Вам также может понравиться
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- S35 - Anil Kumar Pandey (J.K. Pathology) Near V Mart, Gandhi Ground, BADAUN243601 9058494498 / 8755328670Документ6 страницS35 - Anil Kumar Pandey (J.K. Pathology) Near V Mart, Gandhi Ground, BADAUN243601 9058494498 / 8755328670Satyabhan SinghОценок пока нет
- WFRP1 - Herbs and Their Uses (Unofficial)Документ10 страницWFRP1 - Herbs and Their Uses (Unofficial)TyCaineОценок пока нет
- Multisystem & Genetic - BoardsДокумент10 страницMultisystem & Genetic - BoardsSoojung NamОценок пока нет
- Quiz Public HealthДокумент26 страницQuiz Public HealthMedShare89% (27)
- SOPs For Laboratory-1 PDFДокумент178 страницSOPs For Laboratory-1 PDFS M50% (2)
- CKDДокумент35 страницCKDNATTAPAT SANGKAKULОценок пока нет
- CKDДокумент35 страницCKDNATTAPAT SANGKAKULОценок пока нет
- Integrated Disease Management in Vegetable CropsДокумент56 страницIntegrated Disease Management in Vegetable CropsSavita Bhoutekar100% (1)
- Skin Infections and InfestationsДокумент37 страницSkin Infections and InfestationsAremu OlatayoОценок пока нет
- Pathogen Environmental Monitoring BookДокумент54 страницыPathogen Environmental Monitoring BookAngga Prasetyo100% (1)
- Pneumonia Teaching PlanДокумент5 страницPneumonia Teaching PlanFhai Escio71% (7)
- Microbiology and Pasteurization of Surimi SeafoodДокумент24 страницыMicrobiology and Pasteurization of Surimi Seafoodbajwa82mnaОценок пока нет
- Indian Childhood CirrhosisДокумент20 страницIndian Childhood Cirrhosissubinj_3100% (4)
- CRT Acute AbdomenДокумент73 страницыCRT Acute AbdomenNATTAPAT SANGKAKUL100% (1)
- 7.pulmonary Embolism An Update ManagementДокумент40 страниц7.pulmonary Embolism An Update ManagementNATTAPAT SANGKAKULОценок пока нет
- ATB Gyne PDFДокумент10 страницATB Gyne PDFNATTAPAT SANGKAKULОценок пока нет
- ATB Gyne PDFДокумент10 страницATB Gyne PDFNATTAPAT SANGKAKULОценок пока нет
- CRT Breast (Complete)Документ70 страницCRT Breast (Complete)NATTAPAT SANGKAKULОценок пока нет
- CVS in PregnancyДокумент47 страницCVS in PregnancyNATTAPAT SANGKAKULОценок пока нет
- CVS in PregnancyДокумент47 страницCVS in PregnancyNATTAPAT SANGKAKULОценок пока нет
- Bacterial: Viral FungalДокумент53 страницыBacterial: Viral FungalNATTAPAT SANGKAKULОценок пока нет
- Bacterial: Viral FungalДокумент53 страницыBacterial: Viral FungalNATTAPAT SANGKAKULОценок пока нет
- Cancer Screening For 5th Medical StudentsДокумент73 страницыCancer Screening For 5th Medical StudentsNATTAPAT SANGKAKULОценок пока нет
- CBD-Guillian BarreДокумент18 страницCBD-Guillian BarreNATTAPAT SANGKAKULОценок пока нет
- CBD Guillian BarreДокумент18 страницCBD Guillian BarreNATTAPAT SANGKAKULОценок пока нет
- Adrenal Insufficiency Guideline 020713Документ35 страницAdrenal Insufficiency Guideline 020713NATTAPAT SANGKAKULОценок пока нет
- Lobal Initiative For Chronic Bstructive Ung Isease: G O L DДокумент14 страницLobal Initiative For Chronic Bstructive Ung Isease: G O L DNATTAPAT SANGKAKULОценок пока нет
- Blood Smear InterpretationДокумент113 страницBlood Smear InterpretationNATTAPAT SANGKAKULОценок пока нет
- Drug StudiesДокумент32 страницыDrug StudiesKelly ChanОценок пока нет
- Amoeba, Flagellates, CiliatesДокумент3 страницыAmoeba, Flagellates, CiliatesRuel Antiola Mateo100% (1)
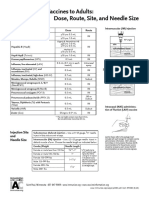
- Administering Vaccines To Adults: Dose, Route, Site, and Needle SizeДокумент1 страницаAdministering Vaccines To Adults: Dose, Route, Site, and Needle SizeAkashОценок пока нет
- Covid-19 (Sars-Cov-2 Rna RT-PCR) : Result: Not Detected Remark: Individual Specimens Reference Range: Not DetectedДокумент2 страницыCovid-19 (Sars-Cov-2 Rna RT-PCR) : Result: Not Detected Remark: Individual Specimens Reference Range: Not DetectedRonni PriceОценок пока нет
- CEFUROXIMEДокумент2 страницыCEFUROXIMEMelvz BallesterosОценок пока нет
- Covid 3Документ5 страницCovid 3api-559328651Оценок пока нет
- Ta Bo LaДокумент65 страницTa Bo LaFina RepitiyanaОценок пока нет
- Price List April 2018Документ7 страницPrice List April 2018nidaОценок пока нет
- Mathematical Modelling of Infectious DiseasesДокумент11 страницMathematical Modelling of Infectious DiseasesBOBBY212Оценок пока нет
- What Is DracunculiasisДокумент1 страницаWhat Is DracunculiasisSiti SyahirahОценок пока нет
- Public Health Approaches To Malaria: Source: National Library of MedicineДокумент24 страницыPublic Health Approaches To Malaria: Source: National Library of MedicineRahmalia Fitri RosaОценок пока нет
- The Diagnosis and Management of Anorectal Disorders PDFДокумент60 страницThe Diagnosis and Management of Anorectal Disorders PDFArizal Abdullah100% (1)
- MDH BrochureДокумент2 страницыMDH Brochurerahms79Оценок пока нет
- Dichiarazione Di Conformita Disinfettanti 18-10-201-2Документ3 страницыDichiarazione Di Conformita Disinfettanti 18-10-201-2Loredana BarbaneagraОценок пока нет
- Guarino 2014Документ21 страницаGuarino 2014ChangОценок пока нет
- MCB 1000L: Applied Microbiology Laboratory ManualДокумент70 страницMCB 1000L: Applied Microbiology Laboratory Manualmahsamoradi100% (1)
- 1a..antimicrobials IntroductionДокумент84 страницы1a..antimicrobials IntroductionAnonymous RlDDdTAsKJОценок пока нет
- ULTRASOUND FEATURES OF FETAL SYNDROMES: Maternal InfectionsДокумент44 страницыULTRASOUND FEATURES OF FETAL SYNDROMES: Maternal InfectionsEasterlilyОценок пока нет
- Prinsip Prinsip SurveilansДокумент30 страницPrinsip Prinsip SurveilansYona TarunaОценок пока нет