedsДокумент1 страницаRelation of Fruit Flower and SeedsJoylass P. CarbungcoОценок пока нет
- Biology Chapter 2 Notes (Grade 11)Документ5 страницBiology Chapter 2 Notes (Grade 11)Tammy Lam100% (6)
- The Emergence and Promise of Single-Cell Temporal-Omics ApproachesДокумент9 страницThe Emergence and Promise of Single-Cell Temporal-Omics ApproachesFrancisco Javier BaculimaОценок пока нет
- DNA Fingerprinting - Bio-RadДокумент102 страницыDNA Fingerprinting - Bio-Radebujak100% (3)
- Life Science Previous Paper 2017 DecДокумент38 страницLife Science Previous Paper 2017 DecShilpi PriyaОценок пока нет
- Netters Essential Histology With Student Consult Access 2nd Edition Ovalle Test BankДокумент35 страницNetters Essential Histology With Student Consult Access 2nd Edition Ovalle Test Bankjacobnigordon100% (14)
- NanoCellect Biomedical Begins Distribution To EuropeДокумент2 страницыNanoCellect Biomedical Begins Distribution To EuropePR.comОценок пока нет
- Swot Analysis MabДокумент4 страницыSwot Analysis MabparasmanishaОценок пока нет
- (Plant Science Research and Practices) White, Monica-Rapeseed - Chemical Composition, Production and Health Benefits-Nova Science Publishers (2016)Документ177 страниц(Plant Science Research and Practices) White, Monica-Rapeseed - Chemical Composition, Production and Health Benefits-Nova Science Publishers (2016)Red Red100% (1)
- NCM 112-Care of Clients With Problems in Cellular AberrationsДокумент45 страницNCM 112-Care of Clients With Problems in Cellular AberrationsClaraОценок пока нет
- Bio2 Test 3Документ16 страницBio2 Test 3Carrie NortonОценок пока нет
- List of Video Lectures Available in Our Video BankДокумент25 страницList of Video Lectures Available in Our Video Bankzeeshannajeeb80% (10)
- Ecology Canadian 4th Edition Molles Test Bank 1Документ10 страницEcology Canadian 4th Edition Molles Test Bank 1joseph100% (36)
- ROSELA, ERLAINE MARIE Blood-LabДокумент4 страницыROSELA, ERLAINE MARIE Blood-LabPadoОценок пока нет
- Answers To Chapter 5: (In-Text & Asterisked Problems)Документ10 страницAnswers To Chapter 5: (In-Text & Asterisked Problems)平野健太朗Оценок пока нет
- DNA Profiling: DNA Profiling (Also Called DNA Fingerprinting, DNA Testing, or DNA Typing) IsДокумент3 страницыDNA Profiling: DNA Profiling (Also Called DNA Fingerprinting, DNA Testing, or DNA Typing) IsShaik MoqtiyarОценок пока нет
- Kuliah-6 Pemurnian Enzim TranslateДокумент77 страницKuliah-6 Pemurnian Enzim Translatesyifa nurul ainiОценок пока нет
- Importanceof CarbohydratesДокумент3 страницыImportanceof CarbohydratescraigОценок пока нет
- Phenetic Approaches To Classification: Academy of Natural Sciences, Philadelphia, Pennsylvania 19103Документ8 страницPhenetic Approaches To Classification: Academy of Natural Sciences, Philadelphia, Pennsylvania 19103Trang PhamОценок пока нет
- MUHC News LetterДокумент16 страницMUHC News LetterLouiseWorrallОценок пока нет
- Phylogenetic TreesДокумент11 страницPhylogenetic TreesManisha BishtОценок пока нет
- CAP Checklist 110718Документ53 страницыCAP Checklist 110718yousrazeidan1979Оценок пока нет
- Biochemistry Vol 2 David E. MetzlerДокумент1 040 страницBiochemistry Vol 2 David E. Metzlerysmnsnmz100% (2)
- Cornell University: Dairy Foods Science NotesДокумент2 страницыCornell University: Dairy Foods Science NotesTanishka AggarwalОценок пока нет
- Blueprint For The Provision of Comprehensive Care For Trans Persons and Their Communities in The Caribbean and Other Anglophone CountriesДокумент88 страницBlueprint For The Provision of Comprehensive Care For Trans Persons and Their Communities in The Caribbean and Other Anglophone CountriesTRANScending BordersОценок пока нет
- MergedДокумент427 страницMergedNishit kumar100% (1)