Вам также может понравиться
- Cultural Competency Skills for Psychologists, Psychotherapists, and Counselling Professionals: A Workbook for Caring Across CulturesОт EverandCultural Competency Skills for Psychologists, Psychotherapists, and Counselling Professionals: A Workbook for Caring Across CulturesОценок пока нет
- Advantages of MultilingualismДокумент6 страницAdvantages of MultilingualismanglicusОценок пока нет
- The Role of Language in Therapy - How Bilingual - Multilingual TherДокумент107 страницThe Role of Language in Therapy - How Bilingual - Multilingual Thermelpomena81Оценок пока нет
- Rosenberg Et Al - Through Interpreters' Eyes, Comparing Roles of Professional and Family InterpretersДокумент7 страницRosenberg Et Al - Through Interpreters' Eyes, Comparing Roles of Professional and Family InterpretersMaria AguilarОценок пока нет
- Research Paper Final DraftДокумент19 страницResearch Paper Final Draftapi-532628235Оценок пока нет
- The Role of Clinical SupervisionДокумент7 страницThe Role of Clinical Supervisionsethiee100% (1)
- The Role of Language in DermatologyДокумент2 страницыThe Role of Language in DermatologyEnglish VoiceОценок пока нет
- Migrants Perceptions of Using InterpretersДокумент10 страницMigrants Perceptions of Using Interpretersapi-242029870Оценок пока нет
- Physician-Patient Communication 2018Документ12 страницPhysician-Patient Communication 2018danielefranceschiОценок пока нет
- Multicultural Article Summary CritiqueДокумент2 страницыMulticultural Article Summary Critiqueapi-617357782Оценок пока нет
- Martinez Be RelevantДокумент12 страницMartinez Be RelevantDiane Veronica Taylor MoreauОценок пока нет
- CRITIC Jurnal PsycolinguisticДокумент4 страницыCRITIC Jurnal PsycolinguisticDimas HarilukitoОценок пока нет
- Why Bilingualism: The Role of Joint Activation and Executive Function in The BrainДокумент36 страницWhy Bilingualism: The Role of Joint Activation and Executive Function in The Brainapi-548705046Оценок пока нет
- How Do Medical Specialists Value Their Own Intercultural Communication Behaviour? A Reflective Practice StudyДокумент9 страницHow Do Medical Specialists Value Their Own Intercultural Communication Behaviour? A Reflective Practice StudyHarrison PonceОценок пока нет
- Julia Article EappДокумент13 страницJulia Article EappGwyneth LabaoОценок пока нет
- Beyond English Only - Addressing Language Interpretation in ProfesДокумент26 страницBeyond English Only - Addressing Language Interpretation in ProfesAnna BellОценок пока нет
- Advertising To Bilinguals: Does The Language of Advertising Influence The Nature of Thoughts?Документ16 страницAdvertising To Bilinguals: Does The Language of Advertising Influence The Nature of Thoughts?alfareasОценок пока нет
- Understanding The Unsaid Enhancing MulticulturalДокумент15 страницUnderstanding The Unsaid Enhancing Multiculturalmunnie0906_109606846Оценок пока нет
- In Brief (Summer 11) AphasiaДокумент1 страницаIn Brief (Summer 11) AphasiaSpeech & Language Therapy in PracticeОценок пока нет
- BAS Conference 2007Документ5 страницBAS Conference 2007Speech & Language Therapy in PracticeОценок пока нет
- 2006 Debruin y BrugmansДокумент9 страниц2006 Debruin y BrugmansLucila S. RolfoОценок пока нет
- Historical Trends in Humanistic TherapiesДокумент4 страницыHistorical Trends in Humanistic Therapiestithi royОценок пока нет
- Cross-Cultural Analysis of Language in The Assessment of Personality VariablesДокумент121 страницаCross-Cultural Analysis of Language in The Assessment of Personality Variablescoconut108Оценок пока нет
- Nonverbal Communication For The Enhancement of Foreign Language Professional Competency in Medical Students: A StudyДокумент15 страницNonverbal Communication For The Enhancement of Foreign Language Professional Competency in Medical Students: A Study19041425 Phạm Thị Thanh HuyềnОценок пока нет
- Caring in English: ESP For Nurses: August 2013Документ11 страницCaring in English: ESP For Nurses: August 2013Serendipity EnglishОценок пока нет
- Mitigating Language and Cultural Barriers in Healthcare - Toward A Holistic ApproachДокумент5 страницMitigating Language and Cultural Barriers in Healthcare - Toward A Holistic ApproachY FernandezОценок пока нет
- Thepsychologist 0307asy4Документ3 страницыThepsychologist 0307asy4serendipitykbjcОценок пока нет
- Mitigating Language and Cultural BarrierДокумент5 страницMitigating Language and Cultural BarrierIva StojčićОценок пока нет
- Non Verbal and PsychotherapyДокумент15 страницNon Verbal and PsychotherapyApplied Psych23Оценок пока нет
- Foundations of Multicultural Psychology Intro SampleДокумент16 страницFoundations of Multicultural Psychology Intro SampleGlory Mae ProllesОценок пока нет
- Addressing Language and Culture Differences in Health Care Settings 2 PDFДокумент4 страницыAddressing Language and Culture Differences in Health Care Settings 2 PDFWandi HuseinОценок пока нет
- The Interpreter As Institutional Gatekeeper: The Social-Linguistic Role of Interpreters in Spanish-English Medical DiscourseДокумент24 страницыThe Interpreter As Institutional Gatekeeper: The Social-Linguistic Role of Interpreters in Spanish-English Medical DiscourseFiammetta AnzevinoОценок пока нет
- English Medical TranslationДокумент11 страницEnglish Medical Translationlixiaoxiu100% (1)
- Effective Psychotherapy in A Racially and Culturally Diverse Society - Bhui & N MorganДокумент8 страницEffective Psychotherapy in A Racially and Culturally Diverse Society - Bhui & N MorgancaveolemuresОценок пока нет
- Therapeutic Communication: Esmeralda Sherko, Eugjen Sotiri, Erinda LikaДокумент10 страницTherapeutic Communication: Esmeralda Sherko, Eugjen Sotiri, Erinda LikaChucky VergaraОценок пока нет
- Large-Scale Analysis of Counseling Conversations: An Application of Natural Language Processing To Mental HealthДокумент14 страницLarge-Scale Analysis of Counseling Conversations: An Application of Natural Language Processing To Mental HealthgovindmanianОценок пока нет
- ACFrOgA1xCZYLiNrpcCuDbnjLc0jxOlBGItE5MposOqdkNegglqWuP5GQCa2 CBAe1it F58tMAJMA9CG81 BOzVp73qAiiSQ7OhdQs6cWG0Tj83fENHiWROyTYCVyDcGkQVF-1eldlfBHZmq235Документ10 страницACFrOgA1xCZYLiNrpcCuDbnjLc0jxOlBGItE5MposOqdkNegglqWuP5GQCa2 CBAe1it F58tMAJMA9CG81 BOzVp73qAiiSQ7OhdQs6cWG0Tj83fENHiWROyTYCVyDcGkQVF-1eldlfBHZmq235MARIA ELENA ELIZONDO DE LA GARZAОценок пока нет
- Beyond Basic Communication: The Role of The Mother Tongue in Cognitive-Behavioral Therapy (CBT)Документ12 страницBeyond Basic Communication: The Role of The Mother Tongue in Cognitive-Behavioral Therapy (CBT)abrhamОценок пока нет
- Transformation of Professional Identity - An Exploration of Psychologists and Psychiatrists Implementing Open Dialogue - GRIFADOДокумент22 страницыTransformation of Professional Identity - An Exploration of Psychologists and Psychiatrists Implementing Open Dialogue - GRIFADOmariana puchivailoОценок пока нет
- Dissertation Sur La StigmatisationДокумент5 страницDissertation Sur La StigmatisationHowToWriteMyPaperLittleRock100% (1)
- Intensive Care NursesДокумент15 страницIntensive Care NursesUlysses GamayonОценок пока нет
- Literature Review On Speech TherapyДокумент8 страницLiterature Review On Speech Therapyfihum1hadej2100% (1)
- JABADAO - Making A Song and Dance About Communication.Документ3 страницыJABADAO - Making A Song and Dance About Communication.Speech & Language Therapy in PracticeОценок пока нет
- InterpreterДокумент12 страницInterpreterXinyue XuОценок пока нет
- Caring in English: ESP For Nurses: August 2013Документ11 страницCaring in English: ESP For Nurses: August 2013Al DobbОценок пока нет
- The Scope of Clinical LinguisticsДокумент228 страницThe Scope of Clinical LinguisticsMeet UlixisОценок пока нет
- Research Paper Topics On BilingualismДокумент4 страницыResearch Paper Topics On Bilingualismisvgmchkf100% (1)
- Of (Or of (Or of or Four ofДокумент5 страницOf (Or of (Or of or Four ofFrancis SmithОценок пока нет
- CrujjjjjДокумент8 страницCrujjjjjAlexander QuemadaОценок пока нет
- The Significance of Communication and Care in One's Mother Tongue: Patients' ViewsДокумент12 страницThe Significance of Communication and Care in One's Mother Tongue: Patients' ViewsJohn Earl SetiasОценок пока нет
- Impact of Language Proficiency On Mental Health Service Use - Treatment andДокумент9 страницImpact of Language Proficiency On Mental Health Service Use - Treatment andRima MuhsenОценок пока нет
- In Brief Winter 11Документ2 страницыIn Brief Winter 11Speech & Language Therapy in PracticeОценок пока нет
- Artikel Language IdeologyДокумент2 страницыArtikel Language Ideologycanakya muhammadОценок пока нет
- Contrastive Analysis On Speech Act, MA Thesis SummaryДокумент13 страницContrastive Analysis On Speech Act, MA Thesis Summaryneed_information100% (3)
- Dissertation On The Effects of Bilingualism On Cognitive Development PDFДокумент26 страницDissertation On The Effects of Bilingualism On Cognitive Development PDFsofianeliver100% (2)
- Psychology of Bilingualism The Cognitive and Emotional World of Bilinguals by Alfredo Ardila, Anna B. Cieślicka, Roberto R. Heredia, Mónica RoselliДокумент318 страницPsychology of Bilingualism The Cognitive and Emotional World of Bilinguals by Alfredo Ardila, Anna B. Cieślicka, Roberto R. Heredia, Mónica RoselliAlessandra Ale100% (1)
- Brain StormingДокумент492 страницыBrain StormingjosephОценок пока нет
- Multi Culture 18Документ12 страницMulti Culture 18ehsaan120Оценок пока нет
- Language Variation Across Pakistan and British Pharmaceutical Text: Critical Discourse AnalysisДокумент11 страницLanguage Variation Across Pakistan and British Pharmaceutical Text: Critical Discourse AnalysisUme LailaОценок пока нет
- 2008 08 AJSLP - Bilingual AphasiaДокумент20 страниц2008 08 AJSLP - Bilingual Aphasiaamy_maguireОценок пока нет
- An American FoucaultДокумент20 страницAn American Foucaultlc49Оценок пока нет
- Derek HookTranscript 1Документ8 страницDerek HookTranscript 1lc49Оценок пока нет
- Pah 2004 6 1 107Документ10 страницPah 2004 6 1 107lc49Оценок пока нет
- Goldwater E First InterviewДокумент3 страницыGoldwater E First Interviewlc49Оценок пока нет
- Resnick PrelimsДокумент21 страницаResnick Prelimslc49Оценок пока нет
- PPA Reading Group - Reading ListДокумент1 страницаPPA Reading Group - Reading Listlc49Оценок пока нет
- Self Cingulate CortexДокумент7 страницSelf Cingulate Cortexlc49Оценок пока нет
- Chapter39 PDFДокумент14 страницChapter39 PDFlc49Оценок пока нет
- Domenico Consenza Body and Language in Eating DisordersДокумент26 страницDomenico Consenza Body and Language in Eating Disorderslc49Оценок пока нет
- Thomas Ogden InterviewДокумент20 страницThomas Ogden Interviewlc49100% (1)
- IPT For DepressionДокумент13 страницIPT For Depressionlc49Оценок пока нет
- Lacan Verso InterviewДокумент10 страницLacan Verso Interviewlc49Оценок пока нет
- Lacan Adaptation WikipediaДокумент3 страницыLacan Adaptation Wikipedialc49Оценок пока нет
- Nikolas Rose - Neurochemical SelvesДокумент15 страницNikolas Rose - Neurochemical Selveslc49Оценок пока нет
- Philip Bromberg InterviewДокумент33 страницыPhilip Bromberg Interviewlc49100% (1)
- Schizoid Bioenergetics PT 2Документ10 страницSchizoid Bioenergetics PT 2lc49Оценок пока нет
- Professional Goals For Practicum 2 0Документ5 страницProfessional Goals For Practicum 2 0api-321657011Оценок пока нет
- Tips On Writing A Thesis StatementДокумент2 страницыTips On Writing A Thesis StatementSheena Rhea GingcoОценок пока нет
- 15 Solomon Melesse Mulu MelesseДокумент9 страниц15 Solomon Melesse Mulu MelesseHaroon Khan DurraniОценок пока нет
- PGNHS OFFICIAL Paper Size A4 Header and Footer For Outgoing CommunicationДокумент10 страницPGNHS OFFICIAL Paper Size A4 Header and Footer For Outgoing CommunicationPunong Grande NHS Banga NHS Annex (R XII - South Cotabato)Оценок пока нет
- Corporate Conflict Management by Rout and OmikoДокумент294 страницыCorporate Conflict Management by Rout and OmikoMr. MeОценок пока нет
- Effective Teaching Techniques StrategiesДокумент14 страницEffective Teaching Techniques StrategiesJAY MIRANDAОценок пока нет
- Jefferson Cereal Box ProjectДокумент2 страницыJefferson Cereal Box ProjectkmanzelliОценок пока нет
- On Etulo IdeophonesДокумент4 страницыOn Etulo IdeophonesIOSRjournalОценок пока нет
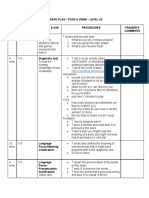
- Lesson Plan - Food & Drink - Level A2 Time Interaction Stage & Aim Procedures Trainer'S Comments Lead-InДокумент4 страницыLesson Plan - Food & Drink - Level A2 Time Interaction Stage & Aim Procedures Trainer'S Comments Lead-InCương Nguyễn DuyОценок пока нет
- The Behavioral Inattention Test For Unilateral Visual NeglectДокумент7 страницThe Behavioral Inattention Test For Unilateral Visual NeglectDharmik PrajapatiОценок пока нет
- Character Education in Adolescence - Rudolf AllersДокумент35 страницCharacter Education in Adolescence - Rudolf AllersJorge Luis Villacís Nieto100% (1)
- NOTESДокумент2 страницыNOTESRobyn Macy MirandaОценок пока нет
- P.E. at Health PresentationДокумент46 страницP.E. at Health PresentationMylene Quilatan Masanga100% (1)
- The Art of ReportingДокумент4 страницыThe Art of ReportingTOPdeskОценок пока нет
- School Improvement Plans, A Tool To Improve The Quality of EducationДокумент12 страницSchool Improvement Plans, A Tool To Improve The Quality of EducationArumugam ManickamОценок пока нет
- Lesson 5 Working Memory Model Ao3Документ20 страницLesson 5 Working Memory Model Ao3Srnt YyoОценок пока нет
- OBE Syllabus AgriFisheryДокумент14 страницOBE Syllabus AgriFisheryMary Ann Austria Gonda-Felipe90% (10)
- Syllabus - GE 9 - Rizal 1Документ4 страницыSyllabus - GE 9 - Rizal 1Roger Yatan Ibañez Jr.Оценок пока нет
- Systematic Review On Sustainable Entrepreneurship Education (SEE) : A Framework and AnalysisДокумент24 страницыSystematic Review On Sustainable Entrepreneurship Education (SEE) : A Framework and AnalysisVatsal Shah100% (1)
- Youth Alive Leadership Training Day 2022Документ2 страницыYouth Alive Leadership Training Day 2022Jemylene LicoОценок пока нет
- Superlative Board Game PDFДокумент2 страницыSuperlative Board Game PDFUzhe ChávezОценок пока нет
- Methods of Research PPT 1Документ35 страницMethods of Research PPT 1Cueshe YeeОценок пока нет
- Tips On Writing Course Goals/Learning Outcomes and Measurable Learning ObjectivesДокумент8 страницTips On Writing Course Goals/Learning Outcomes and Measurable Learning ObjectivesLovely Abia CapalesОценок пока нет
- EC Useful Homophones ListsДокумент5 страницEC Useful Homophones ListsAdriana BrebenelОценок пока нет
- December 11,12,13,14, 2023.Документ6 страницDecember 11,12,13,14, 2023.Rowena Reyes SadiconОценок пока нет
- 8601 Rana ZubairДокумент18 страниц8601 Rana Zubairarifa aizazОценок пока нет
- Summative Assessment AnalysisДокумент5 страницSummative Assessment Analysisapi-282071638Оценок пока нет
- Imitation by James W. Partington, PHD, BCBA-D, Et Al.Документ10 страницImitation by James W. Partington, PHD, BCBA-D, Et Al.autismoneОценок пока нет
- LAC 10 PROPOSAL HRD F 057 Learning and Development DesignДокумент5 страницLAC 10 PROPOSAL HRD F 057 Learning and Development DesignJimwel Gutierrez100% (2)
- Group-1 TGДокумент6 страницGroup-1 TGCristy GallardoОценок пока нет