Вам также может понравиться
- Pharmacology SlidesДокумент114 страницPharmacology Slidesbrandon15000100% (9)
- NCLEX-RN Exam Prep 2024-2025: 500 NCLEX-RN Test Prep Questions and Answers with ExplanationsОт EverandNCLEX-RN Exam Prep 2024-2025: 500 NCLEX-RN Test Prep Questions and Answers with ExplanationsОценок пока нет
- UWORLDNCLEXreview2021 Watermarked PDFДокумент100 страницUWORLDNCLEXreview2021 Watermarked PDFashley100% (1)
- Pharma 12Документ16 страницPharma 12Mary Roan RonatoОценок пока нет
- Antidiarrheal DrugsДокумент4 страницыAntidiarrheal DrugsNadhirah ZulkifliОценок пока нет
- Drug Outline: Autonomic Nervous System Drug Class Drug OtherДокумент4 страницыDrug Outline: Autonomic Nervous System Drug Class Drug OtherCess Lagera YbanezОценок пока нет
- Pharmacology - Section 23 - Antibiotics 2Документ5 страницPharmacology - Section 23 - Antibiotics 2Pathalee ThalpavilaОценок пока нет
- NCLEX Review: Pharmacology Charlene Natale, BSN, RNДокумент43 страницыNCLEX Review: Pharmacology Charlene Natale, BSN, RNMenly Susada100% (1)
- PharmacologyДокумент3 страницыPharmacologyMohd Afiq AizuddinОценок пока нет
- Cardio Q&aДокумент147 страницCardio Q&aHoney Lyn AlebioОценок пока нет
- Cardiovascular System Drugs - Active Stack® Pharmacology Flash Cards - Study Materials - My ATIДокумент1 страницаCardiovascular System Drugs - Active Stack® Pharmacology Flash Cards - Study Materials - My ATIAntonette Joy SolinapОценок пока нет
- PharmacologyДокумент9 страницPharmacologyRPh Krishna Chandra JagritОценок пока нет
- Cholinergic Pharmacology - Drug TableДокумент2 страницыCholinergic Pharmacology - Drug TableFОценок пока нет
- Pharmacology FirecrackerДокумент37 страницPharmacology FirecrackerRehan Usman100% (1)
- Suffixes and PrefixesДокумент2 страницыSuffixes and PrefixesBeckyОценок пока нет
- Drugs SummaryДокумент23 страницыDrugs Summaryapi-3832811100% (1)
- PharmacyДокумент16 страницPharmacyJow RamosОценок пока нет
- Pharm Phlash PDFДокумент207 страницPharm Phlash PDFAdiShine100% (1)
- Angina Pharmacology YeahДокумент16 страницAngina Pharmacology YeahMuhammad AfifuddinОценок пока нет
- Family Names of DrugsДокумент1 страницаFamily Names of DrugsangelОценок пока нет
- 12 Points To Answering Pharmacology Questions PDFДокумент2 страницы12 Points To Answering Pharmacology Questions PDFbsebi763271Оценок пока нет
- Head and NeckkkkkkДокумент7 страницHead and NeckkkkkkJoey A. RumbaoaОценок пока нет
- Pharm Chapter 2 and 3 Study GuideДокумент10 страницPharm Chapter 2 and 3 Study GuideamkОценок пока нет
- Pharmacodynamics 4Документ28 страницPharmacodynamics 4علي المحترفОценок пока нет
- Pall CareДокумент81 страницаPall Careडा. सत्यदेव त्यागी आर्यОценок пока нет
- Table of Sedative, Hypnotic, AntianxietyДокумент4 страницыTable of Sedative, Hypnotic, AntianxietyirfanzukriОценок пока нет
- Pharmacology Important Things To RememberДокумент5 страницPharmacology Important Things To RememberHydie100% (1)
- Classification of Drugs PDFДокумент15 страницClassification of Drugs PDFmuhammad ihtisham ul hassanОценок пока нет
- Anti-Infective Pharmacology ReviewerДокумент5 страницAnti-Infective Pharmacology ReviewerArianne Pearl PrimeroОценок пока нет
- Antidepressants: Depression Is One The Most Treatable Mental IllnessДокумент40 страницAntidepressants: Depression Is One The Most Treatable Mental IllnessMohammed AbdullahОценок пока нет
- Pharmacology A ReviewДокумент15 страницPharmacology A ReviewKathrynne MendozaОценок пока нет
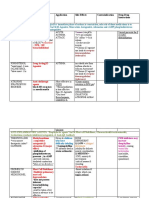
- Drug Name Mechanism Application Side Effects Contraindication Drug-Drug InteractionsДокумент3 страницыDrug Name Mechanism Application Side Effects Contraindication Drug-Drug Interactionsazhar hussinОценок пока нет
- Suffixes and PrefixesДокумент2 страницыSuffixes and PrefixesNiksОценок пока нет
- NCMA216.PHARMA Drugs Acting On The Endocrine SystemДокумент71 страницаNCMA216.PHARMA Drugs Acting On The Endocrine SystemKhams TolentinoОценок пока нет
- Remembering Medication ClassificationsДокумент2 страницыRemembering Medication ClassificationsGVHHОценок пока нет
- Printed Material Module 7 Gastrointestinal System Drugs - PDFДокумент45 страницPrinted Material Module 7 Gastrointestinal System Drugs - PDFShang MacarayonОценок пока нет
- Pharm 2013Документ13 страницPharm 2013Shae Thomas100% (6)
- Chapter 1 - The Nursing Process and Drug TherapyДокумент3 страницыChapter 1 - The Nursing Process and Drug TherapyHaleyОценок пока нет
- Drugs Used in TuberculosisДокумент27 страницDrugs Used in Tuberculosisapi-3705123Оценок пока нет
- Introduction To Nursing PharmacologyДокумент6 страницIntroduction To Nursing PharmacologyArun Roa DanielОценок пока нет
- Pharm Exam ReviewДокумент13 страницPharm Exam ReviewAshleyОценок пока нет
- GIT DrugsДокумент180 страницGIT DrugsMaria Linevel Balderamos Dalida100% (1)
- Pharmacology Notes #1Документ2 страницыPharmacology Notes #1JUSTINE ALLYSA MAY CASTILLOОценок пока нет
- Medication DilutionДокумент23 страницыMedication DilutionamgdanielaОценок пока нет
- Fluid Overload Student PagesДокумент4 страницыFluid Overload Student PagesJess OswaldОценок пока нет
- Antihypertensive Cheat SheetДокумент2 страницыAntihypertensive Cheat SheetRigley GarmanОценок пока нет
- Pharmacology CNS DrugsДокумент15 страницPharmacology CNS DrugsM Youssif Elkady100% (1)
- Introduction To Cns PharmacologyДокумент66 страницIntroduction To Cns PharmacologyYazan Emad Salem100% (1)
- Common Drugs and AntidotesДокумент2 страницыCommon Drugs and AntidotesreynoldОценок пока нет
- Drug Card Solu-MEDROLДокумент2 страницыDrug Card Solu-MEDROLBenОценок пока нет
- Labs 1.19 ABG AnalysisДокумент1 страницаLabs 1.19 ABG AnalysisMonica GonzalezОценок пока нет
- Antiarrhythmic Drugs Classification (Vaughan Williams)Документ8 страницAntiarrhythmic Drugs Classification (Vaughan Williams)ana100% (1)
- ATI Flash Cards 05, Medications Affecting The Nervous SystemДокумент110 страницATI Flash Cards 05, Medications Affecting The Nervous SystemGiovanni MictilОценок пока нет
- Pharmacology Notes (Chapter 20 and 21)Документ2 страницыPharmacology Notes (Chapter 20 and 21)graycorypОценок пока нет
- Drug KenalogДокумент1 страницаDrug KenalogSrkocherОценок пока нет
- Northern Ireland Management of Infection Guidelines For Primary and Community Care 2016Документ48 страницNorthern Ireland Management of Infection Guidelines For Primary and Community Care 2016dreneavalentinstefanОценок пока нет
- Pain Med ChartsДокумент4 страницыPain Med ChartsNursingSchoolNotesОценок пока нет
- Drug Names - Stems, Prefixes, Roots and Suffixes - NCLEX MasteryДокумент5 страницDrug Names - Stems, Prefixes, Roots and Suffixes - NCLEX MasteryMarcel YoungОценок пока нет
- Antiinfectives Drug TableДокумент5 страницAntiinfectives Drug Tablecdp1587100% (3)
- HANDOUT1Документ6 страницHANDOUT1Mark Elben TeodoroОценок пока нет
- Or Nursing 2Документ4 страницыOr Nursing 2Mark Elben TeodoroОценок пока нет
- Or NursingДокумент6 страницOr NursingMark Elben TeodoroОценок пока нет
- RN HealsДокумент2 страницыRN HealsMark Elben TeodoroОценок пока нет
- Test Bank For General Organic and Biochemistry An Applied Approach 2nd Edition ArmstrongДокумент15 страницTest Bank For General Organic and Biochemistry An Applied Approach 2nd Edition Armstrongrowancong0f3pОценок пока нет
- DR Erwin Sukandi, SPPD, K-KV BelumДокумент47 страницDR Erwin Sukandi, SPPD, K-KV BelumrajaalfatihОценок пока нет
- Side Effects of Calcium Channel Blockers: R. Patterson RussellДокумент3 страницыSide Effects of Calcium Channel Blockers: R. Patterson RussellLivia GudacОценок пока нет
- 2018.docx Version 1Документ92 страницы2018.docx Version 1Afsal Ur FriendОценок пока нет
- Complications of Thoracic SurgeryДокумент45 страницComplications of Thoracic SurgeryAlin ToaderОценок пока нет
- Nuclear Stress Test Instructions 1Документ2 страницыNuclear Stress Test Instructions 1Maria EdelОценок пока нет
- Guaranteed To Pass: Exam Tidbits in Easy To Digest, Bite Sized MorselsДокумент2 страницыGuaranteed To Pass: Exam Tidbits in Easy To Digest, Bite Sized MorselsAmberОценок пока нет
- Tacrolimus Ointment Is Used To Treat The Symptoms of EczemaДокумент2 страницыTacrolimus Ointment Is Used To Treat The Symptoms of EczemaSharan SahotaОценок пока нет
- Drugs Affecting Blood PressureДокумент54 страницыDrugs Affecting Blood PressureJeremy VivitОценок пока нет
- Cardiac DripsДокумент7 страницCardiac DripsCeara MillasОценок пока нет
- MCQ On Cardiology IДокумент84 страницыMCQ On Cardiology IHarsh Oak50% (2)
- Diltiazem - ProfileДокумент14 страницDiltiazem - Profileumamaheswararao4Оценок пока нет
- Cardiovascular PharmacologyДокумент77 страницCardiovascular PharmacologyDhruva PatelОценок пока нет
- Practice Exam 1 HESIДокумент10 страницPractice Exam 1 HESIdinkinspdd50% (2)
- Online Practice Tests, Live Classes, Tutoring, Study Guides Q&A, Premium Content and MoreДокумент112 страницOnline Practice Tests, Live Classes, Tutoring, Study Guides Q&A, Premium Content and MoreYoAmoNYC100% (2)
- DRUG INDEX CompiledДокумент24 страницыDRUG INDEX Compiledahmad aliОценок пока нет
- New Question for MoH Prometric Exam تمДокумент7 страницNew Question for MoH Prometric Exam تمsundus951100% (1)
- 0905 (1) When Cardiovascular Medications Become ToxinsДокумент20 страниц0905 (1) When Cardiovascular Medications Become ToxinsjojoleroОценок пока нет
- ACLS DrugsДокумент16 страницACLS Drugstostc100% (2)
- Reflective Journal 1Документ3 страницыReflective Journal 1api-380537580Оценок пока нет
- Cardiac Drug FunctionДокумент2 страницыCardiac Drug FunctionShanda Rieder KozickiОценок пока нет
- 2017 Medical Pharmacology Practice Exam 4Документ6 страниц2017 Medical Pharmacology Practice Exam 4Franklin garryОценок пока нет
- MCQs For Prometric Examination PDFДокумент155 страницMCQs For Prometric Examination PDFYacine Tarik AizelОценок пока нет
- Cardiovascular Agent: Prof. Clement Belvis RN, RM, MPHДокумент86 страницCardiovascular Agent: Prof. Clement Belvis RN, RM, MPHEimhie Lee CasiОценок пока нет
- Lesson 1 Cardiac Glycosides, Antianginals, and Antidysrhythmics - AntiarrhythmmicsДокумент40 страницLesson 1 Cardiac Glycosides, Antianginals, and Antidysrhythmics - AntiarrhythmmicsXiamen Magsino NolascoОценок пока нет
- Herbesser StrokeДокумент15 страницHerbesser StrokePrincess MiraОценок пока нет
- Guaranteed To Pass: Exam Tidbits in Easy To Digest, Bite Sized MorselsДокумент2 страницыGuaranteed To Pass: Exam Tidbits in Easy To Digest, Bite Sized MorselsCarl LeeОценок пока нет
- DRUGS Initial StockДокумент163 страницыDRUGS Initial StockdeasyОценок пока нет
- Cardialgia. Chronic Coronary DiseaseДокумент75 страницCardialgia. Chronic Coronary DiseaseВиктория ПашаеваОценок пока нет
- SDL Obat EmergencyДокумент26 страницSDL Obat EmergencyfarhantunichiaОценок пока нет
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)От EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Рейтинг: 3 из 5 звезд3/5 (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionОт EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionРейтинг: 4 из 5 звезд4/5 (404)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОт EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОценок пока нет
- The Age of Magical Overthinking: Notes on Modern IrrationalityОт EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityРейтинг: 4 из 5 звезд4/5 (32)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisОт EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisРейтинг: 4.5 из 5 звезд4.5/5 (42)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDОт EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDРейтинг: 5 из 5 звезд5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeОт EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeРейтинг: 2 из 5 звезд2/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedОт EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedРейтинг: 4.5 из 5 звезд4.5/5 (82)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryОт EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryРейтинг: 4 из 5 звезд4/5 (46)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaОт EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsОт EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsРейтинг: 4 из 5 звезд4/5 (4)
- The Obesity Code: Unlocking the Secrets of Weight LossОт EverandThe Obesity Code: Unlocking the Secrets of Weight LossРейтинг: 4 из 5 звезд4/5 (6)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesОт EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesРейтинг: 4.5 из 5 звезд4.5/5 (1412)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsОт EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsРейтинг: 5 из 5 звезд5/5 (1)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.От EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Рейтинг: 4.5 из 5 звезд4.5/5 (110)
- Why We Die: The New Science of Aging and the Quest for ImmortalityОт EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityРейтинг: 4 из 5 звезд4/5 (5)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsОт EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsРейтинг: 4.5 из 5 звезд4.5/5 (170)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisОт EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisРейтинг: 5 из 5 звезд5/5 (8)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisОт EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisРейтинг: 3.5 из 5 звезд3.5/5 (2)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessОт EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessРейтинг: 4.5 из 5 звезд4.5/5 (328)
- Troubled: A Memoir of Foster Care, Family, and Social ClassОт EverandTroubled: A Memoir of Foster Care, Family, and Social ClassРейтинг: 4.5 из 5 звезд4.5/5 (27)
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingОт EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingРейтинг: 4 из 5 звезд4/5 (1138)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeОт EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeРейтинг: 4.5 из 5 звезд4.5/5 (253)