Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- ScholarshipsДокумент1 страницаScholarshipsBoobesh Venkata RamananОценок пока нет
- Cleaning and Maintaining Your Royal Enfield BulletДокумент7 страницCleaning and Maintaining Your Royal Enfield BulletBoobesh Venkata RamananОценок пока нет
- TitleДокумент10 страницTitleBoobesh Venkata RamananОценок пока нет
- SRM University SRM College of Physiotherapy Bachelor of Physiotherapy (B.P.T) Cri - Worksheet DEPARTMENT: - DATE: FROM - TOДокумент1 страницаSRM University SRM College of Physiotherapy Bachelor of Physiotherapy (B.P.T) Cri - Worksheet DEPARTMENT: - DATE: FROM - TOBoobesh Venkata RamananОценок пока нет
- A Six-Week Trial of Hula Hooping Using A Weighted Hoop - Eff..Документ1 страницаA Six-Week Trial of Hula Hooping Using A Weighted Hoop - Eff..Boobesh Venkata RamananОценок пока нет
- Biomechanicsofanklejoint 130829145732 Phpapp01Документ76 страницBiomechanicsofanklejoint 130829145732 Phpapp01Hagima Adrian-MihaiОценок пока нет
- Abroad Scholorship by GovernmentДокумент14 страницAbroad Scholorship by GovernmentBoobesh Venkata RamananОценок пока нет
- CWT6Документ16 страницCWT6Boobesh Venkata RamananОценок пока нет
- Gaitppt 140919174427 Phpapp01Документ42 страницыGaitppt 140919174427 Phpapp01Boobesh Venkata RamananОценок пока нет
- Minisota PT Instructions Foreign Educated 2015 - tcm21-52856Документ12 страницMinisota PT Instructions Foreign Educated 2015 - tcm21-52856Boobesh Venkata RamananОценок пока нет
- Cryotherapy Treatment ProcedureДокумент6 страницCryotherapy Treatment ProcedureBoobesh Venkata RamananОценок пока нет
- Healthcare Professionals Qualification Requirements (PQR) 2014-1 PDFДокумент123 страницыHealthcare Professionals Qualification Requirements (PQR) 2014-1 PDFnnawaz4Оценок пока нет
- Full Body Exoskeleton For Quadriplegic PatientsДокумент1 страницаFull Body Exoskeleton For Quadriplegic PatientsBoobesh Venkata RamananОценок пока нет
- Buff Dudes 12 Week Home and Gym PlanДокумент15 страницBuff Dudes 12 Week Home and Gym Planallan_gs100% (2)
- Balance Test - Standing Stork Test (Blind)Документ4 страницыBalance Test - Standing Stork Test (Blind)Boobesh Venkata RamananОценок пока нет
- 'T' Drill TestДокумент4 страницы'T' Drill TestBoobesh Venkata RamananОценок пока нет
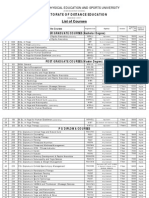
- Directorate of Distance Education List of Courses: Tamil Nadu Physical Education and Sports UniversityДокумент4 страницыDirectorate of Distance Education List of Courses: Tamil Nadu Physical Education and Sports UniversityBoobesh Venkata RamananОценок пока нет
- Syllabus - MBBSДокумент167 страницSyllabus - MBBStariqayubОценок пока нет
- Micro BiologyДокумент12 страницMicro BiologyBoobesh Venkata RamananОценок пока нет
- SRM BPT SyllabusДокумент151 страницаSRM BPT SyllabusBoobesh Venkata RamananОценок пока нет
- Essays For 12th StandardДокумент43 страницыEssays For 12th StandardBoobesh Venkata Ramanan0% (1)
- AsthmaДокумент6 страницAsthmaBoobesh Venkata RamananОценок пока нет
- B.tech Biotech III Yr I Sem - 0Документ18 страницB.tech Biotech III Yr I Sem - 0Boobesh Venkata RamananОценок пока нет
- School - Diagnosis of Genetic DisordersДокумент33 страницыSchool - Diagnosis of Genetic DisordersBoobesh Venkata Ramanan100% (1)
- Medicinal PlantsДокумент211 страницMedicinal PlantsDr-Abdulrahman GhonemОценок пока нет
- GWP - Unicef - Guidance Note Risk Assessments For Wash PDFДокумент56 страницGWP - Unicef - Guidance Note Risk Assessments For Wash PDFyomifОценок пока нет
- Geometry Solving Problems (Circles)Документ36 страницGeometry Solving Problems (Circles)Hero MirasolОценок пока нет
- 3B Adverbial PhrasesДокумент1 страница3B Adverbial PhrasesSarah IОценок пока нет
- Infanrix Hexa RSMKL July 2023Документ37 страницInfanrix Hexa RSMKL July 2023Bayu KurniawanОценок пока нет
- 2 - RUBRIC PHY110 (For Student)Документ3 страницы2 - RUBRIC PHY110 (For Student)Puteri AaliyyaОценок пока нет
- 2018 World Traumatic Dental Injury Prevalence and IncidenceДокумент16 страниц2018 World Traumatic Dental Injury Prevalence and IncidencebaridinoОценок пока нет
- Leading a Community Through Integrity and CourageДокумент2 страницыLeading a Community Through Integrity and CourageGretchen VenturaОценок пока нет
- Why Research Is Important in The BusinessДокумент2 страницыWhy Research Is Important in The BusinessBricx BalerosОценок пока нет
- OEO105020 LTE ERAN2.2 Connection Management Feature ISSUE 1.00Документ52 страницыOEO105020 LTE ERAN2.2 Connection Management Feature ISSUE 1.00Daniel YulistianОценок пока нет
- EY The Cfo Perspective at A Glance Profit or LoseДокумент2 страницыEY The Cfo Perspective at A Glance Profit or LoseAayushi AroraОценок пока нет
- Perkin Elmer Singapore Distribution CaseДокумент3 страницыPerkin Elmer Singapore Distribution CaseJackie Canlas100% (1)
- WORKSHOP ON ACCOUNTING OF IJARAHДокумент12 страницWORKSHOP ON ACCOUNTING OF IJARAHAkif ShaikhОценок пока нет
- Semi-Detailed Lesson Plan Template: Pagsanjan Intergrated National High School 8Документ3 страницыSemi-Detailed Lesson Plan Template: Pagsanjan Intergrated National High School 8Mae Ganate RoblesОценок пока нет
- Levenbach Causal2017Документ15 страницLevenbach Causal2017Jenna GrantОценок пока нет
- People vs. LorenzoДокумент8 страницPeople vs. LorenzoMRose SerranoОценок пока нет
- Think Like An EconomistДокумент34 страницыThink Like An EconomistDiv-yuh BothraОценок пока нет
- Adina CFD FsiДокумент481 страницаAdina CFD FsiDaniel GasparinОценок пока нет
- The Road To Privatization: TQM and Business Planning: Bennington, Lynne Cummane, JamesДокумент11 страницThe Road To Privatization: TQM and Business Planning: Bennington, Lynne Cummane, JamesBojan KovacevicОценок пока нет
- Benefits and Risks of Dexamethasone in Noncardiac Surgery: Clinical Focus ReviewДокумент9 страницBenefits and Risks of Dexamethasone in Noncardiac Surgery: Clinical Focus ReviewAlejandra VillaОценок пока нет
- Cambridge Assessment International Education: Biology 5090/61 October/November 2017Документ6 страницCambridge Assessment International Education: Biology 5090/61 October/November 2017Zarish NoorОценок пока нет
- Module 2 - Content and Contextual Analysis of Selected Primary andДокумент41 страницаModule 2 - Content and Contextual Analysis of Selected Primary andAngelica CaldeoОценок пока нет
- Summary Basis For Regulatory Action TemplateДокумент23 страницыSummary Basis For Regulatory Action TemplateAviseka AcharyaОценок пока нет
- IFRS 17 Risk Adjustment For Non-Financial Risk For Life and Health Insurance ContractsДокумент34 страницыIFRS 17 Risk Adjustment For Non-Financial Risk For Life and Health Insurance ContractsaljdummyОценок пока нет
- Nitrate Reduction in Sulfate Reducing BacteriaДокумент10 страницNitrate Reduction in Sulfate Reducing BacteriaCatalinaManjarresОценок пока нет
- Parashara'S Light 7.0.1 (C) Geovision Software, Inc., Licensed ToДокумент5 страницParashara'S Light 7.0.1 (C) Geovision Software, Inc., Licensed TobrajwasiОценок пока нет
- Untitled DocumentДокумент2 страницыUntitled DocumentClaudia WinОценок пока нет
- Modelling of Induction Motor PDFДокумент42 страницыModelling of Induction Motor PDFsureshОценок пока нет
- Kurukshetra English August '17Документ60 страницKurukshetra English August '17amit2688Оценок пока нет
- Blind and Visually ImpairedДокумент5 страницBlind and Visually ImpairedPrem KumarОценок пока нет
- Comprehension Used ToДокумент2 страницыComprehension Used TomarialecortezОценок пока нет