Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Duncan Richards and J. K. Aronson - Oxford Handbook of Practical Drug TherapyДокумент818 страницDuncan Richards and J. K. Aronson - Oxford Handbook of Practical Drug TherapyDavid100% (3)
- Global Pharmaceutical Contract Manufacturing Market InsightsДокумент26 страницGlobal Pharmaceutical Contract Manufacturing Market InsightsShahid ShoaibОценок пока нет
- Biosimilars Market Size, Trends and Forecast, 2026Документ7 страницBiosimilars Market Size, Trends and Forecast, 2026swati kaleОценок пока нет
- In Vitro Evaluation of Nasogastric Tube Delivery Performance of Esomeprazole MagnesiumДокумент14 страницIn Vitro Evaluation of Nasogastric Tube Delivery Performance of Esomeprazole MagnesiumJoana GasparОценок пока нет
- Reichert 2002Документ5 страницReichert 2002Joana GasparОценок пока нет
- Trends in Biotechnology Volume 27 Issue 7 2009 (Doi 10.1016 - J.tibtech.2009.03.005) Leyre Zuñiga Begoña Calvo - Regulatory Aspects of Biosimilars in EuropeДокумент3 страницыTrends in Biotechnology Volume 27 Issue 7 2009 (Doi 10.1016 - J.tibtech.2009.03.005) Leyre Zuñiga Begoña Calvo - Regulatory Aspects of Biosimilars in EuropeMohamedRefaatMohamedОценок пока нет
- Dendritic Cell-Based Vaccination in Cancer Therapeutic Implications Emerging From Murine ModelsДокумент18 страницDendritic Cell-Based Vaccination in Cancer Therapeutic Implications Emerging From Murine ModelsJoana GasparОценок пока нет
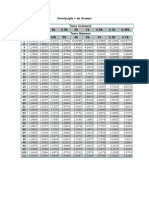
- Tabela T StudentДокумент1 страницаTabela T StudentJoana GasparОценок пока нет
- ICH Q2 R1 GuidelineДокумент17 страницICH Q2 R1 GuidelineRicard Castillejo HernándezОценок пока нет
- High-Efficiency Production of Bioactive Recombinant Human Fibroblast Growth Factor 18 in Escherichia Coli and Its Effects On Hair Follicle GrowthДокумент10 страницHigh-Efficiency Production of Bioactive Recombinant Human Fibroblast Growth Factor 18 in Escherichia Coli and Its Effects On Hair Follicle GrowthJoana GasparОценок пока нет
- Pharmaceuticals Executive SummaryДокумент10 страницPharmaceuticals Executive SummaryPradyot78Оценок пока нет
- Paras Biopharmaceuticals Finland Oy Announces Successful Development of Biologically Active Romiplostim (N-Plate® Biosimilar) Production TechnologyДокумент3 страницыParas Biopharmaceuticals Finland Oy Announces Successful Development of Biologically Active Romiplostim (N-Plate® Biosimilar) Production TechnologyPR.comОценок пока нет
- Program BiosimilarsДокумент4 страницыProgram BiosimilarsCecilia ChuiОценок пока нет
- CPGM 7345.848 - Inspection of Biological Drug ProductsДокумент20 страницCPGM 7345.848 - Inspection of Biological Drug ProductsKisho RamОценок пока нет
- Guide To Application For Registration of Medicinal Products - 4th EditiДокумент142 страницыGuide To Application For Registration of Medicinal Products - 4th EditiKdp03Оценок пока нет
- About: Mr. Ramanbhai B. Patel (Late)Документ6 страницAbout: Mr. Ramanbhai B. Patel (Late)9922779374Оценок пока нет
- Coverage Initiation - BioconДокумент32 страницыCoverage Initiation - BioconAjit AgrawalОценок пока нет
- Fundamentals of International Pharmaceutical and Biologics RegulationsДокумент296 страницFundamentals of International Pharmaceutical and Biologics RegulationsPranay GhiyaОценок пока нет
- Introduction To Biologics and BiosimilarsДокумент15 страницIntroduction To Biologics and BiosimilarsDinesh IitmОценок пока нет
- Pre-Filled Syringes 2014-2024 PDFДокумент24 страницыPre-Filled Syringes 2014-2024 PDFVisiongainGlobal0% (1)
- Annex 3 TRS 1011Документ99 страницAnnex 3 TRS 1011Anonymous RuVgQLОценок пока нет
- Credit Course Individual Desk I Pharmaceutical Manufacturing IndustryДокумент71 страницаCredit Course Individual Desk I Pharmaceutical Manufacturing IndustryKareem Ashraf RizkОценок пока нет
- Compensation ManagementДокумент27 страницCompensation ManagementGeetika apurvaОценок пока нет
- Biosimilars PathwayДокумент13 страницBiosimilars Pathwaytamara_0021Оценок пока нет
- OPTH-D-23-00561_R1 (2)Документ41 страницаOPTH-D-23-00561_R1 (2)shilpi.dhawan1973Оценок пока нет
- 12 - 268CPD-Biosimilar Drugs PDFДокумент6 страниц12 - 268CPD-Biosimilar Drugs PDFwasonoОценок пока нет
- Drreddys Investor Presentation June2015Документ34 страницыDrreddys Investor Presentation June2015Vu HauОценок пока нет
- FDA-approved List of BiosimilarsДокумент2 страницыFDA-approved List of BiosimilarsYoo AnОценок пока нет
- Biosimilar Current Status in India: Review ArticleДокумент4 страницыBiosimilar Current Status in India: Review ArticlebhupiscribdОценок пока нет
- 2020 - 03 - 23 - Sanofi Report 2019 20F AccessibleДокумент294 страницы2020 - 03 - 23 - Sanofi Report 2019 20F AccessibleJulian HutabaratОценок пока нет
- Schedule Ismi HottiДокумент23 страницыSchedule Ismi HottisigitОценок пока нет
- Biotech Firms, Billions at Risk, Lobby States To Limit GenericsДокумент2 страницыBiotech Firms, Billions at Risk, Lobby States To Limit Genericsdule83Оценок пока нет
- Need For Better Insulins and BiosimilarsДокумент57 страницNeed For Better Insulins and Biosimilarsnsk79in@gmail.comОценок пока нет
- Ncologist: Erythropoiesis-Stimulating Agents in Renal MedicineДокумент6 страницNcologist: Erythropoiesis-Stimulating Agents in Renal MedicineSergio RodriguezОценок пока нет
- Anticipated Availability of First-Time GenericsДокумент31 страницаAnticipated Availability of First-Time Genericssanjay28382Оценок пока нет
- Williams S. Ettouati, Pharm. D. Director, Industrial Relations & Development Health Sciences Associate Clinical Professor, N.SДокумент41 страницаWilliams S. Ettouati, Pharm. D. Director, Industrial Relations & Development Health Sciences Associate Clinical Professor, N.SRaghul BaskaranОценок пока нет
- US Pharmaceutical Industry Analysis: PEST Analysis, Trends, ForecastДокумент34 страницыUS Pharmaceutical Industry Analysis: PEST Analysis, Trends, ForecastphoboscaОценок пока нет