Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Factors Associated With Occasional and Recurrent Falls in Mexican Community-Dwelling Older PeopleДокумент12 страницFactors Associated With Occasional and Recurrent Falls in Mexican Community-Dwelling Older PeopleAlejandro GuzmanОценок пока нет
- MB - CM.SL.2018. Enciclopedia de Neuropsicología ClínicaДокумент3 848 страницMB - CM.SL.2018. Enciclopedia de Neuropsicología ClínicaAlejandro Guzman100% (5)
- HG - HG.JAGS.2020.68. Enfermedad de Coronavirus en Centros AsistencialesДокумент6 страницHG - HG.JAGS.2020.68. Enfermedad de Coronavirus en Centros AsistencialesAlejandro GuzmanОценок пока нет
- HG - HG.JASP.2020.32. Marco de Trabajo en Respuesta A COVID-19 PDFДокумент8 страницHG - HG.JASP.2020.32. Marco de Trabajo en Respuesta A COVID-19 PDFAlejandro GuzmanОценок пока нет
- Factors Associated With Occasional and Recurrent Falls in Mexican Community-Dwelling Older PeopleДокумент12 страницFactors Associated With Occasional and Recurrent Falls in Mexican Community-Dwelling Older PeopleAlejandro GuzmanОценок пока нет
- HG - MC.2018.102.03.13. Errores Diagnósticos Al Borde de La CamaДокумент12 страницHG - MC.2018.102.03.13. Errores Diagnósticos Al Borde de La CamaAlejandro GuzmanОценок пока нет
- HG - HG.REGG.2016.51. Medicina Del Estilo de Vida y Envejecimiento SaludableДокумент9 страницHG - HG.REGG.2016.51. Medicina Del Estilo de Vida y Envejecimiento SaludableAlejandro GuzmanОценок пока нет
- Envejecimiento Saludable A Través de Las Etapas Del EnvejecimientoДокумент10 страницEnvejecimiento Saludable A Través de Las Etapas Del EnvejecimientoAlejandro GuzmanОценок пока нет
- Efectos de La Parotina en Huesos LargosДокумент6 страницEfectos de La Parotina en Huesos LargosAlejandro GuzmanОценок пока нет
- Krauss 2016Документ16 страницKrauss 2016Alejandro GuzmanОценок пока нет
- 1 PDFДокумент11 страниц1 PDFJoeljar Enciso SaraviaОценок пока нет
- HG - HM.GG - Aa.2016.45.06. Associación Entre Limitaciones de Movilidad e Incidencia de DiscapacidadДокумент8 страницHG - HM.GG - Aa.2016.45.06. Associación Entre Limitaciones de Movilidad e Incidencia de DiscapacidadAlejandro GuzmanОценок пока нет
- J Mcna 2014 11 003Документ17 страницJ Mcna 2014 11 003Cristine Westphal KroonОценок пока нет
- HG - HM.JGMS.2017.72. Trayectorias Del Envejecimeinto SaludableДокумент7 страницHG - HM.JGMS.2017.72. Trayectorias Del Envejecimeinto SaludableAlejandro GuzmanОценок пока нет
- HG - HM.JGMS.2017.72. Trayectorias Del Envejecimeinto SaludableДокумент7 страницHG - HM.JGMS.2017.72. Trayectorias Del Envejecimeinto SaludableAlejandro GuzmanОценок пока нет
- Efectos de La Parotina en Huesos LargosДокумент6 страницEfectos de La Parotina en Huesos LargosAlejandro GuzmanОценок пока нет
- Valoración Geriátrica IntegralДокумент13 страницValoración Geriátrica IntegralBlackthestralОценок пока нет
- Prevention of Falls in Community Dwelling Older Adults NEJM 2020 PDFДокумент10 страницPrevention of Falls in Community Dwelling Older Adults NEJM 2020 PDFShatha WishahОценок пока нет
- Valoración Geriátrica IntegralДокумент13 страницValoración Geriátrica IntegralBlackthestralОценок пока нет
- J Mcna 2014 11 003Документ17 страницJ Mcna 2014 11 003Cristine Westphal KroonОценок пока нет
- Desai 2010Документ16 страницDesai 2010Alejandro GuzmanОценок пока нет
- Aging With Long-Term Mobility Impairment: Maintaining Activities of Daily Living Via Selection, Optimization, and CompensationДокумент11 страницAging With Long-Term Mobility Impairment: Maintaining Activities of Daily Living Via Selection, Optimization, and CompensationAlejandro GuzmanОценок пока нет
- Krauss 2016Документ16 страницKrauss 2016Alejandro GuzmanОценок пока нет
- A Review and Summary of The Impact of Malnutrition in Older People and The Reported Costs and Benefits of InterventionsДокумент30 страницA Review and Summary of The Impact of Malnutrition in Older People and The Reported Costs and Benefits of InterventionsAlejandro GuzmanОценок пока нет
- Tinetti Mobility Test Is Related To Muscle Mass and Strength in Non-Institutionalized Elderly PeopleДокумент9 страницTinetti Mobility Test Is Related To Muscle Mass and Strength in Non-Institutionalized Elderly PeopleAlejandro GuzmanОценок пока нет
- Defining Undernutrition (Malnutrition) in Older Persons: EditorialДокумент3 страницыDefining Undernutrition (Malnutrition) in Older Persons: EditorialAlejandro GuzmanОценок пока нет
- Geriatric Nursing: Shirley Musich, PHD, Shaohung S. Wang, PHD, Joann Ruiz, MPH, Kevin Hawkins, PHD, Ellen Wicker, MhaДокумент8 страницGeriatric Nursing: Shirley Musich, PHD, Shaohung S. Wang, PHD, Joann Ruiz, MPH, Kevin Hawkins, PHD, Ellen Wicker, MhaAlejandro GuzmanОценок пока нет
- ESPEN Guidelines On Definitions and Terminology of Clinical NutritionДокумент16 страницESPEN Guidelines On Definitions and Terminology of Clinical NutritionMarie GCОценок пока нет
- Oup Accepted Manuscript 2018Документ4 страницыOup Accepted Manuscript 2018Alejandro GuzmanОценок пока нет
- HG - HM.GG - Aa.2016.45.06. Associación Entre Limitaciones de Movilidad e Incidencia de DiscapacidadДокумент8 страницHG - HM.GG - Aa.2016.45.06. Associación Entre Limitaciones de Movilidad e Incidencia de DiscapacidadAlejandro GuzmanОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Test Bank For 3 2 1 Code It 2020 8th Edition Michelle Green Full DownloadДокумент24 страницыTest Bank For 3 2 1 Code It 2020 8th Edition Michelle Green Full Downloadrobertabergmjnxqrasct100% (43)
- History of LaparosДокумент27 страницHistory of LaparosDr. Sanjay KolteОценок пока нет
- LB Surgical Fire PosterДокумент1 страницаLB Surgical Fire Poster979104025Оценок пока нет
- Diabetic Retinopathy Screening ModuleДокумент96 страницDiabetic Retinopathy Screening ModuleSehaRizaОценок пока нет
- Obstetric History and Physical Examination (Ina Irabon)Документ49 страницObstetric History and Physical Examination (Ina Irabon)Benjamin Gabriel100% (1)
- Resume Tugas Akademik 8-Journal Reading 5-REFДокумент3 страницыResume Tugas Akademik 8-Journal Reading 5-REFRaissaОценок пока нет
- Inventory List at in Emergei (Cy: PrsentДокумент1 страницаInventory List at in Emergei (Cy: PrsentVirginia BennettОценок пока нет
- Mallory Brearey-Resume 2021 1Документ2 страницыMallory Brearey-Resume 2021 1api-507675724Оценок пока нет
- BW Health-5Документ2 страницыBW Health-5Michael JaballasОценок пока нет
- Assessment of Knowledge Attitude and Practice On Emergency Contraceptive Among Goba Female High School and Preparatory StudentsДокумент9 страницAssessment of Knowledge Attitude and Practice On Emergency Contraceptive Among Goba Female High School and Preparatory StudentsLawrence MungaОценок пока нет
- Treatments For OsteoporosisДокумент2 страницыTreatments For Osteoporosisawaw90Оценок пока нет
- Residency Prog CanadaДокумент116 страницResidency Prog Canadahswami20037730Оценок пока нет
- The Exotic Pet Consultation: History TakingДокумент3 страницыThe Exotic Pet Consultation: History TakingDavid PGОценок пока нет
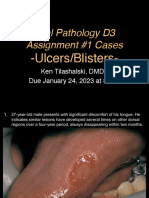
- D3 Ulcers Blisters Cases Due01242023 8amДокумент13 страницD3 Ulcers Blisters Cases Due01242023 8amLinh PhanОценок пока нет
- Active VFC ProvidersДокумент50 страницActive VFC ProvidersClint AnthonyОценок пока нет
- 2021 Abbott Annual ReportДокумент86 страниц2021 Abbott Annual ReportAdriano BolgenhagenОценок пока нет
- Prevalence and Recurrence Rate of Perianal Abscess - A Population-Based Study, Sweden 1997 - 2009Документ5 страницPrevalence and Recurrence Rate of Perianal Abscess - A Population-Based Study, Sweden 1997 - 2009Ridha Aswina DalimuntheОценок пока нет
- MKT 6080 Final Project Milestone 2 WorksheetДокумент12 страницMKT 6080 Final Project Milestone 2 WorksheetDEEОценок пока нет
- NF) S ) JF Cfof) U G) Kfn:Jf:Yo ) JF, HG/N GL (Ë D"X, Xfos KFFRF) + Tx,:6Fkm G (KBSF) V'NNF / CFGTL/S K - Ltof) Lutftds LNLVT K/Liffsf) Kf7/OqmdДокумент4 страницыNF) S ) JF Cfof) U G) Kfn:Jf:Yo ) JF, HG/N GL (Ë D"X, Xfos KFFRF) + Tx,:6Fkm G (KBSF) V'NNF / CFGTL/S K - Ltof) Lutftds LNLVT K/Liffsf) Kf7/OqmdAnil BasnetОценок пока нет
- Special Report: Solutions For Joint and Arthritic Pain: by Jon Benson Author, Fit Over 40Документ21 страницаSpecial Report: Solutions For Joint and Arthritic Pain: by Jon Benson Author, Fit Over 40tobyОценок пока нет
- Science 9 Quarter 1 Week 2 Sim 3Документ30 страницScience 9 Quarter 1 Week 2 Sim 3Jelly FloresОценок пока нет
- Adelekan and OyelamiДокумент8 страницAdelekan and OyelamiAdemola AdelekanОценок пока нет
- Reporte 2020 de La Oficina de Asuntos Globales de Estados UnidosДокумент72 страницыReporte 2020 de La Oficina de Asuntos Globales de Estados UnidosAristegui NoticiasОценок пока нет
- Sybil Williams Resume 2Документ2 страницыSybil Williams Resume 2api-248728180Оценок пока нет
- UNIT 1A. Assessing Community NeedsДокумент116 страницUNIT 1A. Assessing Community NeedsSebastianОценок пока нет
- Management of Abnormal Uterine Bleeding With Emphasis On Alternatives To HyterectomyДокумент16 страницManagement of Abnormal Uterine Bleeding With Emphasis On Alternatives To HyterectomyEstefania gonzalez torresОценок пока нет
- NCP - Pain Related To Surgical Incision (Mark)Документ4 страницыNCP - Pain Related To Surgical Incision (Mark)KM57% (21)
- Oral Habits and Its Relationship To Malocclusion A Review.20141212083000Документ4 страницыOral Habits and Its Relationship To Malocclusion A Review.20141212083000Stacia AnastashaОценок пока нет
- Joanne Marie Gomez ManaliliДокумент4 страницыJoanne Marie Gomez ManaliliJaira Marie Gomez Manalili100% (1)
- Drug DevelopmentДокумент96 страницDrug DevelopmentSheena GagarinОценок пока нет